



-
自2019年12月以来,多起原因不明的病毒性肺炎在全世界流行,研究人员通过对下呼吸道样本的深度测序分析,很快确认本次疫情是由一种新型冠状病毒引起的[1-2]。世界卫生组织将这种新型冠状病毒感染引起的疾病命名为新型冠状病毒肺炎(corona virus disease 2019,COVID-19)[3]。COVID-19是一种新型包膜RNA冠状病毒(正冠状病毒亚科沙贝病毒亚属),传染性较强[4]。采用实时聚合酶链反应(real-time polymerase chain reaction, RT-PCR)快速建立了COVID-19特异性病毒核酸检测的方法[5-6],但研究结果表明,CT对COVID-19的诊断灵敏度(97%)高于RT-PCR(30%~60%)[7]。CT可以识别RT-PCR检测结果为阴性但高度怀疑为COVID-19的患者[8-9]。因此,在COVID-19快速传播的过程中,CT在COVID-19的诊断、严重程度判断和控制方面发挥着尤为重要的作用。在COVID-19患者中,多数患者为普通型,因此,我们分析了无锡市第五人民医院收治的50例普通型COVID-19患者的临床和胸部CT表现,以期为COVID-19的鉴别诊治提供理论依据。
-
回顾性分析2020年1至4月在无锡市第五人民医院诊治的50例普通型COVID-19患者的CT资料。所有患者均按照世界卫生组织指南[10],应用RT-PCR对咽拭子标本进行新型冠状病毒核酸检测,结果为阳性,且均符合《新型冠状病毒肺炎诊疗方案(试行第八版 修订版)》[11]中对 COVID-19的普通型患者的诊断标准。患者的临床数据,包括流行病学调查结果、临床表现、实验室检测结果和其他伴随条件或疾病,均由2名经验丰富的中级职称以上的临床医师收集。该研究得到了无锡市第五人民医院伦理委员会的批准(批准号:无锡五院论文伦字第2021-002-1)。
-
采用德国西门子SOMATOM Definition AS (Siemens Healthcare)螺旋CT扫描仪对患者的胸部进行扫描。患者均取仰卧位,抬起手臂,吸气结束时屏住呼吸。扫描范围从肺尖到肺底。采集参数:管电压为120 kV,自动管电流;矩阵为512×512;层厚为7 mm,薄层重建厚度为1 mm。
-
由2位经验丰富的中级以上职称的放射科医师采用盲法分别在PACS工作站上(Skyview,南京长江瑞亨软件有限公司)使用多平面重建工具对CT薄层图像进行独立分析,采用肺窗(窗宽1200 HU、窗位−600 HU)和纵隔窗(窗宽350 HU、窗位50 HU)的设置,并对分析结果达成一致,如意见不统一时,由第3位主任医师审核结果,并做最终决定。肺病变的分布可分为外周型(以胸膜下为主,主要累及肺外周的1/3)、中央型(以肺门为主,主要累及肺中央的2/3)和外周加中央型,肺叶累及范围分为单叶和多叶,主要的CT征象有磨玻璃影(ground-glass opacity, GGO)[12]、实变、铺路石征[13]、网格样改变、空泡征,增粗血管征(微血管扩张)、纤维条索、胸膜下线(2~5 cm长的弯曲致密影)、空气支气管征、支气管扭曲(小支气管分支弯曲)、胸膜增厚,胸膜牵拉、胸腔积液。根据以往对中东呼吸综合征(Middle East respiratory syndrome,MERS)和严重急性呼吸综合征(severe acute respiratory syndrome,SARS) CT显像的研究[14-17],将肺分为上区(隆凸以上)、中区(气管隆突下缘至下肺静脉干下缘)和下区(下肺静脉干下缘以下);本研究中又将这3个区域分别分为2个区域:前区域(矢状位横隔胸膜垂直中点前面的区域)和后区域(矢状位横隔胸膜垂直中点后面的区域);因此双侧肺总共分为12个肺区。各肺区受累情况评分标准为:0分,未受累;1分,<25%受累;2分,25%~50%受累;3分,50%~75%受累;4分,≥75%受累。
-
采用SPSS19.0软件对数据进行统计分析。对计量资料行Kolmogorov-Smirnov检验确定是否符合正态分布,符合正态分布的连续变量以
$ \bar x \pm s $ 表示;非正态分布的计量资料用M(Q1,Q3)表示,采用Mann-Whitney U检验。计数资料[以数量(百分比)表示]的比较采用卡方检验。P<0.05为差异有统计学意义。 -
50例COVID-19患者中,男性患者年龄为(39.2±20.9)岁,女性患者年龄为(37.1±18.6)岁。其中,17例患者(34%)曾去过武汉,23例(46%)接触过确诊患者,10例(20%)的暴露史未知。在这些患者中,24例患者(48%)咳嗽,9例(18%)发烧,5例(10%)有乏力症状。其他症状有胸闷、咳痰、咽痛和腹泻。50例患者中有17例(34%)无明显症状。患者的临床表现见表1。
临床表现 患者 (n=50) 暴露史 14 d内有武汉旅居史 17(34) 14 d内有与确诊患者接触史 23(46) 未知 10(20) 症状 发烧 24(48) 咳嗽 9(18) 乏力 5(10) 肌肉痛 1(2) 胸闷 2(4) 咳痰 2(4) 咽痛 1(2) 腹泻 2(4) 无明显症状 17(34) 伴随疾病 高血压 9(18) 糖尿病 2(4) 冠心病 1(2) 癫痫 1(2) 恶性肿瘤 2(4) 十二指肠溃疡 1(2) 精神分裂症 1(2) 手术史 6(12) 表 1 50例普通型新型冠状病毒肺炎患者的临床表现[例(%)]
Table 1. Clinical characteristics of 50 patients with common novel corona virus disease 2019 (case (%))
-
大部分普通型患者的实验室检查结果在正常范围内(表2)。2例患者(4%)白细胞减少,13例患者(26%)淋巴细胞计数下降,7例患者(14%)淋巴细胞百分比下降,12例患者(24%)超敏C反应蛋白(hypersensitive C-reactive protein,hs-CRP)水平升高。其他异常包括d-二聚体(18%)、谷丙转氨酶(26%)、天冬氨酸转氨酶(10%)、肌酐(26%)、肌酸激酶(14%)和尿素(8%)水平升高。
项目 患者(n=50) 白细胞计数 升高 0 降低 2(4) 正常 48(96) 淋巴细胞计数 升高 2(4) 降低 13(26) 正常 35(70) 淋巴细胞百分比 升高 5(10) 降低 7(14) 正常 38(76) 超敏C反应蛋白 升高 12(24) 正常 38(76) d-二聚体 升高 9(18) 正常 41(82) 谷丙转氨酶 升高 13(26) 降低 1(2) 正常 36(72) 天冬氨酸转氨酶 升高 5(10) 正常 45(90) 肌酐 升高 13(26) 降低 7(14) 正常 30(60) 肌酸激酶 升高 7(14) 降低 1(2) 正常 42(84) 尿素 升高 4(8) 降低 2(4) 正常 44(88) 表 2 50例普通型新型冠状病毒肺炎患者的实验室检查结果[例(%)]
Table 2. Laboratory test results of 50 patients with common novel corona virus disease 2019 (case (%))
-
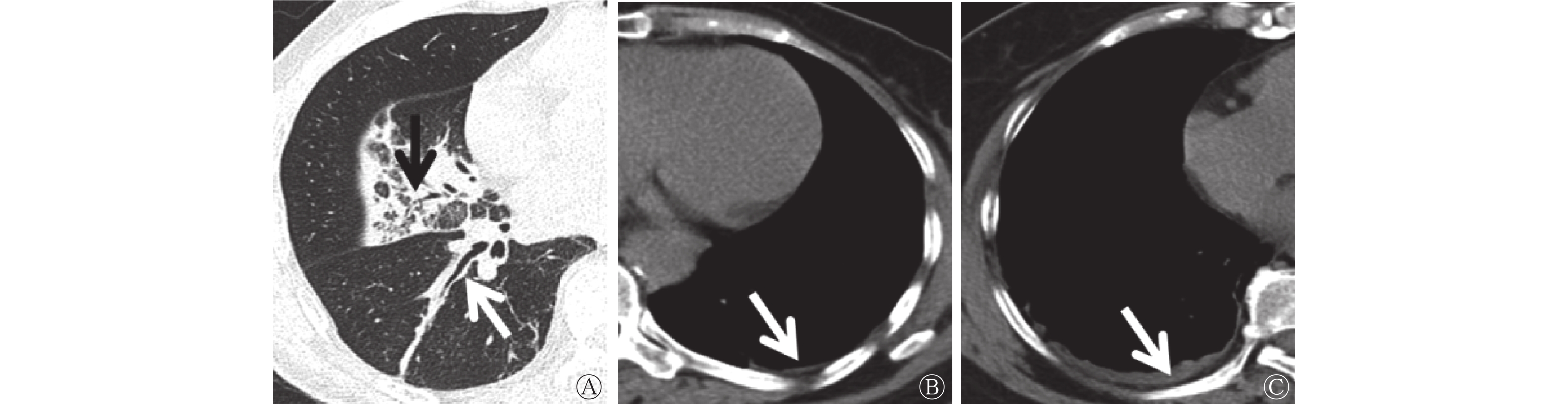
50例普通型COVID-19患者的CT表现包括肺、支气管及胸膜病变(图1、2)。肺部病变方面,CT示GGO 26例(52%)、实变7例(14%)、铺路石征16例(32%)、空泡征3例(6%)、微血管扩张征3例(6%)、纤维条索7例(14%)、胸膜下线2例(4%)。支气管病变包括空气支气管征3例(6%)、支气管扭曲1例(2%)。胸膜改变有胸膜增厚2例(4%)、胸腔积液1例(2%)。

图 1 5例普通型新型冠状病毒肺炎患者肺部改变的CT图
Figure 1. CT features of lung changes in 5 patients with common novel corona virus disease 2019

图 2 3例普通型新型冠状病毒肺炎患者支气管胸膜改变的CT图
Figure 2. CT features of bronchial and pleural changes in 3 patients with common novel corona virus disease 2019
-
由表3可知,从胸部CT所见病灶分布来看,50例患者中32例(64%)以外周为主,4例(8%)外周加中央,其余14例(28%)无病灶,三者间的差异有统计学意义(χ2=24.16,P<0.001),典型病例图见图3。多数患者表现为双侧多叶病变(24例,48%)。左、右肺CT评分差异无统计学意义(χ2=−0.586,P=0.558),下区CT评分高于中、上区(H=6.917,P=0.031),后区CT评分显著高于前区(H=−4.096,P=0.003)。

图 3 1例普通型新型冠状病毒肺炎患者肺部病变分布情况CT图 患者男性,48岁,A示双肺多发病灶累及多叶;B、C示后区病变较严重。CT为计算机体层摄影术
Figure 3. Distribution of pulmonary lesions in 1 patient with common novel corona virus disease 2019
项目 患者
[例(%)]CT 评分
[M(Q1,Q3)]检验值 P值 病灶分布 χ2=24.16 <0.001 无病灶 14(28) − 外周为主 32(64) − 外周加中央为主 4(8) − 累及肺叶 χ2=18.16 <0.001 未累及 14(28) − 单叶 8(16) − 单侧多叶 4(8) − 双侧多叶 24(48) − 左右肺累及 χ2=−0.586 0.558 左侧 32(64) 1(0,2) 右侧 29(58) 1(0,2) 肺的分区 上区 17(34) 0(0,1) H=6.917 0.031 中区 21(42) 0(0,1) 下区 30(60) 1.5(0,2) 前区 16(32) 0(0,1) H=−4.096 0.003 后区 34(68) 1.5(0,3) 注:−表示无此项数据。CT为计算机体层摄影术 表 3 50例普通型新型冠状病毒肺炎患者肺部病变分布及CT评分
Table 3. Distribution and CT score of the pulmonary lesions of 50 patients with common novel corona virus disease 2019
-
自2019年12月以来, COVID-19由于其传染性强、人群普遍易感,在全球引起了大流行。截至2022年1月30日,中国国内的COVID-19确诊患者达138 396例,而海外确诊患者高达3.7亿例。根据国家卫生健康委员会发布的《新型冠状病毒肺炎诊疗方案(试行第八版 修订版)》修订要点[11],可将患者分为轻型、普通型、重型、危重型4类。在本研究中,我们评估和分析了50例普通型COVID-19患者的基本流行病学调查结果、临床数据和CT图像表现。胸部CT的典型表现有助于早期筛查疑似疾病患者。
本研究中的50例普通型COVID-19患者大多曾去过武汉或与确诊患者有过接触史,该结果验证了人与人之间的传播性[18-19]。因此,及早发现患者,将健康人群与COVID-19患者区分开来,从而减少人与人之间的传播是非常重要的。普通型COVID-19患者以发热、咳嗽为主,部分患者无症状。对于大多数普通型COVID-19患者,实验室检查结果显示大部分正常,而淋巴细胞计数下降的患者占26%,淋巴细胞百分比下降的患者占14%,hs-CRP水平升高的患者占24%。这与其他研究结果一致,说明hs-CRP水平升高和淋巴细胞计数减少是COVID-19灵敏的标志物[20]。只有少数患者出现凝血功能、肝肾功能指标等其他实验室检查结果异常。
胸部CT在疑似COVID-19患者的确诊诊断中具有重要作用,有助于早期发现肺部异常,可用于筛查高度可疑的COVID-19患者,特别是RT-PCR初步筛查结果为阴性的患者。在本研究中,典型的CT图像表现主要有GGO、铺路石征和实变。这些结果与其他肺部病毒感染的CT图像表现一致,如SARS[13, 21]。由于发病机制相似,大多数病毒性肺炎在同一病毒科[22]中具有相似的影像表现。新型冠状病毒属于冠状病毒家族[23],因此,其与SARS病毒和MERS病毒感染具有相似的影像表现。在本研究中我们发现,普通COVID-19患者的支气管及胸膜改变的发生率较低。最近的一项研究报道,非急症(轻型和普通)COVID-19患者的支气管源性囊肿和胸膜改变的发生率低于急症(严重型和致命型)患者[24],这与我们的研究结果一致。
通过本研究我们发现,在肺部病变分布方面,普通型COVID-19患者肺部的病变主要分布在外周(64%)、双侧(48%)、下区(60%)、后区(68%),与以往研究结果相似[2, 22];此外,下区和后区的CT评分也明显高于其他区,因为病毒更有可能侵入细支气管和肺泡,进而引起免疫细胞参与的炎症反应。肺外周及肺下段的血管、淋巴管含有较多的免疫细胞,故病灶多分布于外周及肺下段[25]。
不过,我们目前的研究还存在一些局限性:(1)只收集了少数普通型COVID-19患者的数据,所以得到的CT图像结果可能存在偏倚;(2)未对患者胸部CT表现进行随访,因此未能追踪疾病的转归情况;(3)CT改变与临床表现的关系未被探讨,而这可能有助于监测和预测预后,为临床治疗提供依据;(4)未收集轻、重症患者的胸部CT影像和临床表现,未能更全面地评估COVID-19患者的CT影像变化。(5)根据现有研究结果,大多数患者会出现红细胞沉降率升高,但本研究未收集相关的检测结果。
综上所述,普通型COVID-19患者在武汉有明确的暴露史或与确诊患者接触史。普通型COVID-19患者的临床症状主要为发热、咳嗽,部分患者无症状。普通型COVID-19患者多数实验室检查结果正常,部分患者表现为淋巴细胞计数、淋巴细胞百分比下降,hs-CRP水平升高,典型的影像表现主要为GGO、铺路石征、实变,而支气管及胸膜改变的发生率较低。且普通COVID-19患者多为外周分布、双侧受累、下肺、后区、多灶分布。
利益冲突 所有作者声明无利益冲突
作者贡献声明 耿闯负责论文的撰写;龚红霞负责数据的收集、论文的审阅;邱晶负责数据的统计与分析;顾岚负责论文的审阅
50例普通型新型冠状病毒肺炎患者临床及胸部CT表现的分析
Clinical and chest CT manifestations of 50 patients with common novel corona virus disease 2019
-
摘要:
目的 分析50例普通型新型冠状病毒肺炎(COVID-19)患者的流行病学、临床、实验室检测结果及胸部CT表现,为临床诊治提供理论依据。 方法 回顾性分析2020年1至4月于无锡市第五人民医院经实时聚合酶链反应对咽拭子标本检查结果为阳性的50例普通型COVID-19患者[其中,男性26例、女性24例,年龄(38.2±19.6)岁]的临床数据和CT资料;同时对患者行薄层胸部CT扫描多平面重建以观察患者的肺部改变,对各肺区受累情况进行评分。计量资料的比较采用Mann-Whitney U检验。计数资料的比较采用卡方检验。 结果 50例普通型COVID-19患者中,40例患者(80%)曾到过武汉或与确诊患者有过接触史,17例(34%)无明显症状,38例(76%)主要表现为发热、咳嗽、乏力。实验室检查结果多数在正常范围内,部分患者出现淋巴细胞计数下降、超敏C反应蛋白水平升高、淋巴细胞百分比下降。典型CT表现主要为磨玻璃影、铺路石征、实变,且肺组织病变以周围型为主,双侧多叶分布。肺前区CT评分明显低于后区(H=−4.096,P=0.003),中、上区CT评分低于下区(H=6.917,P=0.031)。 结论 普通型COVID-19患者的临床表现可能不明显,实验室检查结果可能无明显异常,而胸部CT的改变比较明显,因此临床诊治过程中应充分结合患者胸部CT的表现,密切关注胸部CT的动态变化。 -
关键词:
- 新型冠状病毒肺炎 /
- 体层摄影术,X线计算机 /
- 临床表现
Abstract:Objectives To analyze the epidemiological, clinical, laboratory test results, and chest CT features of 50 patients with common novel corona virus disease 2019 (COVID-19), so as to provide a theoretical basis for clinical diagnosis and treatment. Methods The clinical manifestations and CT image findings of 50 patients with common novel COVID-19 (including 26 males and 24 females, aged (38.2±19.6) years) who were positive in throat swab samples by real-time polymerase chain reaction in Wuxi Fifth People's Hospital from January to April 2020 were collected and studied retrospectively. In addition, the patients were scanned with thin-layer chest CT and multiplanar reconstruction to observe the changes in their lungs, and the involvement of each lung area was scored. The measurement data were compared by using the Mann-Whitney U test. The Chi-square test was used to compare counting data. Results Of the 50 patients with common novel COVID-19, 40 patients (80%) had been to Wuhan or had a history of contact with confirmed patients, 17 patients (34%) had no evident symptoms, and 38 patients (76%) were primarily characterized by fever, cough and fatigue. The results of laboratory tests are mostly within the normal range, and some patients have shown decreased lymphocyte count, increased level of hypersensitive C-reactive protein, and decreased percentage of lymphocytes. Typical CT manifestations primarily include ground-glass shadow, paving stone sign and consolidation, and lung tissue lesions are primarily of peripheral type, with bilateral lobular distribution. The CT score of the anterior lung area was significantly lower than that of the posterior lung area (H=−4.096, P=0.003), and the CT score of the middle and upper lung area was lower than that of the lower lung area (H=6.917, P=0.031). Conclusions Patients with common novel COVID-19 may not have evident clinical manifestations, and their laboratory results may have no obvious abnormalities, but the change in chest CT is relatively evident. Therefore, patient's chest CT performance and dynamic changes in chest CT should be combined to obtain accurate clinical diagnosis and treatment. -
Key words:
- COVID-19 /
- Tomography, X-ray computed /
- Clinical features
-
图 1 5例普通型新型冠状病毒肺炎患者肺部改变的CT图
Figure 1. CT features of lung changes in 5 patients with common novel corona virus disease 2019
图 2 3例普通型新型冠状病毒肺炎患者支气管胸膜改变的CT图
Figure 2. CT features of bronchial and pleural changes in 3 patients with common novel corona virus disease 2019
图 3 1例普通型新型冠状病毒肺炎患者肺部病变分布情况CT图 患者男性,48岁,A示双肺多发病灶累及多叶;B、C示后区病变较严重。CT为计算机体层摄影术
Figure 3. Distribution of pulmonary lesions in 1 patient with common novel corona virus disease 2019
表 1 50例普通型新型冠状病毒肺炎患者的临床表现[例(%)]
Table 1. Clinical characteristics of 50 patients with common novel corona virus disease 2019 (case (%))
临床表现 患者 (n=50) 暴露史 14 d内有武汉旅居史 17(34) 14 d内有与确诊患者接触史 23(46) 未知 10(20) 症状 发烧 24(48) 咳嗽 9(18) 乏力 5(10) 肌肉痛 1(2) 胸闷 2(4) 咳痰 2(4) 咽痛 1(2) 腹泻 2(4) 无明显症状 17(34) 伴随疾病 高血压 9(18) 糖尿病 2(4) 冠心病 1(2) 癫痫 1(2) 恶性肿瘤 2(4) 十二指肠溃疡 1(2) 精神分裂症 1(2) 手术史 6(12)  下载: 导出CSV
下载: 导出CSV
表 2 50例普通型新型冠状病毒肺炎患者的实验室检查结果[例(%)]
Table 2. Laboratory test results of 50 patients with common novel corona virus disease 2019 (case (%))
项目 患者(n=50) 白细胞计数 升高 0 降低 2(4) 正常 48(96) 淋巴细胞计数 升高 2(4) 降低 13(26) 正常 35(70) 淋巴细胞百分比 升高 5(10) 降低 7(14) 正常 38(76) 超敏C反应蛋白 升高 12(24) 正常 38(76) d-二聚体 升高 9(18) 正常 41(82) 谷丙转氨酶 升高 13(26) 降低 1(2) 正常 36(72) 天冬氨酸转氨酶 升高 5(10) 正常 45(90) 肌酐 升高 13(26) 降低 7(14) 正常 30(60) 肌酸激酶 升高 7(14) 降低 1(2) 正常 42(84) 尿素 升高 4(8) 降低 2(4) 正常 44(88)
下载: 导出CSV
表 3 50例普通型新型冠状病毒肺炎患者肺部病变分布及CT评分
Table 3. Distribution and CT score of the pulmonary lesions of 50 patients with common novel corona virus disease 2019
项目 患者
[例(%)]CT 评分
[M(Q1,Q3)]检验值 P值 病灶分布 χ2=24.16 <0.001 无病灶 14(28) − 外周为主 32(64) − 外周加中央为主 4(8) − 累及肺叶 χ2=18.16 <0.001 未累及 14(28) − 单叶 8(16) − 单侧多叶 4(8) − 双侧多叶 24(48) − 左右肺累及 χ2=−0.586 0.558 左侧 32(64) 1(0,2) 右侧 29(58) 1(0,2) 肺的分区 上区 17(34) 0(0,1) H=6.917 0.031 中区 21(42) 0(0,1) 下区 30(60) 1.5(0,2) 前区 16(32) 0(0,1) H=−4.096 0.003 后区 34(68) 1.5(0,3) 注:−表示无此项数据。CT为计算机体层摄影术
下载: 导出CSV
-
[1] Zhu N, Zhang DY, Wang WL, et al. A novel coronavirus from patients with pneumonia in China, 2019[J]. N Engl J Med, 2020, 382(8): 727−733. DOI: 10.1056/NEJMoa2001017. [2] Huang CL, Wang YM, Li XW, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China[J]. Lancet, 2020, 395(10223): 497−506. DOI: 10.1016/S0140-6736(20)30183-5. [3] Sohrabi C, Alsafi Z, O'Neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19)[J]. Int J Surg, 2020, 76: 71−76. DOI: 10.1016/j.ijsu.2020.02.034. [4] Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China[J]. N Engl J Med, 2020, 382(18): 1708−1720. DOI: 10.1056/NEJMoa2002032. [5] Corman VM, Landt O, Kaiser M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR[J]. Euro Surveill, 2020, 25(3): 2000045. DOI: 10.2807/1560-7917.ES.2020.25.3.2000045. [6] Fang YC, Zhang HQ, Xie JC, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR[J]. Radiology, 2020, 296(2): E115−E117. DOI: 10.1148/radiol.2020200432. [7] Ai T, Yang ZL, Hou HY, et al. Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases[J]. Radiology, 2020, 296(2): E32−E40. DOI: 10.1148/radiol.2020200642. [8] Huang PK, Liu TZ, Huang LS, et al. Use of chest CT in combination with negative RT-PCR assay for the 2019 novel coronavirus but high clinical suspicion[J]. Radiology, 2020, 295(1): 22−23. DOI: 10.1148/radiol.2020200330. [9] Xie XZ, Zhong Z, Zhao W, et al. Chest CT for typical coronavirus disease 2019 (COVID-19) pneumonia: relationship to negative RT-PCR testing[J]. Radiology, 2020, 296(2): E41−E45. DOI: 10.1148/radiol.2020200343. [10] World Health Organization. Technical-guidance for 2019-nCoV RT-PCR[EB/OL]. [2022-02-22]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance. [11] 国家卫生健康委员会. 《新型冠状病毒肺炎诊疗方案(试行第八版 修订版)》修订要点[EB/OL]. (2021-04-15)[2022-02-22]. http://www.nhc.gov.cn/yzygj/s7652m/202104/f602891840954b08949fa7914b5c9a80.shtml.
National Health Commission key points for revision of diagnosis and treatment plan for novel coronavirus pneumonia (trial implementation of the eighth revision)[EB/OL]. (2021-04-15)[2022-02-22]. http://www.nhc.gov.cn/yzygj/s7652m/202104/f602891840954b08949fa7914b5c9a80.shtml.[12] Joynt GM, Antonio GE, Lam P, et al. Late-stage adult respiratory distress syndrome caused by severe acute respiratory syndrome: abnormal findings at thin-section CT[J]. Radiology, 2004, 230(2): 339−346. DOI: 10.1148/radiol.2303030894. [13] Wong KT, Antonio GE, Hui DSC, et al. Thin-section CT of severe acute respiratory syndrome: evaluation of 73 patients exposed to or with the disease[J]. Radiology, 2003, 228(2): 395−400. DOI: 10.1148/radiol.2283030541. [14] Ooi GC, Khong PL, Müller NL, et al. Severe acute respiratory syndrome: temporal lung changes at thin-section CT in 30 patients[J]. Radiology, 2004, 230(3): 836−844. DOI: 10.1148/radiol.2303030853. [15] Das KM, Lee EY, Langer RD, et al. Middle East respiratory syndrome coronavirus: what does a radiologist need to know?[J]. AJR Am J Roentgenol, 2016, 206(6): 1193−1201. DOI: 10.2214/AJR.15.15363. [16] Chang YC, Yu CJ, Chang SC, et al. Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: evaluation with thin-section CT[J]. Radiology, 2005, 236(3): 1067−1075. DOI: 10.1148/radiol.2363040958. [17] Chung M, Bernheim A, Mei XY, et al. CT imaging features of 2019 novel coronavirus (2019-nCoV)[J]. Radiology, 2020, 295(1): 202−207. DOI: 10.1148/radiol.2020200230. [18] Chen NS, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study[J]. Lancet, 2020, 395(10223): 507−513. DOI: 10.1016/S0140-6736(20)30211-7. [19] Chan JFW, Yuan SF, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster[J]. Lancet, 2020, 395(10223): 514−523. DOI: 10.1016/S0140-6736(20)30154-9. [20] Zhou SC, Wang YJ, Zhu TT, et al. CT features of coronavirus disease 2019 (COVID-19) pneumonia in 62 patients in Wuhan, China[J]. AJR Am J Roentgenol, 2020, 214(6): 1287−1294. DOI: 10.2214/AJR.20.22975. [21] Gao F, Li M, Ge XJ, et al. Multi-detector spiral CT study of the relationships between pulmonary ground-glass nodules and blood vessels[J]. Eur Radiol, 2013, 23(12): 3271−3277. DOI: 10.1007/s00330-013-2954-3. [22] Koo HJ, Lim S, Choe J, et al. Radiographic and CT features of viral pneumonia[J]. Radiographics, 2018, 38(3): 719−739. DOI: 10.1148/rg.2018170048. [23] Pan YB, Li XR, Yang G, et al. Serological immunochromatographic approach in diagnosis with SARS-CoV-2 infected COVID-19 patients[J]. J Infect, 2020, 81(1): e28−e32. DOI: 10.1016/j.jinf.2020.03.051. [24] Zhao W, Zhong Z, Xie XZ, et al. Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: a multicenter study[J]. AJR Am J Roentgenol, 2020, 214(5): 1072−1077. DOI: 10.2214/AJR.20.22976. [25] Zhou SC, Zhu TT, Wang YJ, et al. Imaging features and evolution on CT in 100 COVID-19 pneumonia patients in Wuhan, China[J]. Eur Radiol, 2020, 30(10): 5446−5454. DOI: 10.1007/s00330-020-06879-6. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 4840
- HTML全文浏览量: 3858
- PDF下载量: 17
