



-
目前调强放疗已成为非小细胞肺癌(non-small cell lung cancer,NSCLC)重要的治疗手段之一,该技术可以在保障靶区剂量准确的情况下尽可能降低正常组织的受照剂量[1-2]。但放疗后,部分患者仍然会发生放射性肺损伤这一常见并发症[3],从而延长了患者的康复时间,增加了患者的治疗成本[4],因此,探索发生放射性肺损伤的危险因素具有实际应用价值。本研究对行调强放疗的216例局部晚期NSCLC患者的临床资料进行分析,筛选发生急性放射性肺损伤的危险因素并建立预测发生风险的列线图模型,为局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的防治提供依据。
-
回顾性分析2017年5月至2019年11月于南京医科大学附属脑科医院(胸科院区)放疗科行调强放疗的216例局部晚期NSCLC患者的临床资料,其中男性94例、女性122例,年龄37~83(61.5±9.6)岁 。纳入标准:(1)临床资料完整;(2)年龄>18岁;(3)经组织病理学检查确诊为ⅢA、ⅢB期NSCLC;(4)采取根治性调强放疗的初始NSCLC患者;(5)未行同步化疗;(6)放疗总剂量为45~77 Gy。排除标准:(1)预计生存期<3个月;(2)正在参与其他临床试验;(3)中途退出治疗。所有患者均在检查前签署了知情同意书。本研究获得南京医科大学附属脑科医院伦理委员会的批准[批准号:南医伦审(2016)第(034)号]。
样本量验证采用样本量计算公式n=[(Ζα/2)2×P×(1−P)]/(δ2×deff),式中,n为样本量,Ζα/2为1.96,P为阳性率估计值,P×(1−P)最大为0.25,δ为最大允许误差,deff为设计效应值。在90%CI下,绝对误差为10%的情况下设计效应值为50%,则抽样估算样本量为192例,应接触样本量为192例,故本研究纳入的样本量充足。
-
于调强放疗结束后至治疗后3个月对所有纳入患者进行定期随访,末次随访的结束时间为2020年2月。放射性肺损伤的诊断标准[5]:在影像学检查照射野内出现肺纤维化、肺泡纤维蛋白渗出等肺组织炎性改变,且排除肺结核、恶性肿瘤肺转移等。急性放射性肺损伤的判定标准参考美国肿瘤放射治疗协作组(RTOG)急性放射性肺损伤分级[6]进行诊断:放疗后1~3个月发生的放射性肺损伤,中位发生时间2个月,肺组织无变化为0级;只有轻微咳嗽,或肺部X射线检查无显著异常,用力咳嗽时发生呼吸困难为1级;X射线检查发现肺部有轻微或片状、棉絮状影,持续性的咳嗽,需要药物治疗为2级;咳嗽比较严重,药物治疗无效,安静时会发生呼吸困难为3级;呼吸功能不全,需要给予机械通气或者持续性吸氧为4级;致命性的呼吸困难为5级。本研究将发生2级及以上急性放射性肺损伤作为随访终点。
-
根据急性放射性肺损伤的发生情况将纳入的局部晚期NSCLC患者分为急性放射性肺损伤组和无急性放射性肺损伤组。对患者的临床资料,包括年龄、性别、糖尿病、吸烟史、化疗、体重指数、病理学分期、病理学类型、肿瘤位置、射野数、处方剂量、V5(5 Gy剂量照射的肺体积占全肺总体积的百分比)、V20(20 Gy剂量照射的肺体积占全肺总体积的百分比)、V30(30 Gy剂量照射的肺体积占全肺总体积的百分比)、平均肺剂量、第1秒用力呼气容积(forced expiratory volume in the first second,FEV1)、大体肿瘤体积、放疗剂量分割模式、图像验证、慢阻肺、间质性肺炎、肺弥散功能和心功能不齐的情况进行分析。
-
放疗剂量:常规分割放疗处方剂量54~70 Gy,1.8~2.0 Gy/次,每周5次,共30~35次;大分割放疗处方剂量为45~77 Gy,5~7 Gy/次,每周5次,共9~11次。
图像引导及验证:患者取仰卧位,平静呼吸,明确激光定位点,对患者进行CT(德国YXLON公司Cougar EVO型)扫描,把得到的图像传到放疗计划系统(沈阳东软医疗系统有限公司)中,由2名具有10年以上工作经验的医师勾画靶区,大体肿瘤体积的范围包括肺内原发灶、纵膈转移淋巴结、同侧肺门。常规分割放疗可于放疗前进行锥形束投照计算机重组断层影像设备(CBCT)计划验证,大分割放疗必须进行锥形束投照计算机重组断层影像设备(CBCT)计划验证。
-
应用SPSS 24.0软件对数据进行统计学分析。计数资料的比较采用χ2检验,采用LASSO回归分析筛选非零系数的预测因素,采用Logistic回归分析筛选局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的独立危险因素,应用R(R3.5.3)软件包(新西兰奥克兰大学的Ross Ihaka等开发)及rms程序包(美国Richard Matthew Stallman开发)建立局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的风险列线图模型,应用caret程序包(美国苹果公司MacOS)及Bootstrap 自抽样法重复抽样1 000次进行内部验证,计算一致性指数(C-index),并绘制校正曲线、ROC曲线和决策曲线。P<0.05为差异有统计学意义。
-
216例局部晚期NSCLC患者行调强放疗后有65例发生急性放射性肺损伤,其中急性放射性肺损伤2级34例、3级17例、4级11例、5级3例,急性放射性肺损伤的发生率为30.09%。急性放射性肺损伤组和无急性放射性肺损伤组患者的性别、糖尿病、吸烟史、化疗、体重指数、病理学分期、病理学类型、肿瘤位置、射野数、处方剂量、大体肿瘤体积、慢阻肺、间质性肺炎、肺弥散功能和心功能不齐的组间差异均无统计学意义(均P>0.05);而年龄、V5、V20、V30、平均肺剂量、FEV1、放疗剂量分割模式和图像验证的组间差异均有统计学意义(均P<0.05,表1)。
项目 急性放射性
肺损伤组(n=65)无急性放射性
肺损伤组(n=151)χ2值 P值 项目 急性放射性肺
损伤组(n=65)无急性放射性
肺损伤组(n=151)χ2值 P值 年龄 8.737 0.003 V20 9.510 0.002 ≥70岁 22(33.85) 24(15.89) ≥28% 15(23.08) 12(7.95) <70岁 43(66.15) 127(84.11) <28% 50(76.92) 139(92.05) 性别 0.263 0.608 V30 10.014 0.002 男 30(46.15) 64(42.38) ≥18% 18(27.69) 16(10.60) 女 35(53.85) 87(57.62) <18% 47(72.31) 135(89.40) 糖尿病 0.782 0.376 平均肺剂量 9.248 0.002 有 10(15.38) 31(20.53) ≥13 Gy 20(30.77) 20(13.25) 无 55(84.62) 120(79.47) <13 Gy 45(69.23) 131(86.75) 吸烟史 0.048 0.826 FEV1 8.737 0.003 有 12(18.46) 26(17.22) <70% 22(33.85) 24(15.89) 无 53(81.54) 125(82.78) ≥70% 43(66.15) 127(84.11) 化疗 0.095 0.758 大体肿瘤体积 0.481 0.488 是 15(23.08) 32(21.19) ≥160 cm3 18(27.69) 49(32.45) 否 50(76.92) 119(78.81) <160 cm3 47(72.31) 102(67.55) 体重指数 0.035 0.851 放疗剂量分割模式 9.135 0.003 ≥24 kg/m2 8(12.31) 20(13.25) 大分割 24(36.92) 27(17.88) <24 kg/m2 57(87.69) 131(86.75) 常规分割 41(63.08) 124(82.12) 病理学分期 0.056 0.812 图像验证 8.945 0.003 ⅢA 33(50.77) 74(49.01) 是 49(75.38) 137(90.73) ⅢB 32(49.23) 77(50.99) 否 16(24.62) 14(9.27) 病理学类型 0.509 0.476 慢阻肺 0.039 0.843 腺癌 34(52.31) 71(47.02) 有 13(20.00) 32(21.19) 鳞癌 31(47.69) 80(52.98) 无 52(80.00) 119(78.81) 肿瘤位置 0.254 0.615 间质性肺炎 0.110 0.740 周围型 36(55.38) 78(51.66) 有 10(15.38) 26(17.22) 中央型 29(44.62) 73(48.34) 无 55(84.62) 125(82.78) 射野数 0.381 0.537 肺弥散功能 0.832 0.362 ≥6 20(30.77) 53(35.10) <25 mm Hg/min 17(26.15) 31(20.53) <6 45(69.23) 98(64.90) ≥25 mm Hg/min 48(73.85) 120(79.47) 处方剂量 0.505 0.477 心功能不齐 0.716 0.398 ≥60 Gy 27(41.54) 55(36.42) 有 11(16.92) 19(12.58) <60 Gy 38(58.46) 96(63.58) 无 54(83.08) 132(87.42) V5 8.497 0.004 ≥60% 17(26.15) 16(10.60) <60% 48(73.85) 135(89.40) 注:V5、V20、V30分别为 5、20、30 Gy剂量照射的肺体积占全肺总体积的百分比;FEV1为第1秒用力呼气容积 表 1 急性放射性肺损伤组和无急性放射性肺损伤组局部晚期非小细胞肺癌患者一般资料的比较[例(%)]
Table 1. Comparison of the general data of patients with locally advanced non-small cell lung cancer in the acute radiation-induced lung injury group and the non-acute radiation-induced lung injury group (cases (%))
-
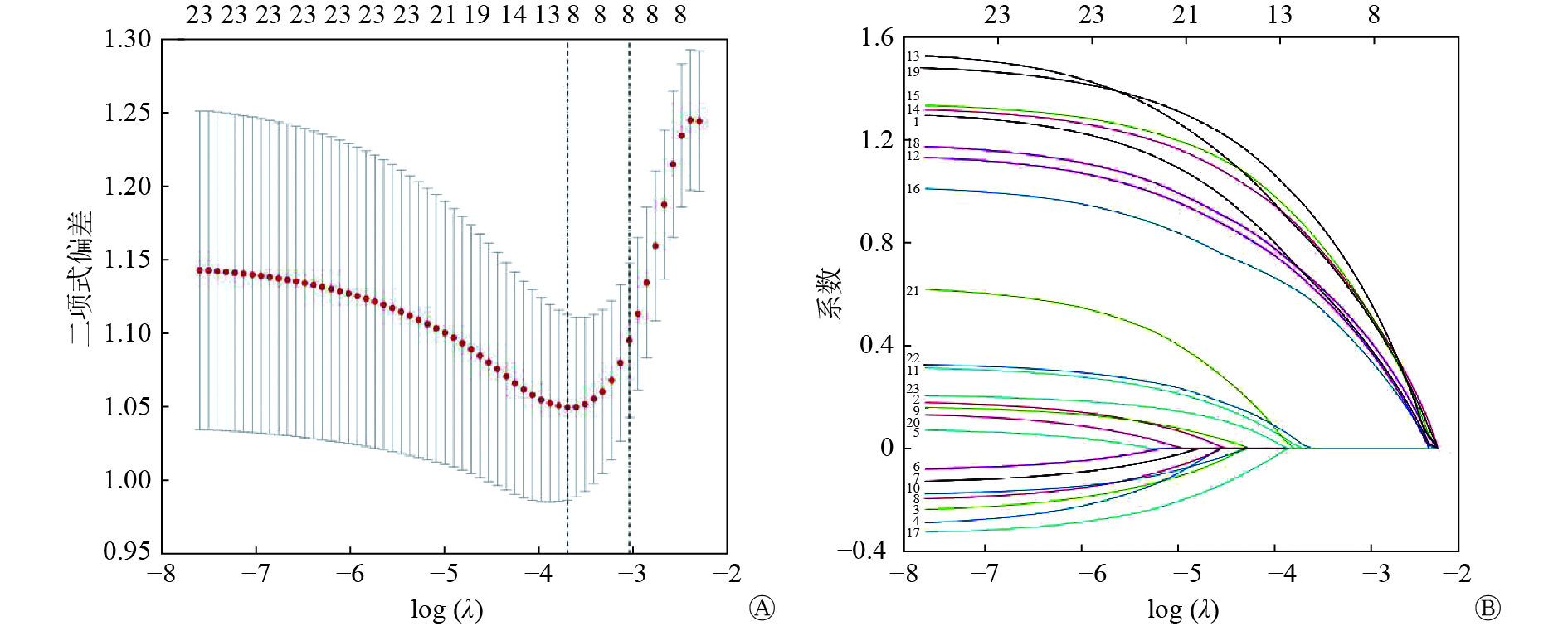
对216例局部晚期NSCLC患者的临床资料进行LASSO回归分析,结果显示,年龄、V5、V20、V30、平均肺剂量、FEV1、放疗剂量分割模式和图像验证是非零系数的预测因素(图1)。

图 1 LASSO回归分析筛选局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的预测因素图
Figure 1. LASSO regression analysis to screen the predictors of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiation therapy
-
以LASSO回归分析筛选的预测因素(年龄、V5、V20、V30、平均肺剂量、FEV1、放疗剂量分割模式和图像验证)为自变量,以是否发生急性放射性肺损伤为因变量,进行多因素Logistic回归分析。结果显示,年龄、V5、V20、V30、平均肺剂量、FEV1、放疗剂量分割模式和图像验证是局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的独立危险因素(均P<0.05,表2)。
因素 回归系数 标准误 Wald值 P值 OR值 95%CI 年龄 1.225 0.431 8.086 0.004 3.404 1.463~7.918 V5 1.144 0.465 6.052 0.014 3.138 1.262~7.805 V20 1.431 0.513 7.791 0.005 4.183 1.531~11.428 V30 1.434 0.461 9.667 0.002 4.197 1.699~10.365 平均肺剂量 1.479 0.438 11.418 0.001 4.388 1.861~10.346 第1秒用力呼气容积 1.081 0.423 6.533 0.011 2.946 1.287~6.748 放疗剂量分割模式 1.158 0.402 8.306 0.004 3.185 1.449~7.002 图像验证 1.545 0.475 10.596 0.001 4.688 1.849~11.886 注:V5、V20、V30分别为5、20、30 Gy剂量照射的肺体积占全肺总体积的百分比;CI为置信区间 表 2 局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiation therapy
-
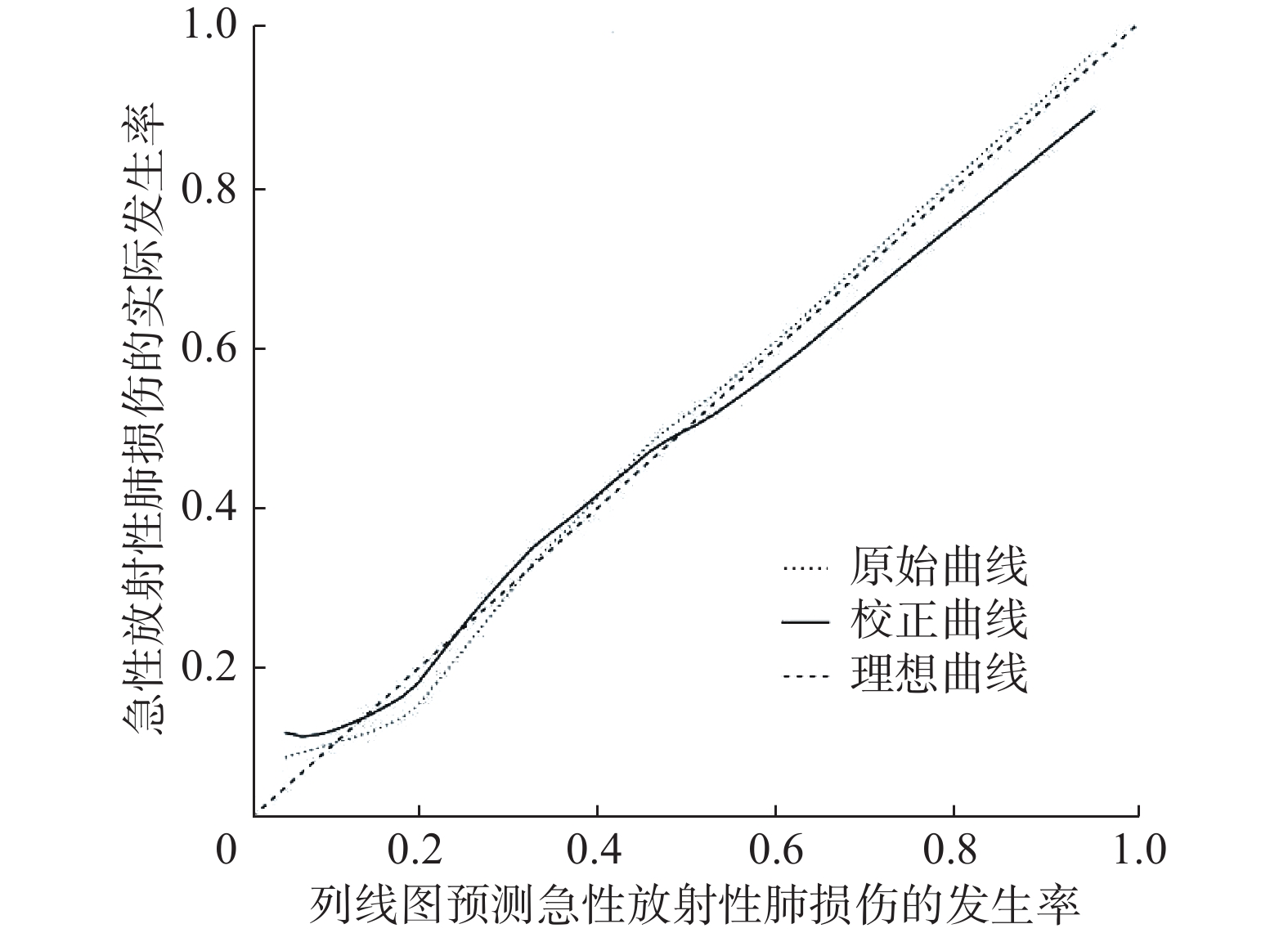
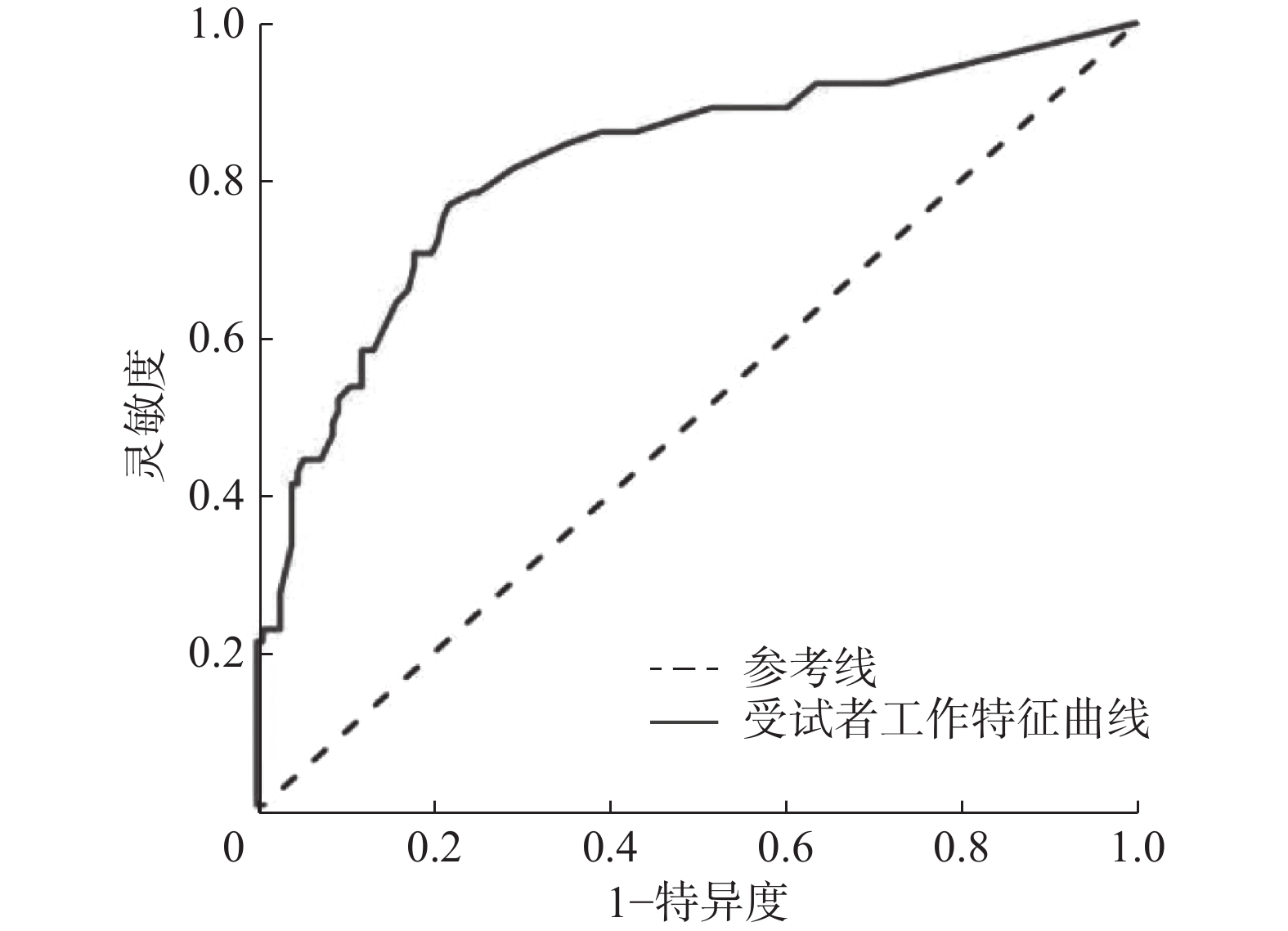
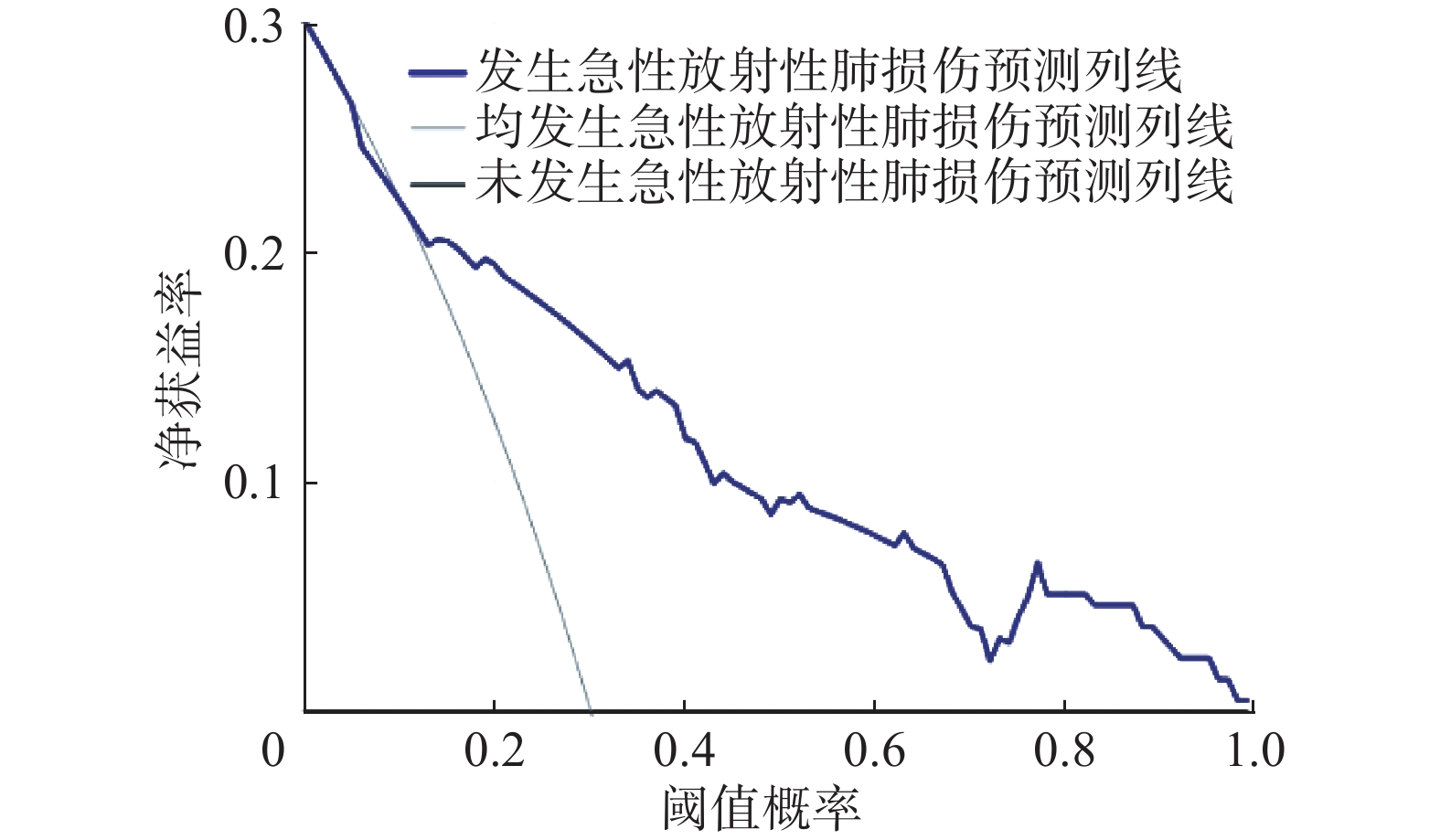
发生急性放射性肺损伤的风险列线图模型见图2,当年龄≥70岁为79分、V5≥60%为74分、V20≥28%为92.5分、V30≥18%为92.5分、平均肺剂量≥13 Gy为96分、FEV1<70%为70分、大分割放疗为75分、未进行图像验证为100分。总分为50~330分时,对应局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的概率为10%~90%,其中风险列线图模型的一致性指数为0.819(95%CI:0.789~0.853)。由图3可见,校正曲线与理想曲线接近。由图4可见,ROC曲线的AUC为0.802。由图5可见,决策曲线显示阈值概率在6%~100%时,具有较高的净获益值。以上结果均说明本模型具有良好的预测准确性。

图 2 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型
Figure 2. A nomogram model for predicting the risk of acute radiation-induced lung injury after intensity-modulated radiation therapy in patients with locally advanced non-small cell lung cancer

图 3 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型的校正曲线
Figure 3. Calibration curve of a nomogram model for predicting the risk of acute radiation-induced lung injury after intensity-modulated radiotherapy in patients with locally advanced non-small cell lung cancer

图 4 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型的受试者工作特征曲线
Figure 4. Receiver operating characteristic curve of the nomogram model for predicting the risk of acute radiation-induced lung injury after intensity-modulated radiation therapy in patients with locally advanced non-small cell lung cancer

图 5 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型的决策曲线
Figure 5. Decision curve of the nomogram model for predicting the risk of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiation therapy
-
NSCLC患者调强放疗后发生急性放射性肺损伤会严重影响患者的治疗效果,给患者造成巨大痛苦[7],而局部晚期NSCLC患者一旦发生放射性肺损伤,将会严重威胁患者的生命健康。本研究纳入的216例局部晚期NSCLC患者调强放疗后有65例患者发生急性放射性肺损伤,发生率为30.09%,稍高于朱成斌等[8]报道的19.43%,其研究对象主要是少数民族患者,而本研究以汉族患者为主要研究对象,因此我们认为,可能是由于民族差异导致的急性放射性肺损伤发生率不同,但这足以表明局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤是值得临床医师重视的问题。
本研究的结果显示,年龄≥70岁、V5≥60%、V20≥28%、V30≥18%、平均肺剂量≥13 Gy、FEV1<70%、大分割放疗和未进行图像验证是局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的独立危险因素。高龄患者更容易发生急性放射性肺损伤,我们认为可能是由于老年患者对放疗的耐受力随年龄的递增而降低所致,这一结果与刘青峰等[9]的研究结果相符。低剂量区间V5也是造成急性放射性肺损伤的原因,本研究结果表明,V5≥60%的患者发生急性放射性肺损伤的概率相对较高,Tang 等[10]也发现,V5是发生急性放射性肺损伤的危险因素。急性放射性肺损伤的严重程度与超过肺耐受剂量的受照体积的大小有关,一旦超过了肺的耐受剂量,发生急性放射性肺损伤的可能性更大,急性放射性肺损伤也更严重。目前,多数研究结果表明,高剂量区间V20和V30是临床预测作用较好的评价放疗计划的剂量参数。王佩等[11]发现,V20、V30是造成急性放射性肺损伤的重要影响因素。Zhou 等[12]认为,V20是一个可以评估急性放射性肺损伤发生风险的剂量学参数。本研究通过分析剂量学参数,得出V20、V30是急性放射性肺损伤的独立危险因素。平均肺剂量是目前公认的具有预测前景的急性放射性肺损伤剂量学参数,国内外相关研究已证实平均肺剂量是急性放射性肺损伤的危险因素[13-14]。将平均肺剂量控制在合适的范围内尤为重要,我们在实践中发现平均肺剂量一旦达到13 Gy,急性放射性肺损伤的发生率明显上升,这可能是由于此时的平均肺剂量已经接近或者达到了肺能够耐受的剂量,因此导致肺损伤发生的风险上升。基础肺功能是发生急性放射性肺损伤的影响因素,肺功能较差的患者对放疗的耐受力较差,放疗后恢复较慢,最终增加急性放射性肺损伤发生的风险。大分割放疗可以快速抑制肿瘤细胞的生长繁殖,降低肿瘤细胞的转移率,但是会使正常组织的损伤增加,延长放疗后的恢复时间,从而增加急性放射性肺损伤的发生风险。放疗时进行图像验证能够做到精准治疗,而未进行图像验证的患者在治疗时可能会存在移位误差,导致急性放射性肺损伤的发生风险增加。
本研究基于筛选出的危险因素建立了局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的列线图模型,医师可以通过患者的各项得分对局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的概率进行个体化预测,及早识别高风险患者并对其进行重点监控。同时,医师可以针对能够控制的危险因素给予患者一定的干预措施,如在保证治疗效果的前提下,适当调整剂量参数,以最大限度地减少放射性肺损伤的发生。本研究中,校正曲线的预测值与实测值基本一致,一致性指数为0.819(95%CI:0.789~0.853),列线图模型的ROC曲线的AUC为0.802,可见本研究的列线图的预测精准度良好。另外,我们发现决策曲线的阈值概率在6%~100%时,采用该列线图来预测局部晚期NSCLC患者调强放疗后急性放射性肺损伤的发生风险具有较高的净获益值,可知该列线图具有较为良好的临床预测价值。
综上所述,年龄≥70岁、V5≥60%、V20≥28%、V30≥18%、平均肺剂量≥13 Gy、FEV1<70%、大分割放疗和未进行图像验证是局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的独立危险因素,本研究构建的列线图模型对局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的预测具有较高的准确性,临床价值较高。另外,本研究为单中心回顾性研究,样本量有限且只进行了内部验证,结果可能存在偏倚,还需要更多的多中心研究加以验证。
利益冲突 所有作者声明无利益冲突
作者贡献声明 郑玮负责试验的设计、资料的收集、论文的撰写;洪梅负责试验的设计;常远负责数据的整理与分析
局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的影响因素及风险预测模型研究
Influencing factors and risk prediction model of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiotherapy
-
摘要:
目的 探讨局部晚期非小细胞肺癌(NSCLC)患者调强放疗后发生急性放射性肺损伤的危险因素,并建立预测风险的列线图模型。 方法 回顾性分析2017年5月至2019年11月于南京医科大学附属脑科医院行调强放疗的216例局部晚期NSCLC患者的临床资料,其中男性94例、女性122例,年龄37~83(61.5±9.6)岁。根据急性放射性肺损伤的发生情况将患者分为急性放射性肺损伤组和无急性放射性肺损伤组。计数资料的比较采用χ2检验,采用LASSO分析和Logistic回归分析筛选局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的独立危险因素,采用R软件包建立预测局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的风险列线图模型,计算一致性指数,绘制校正曲线、受试者工作特征(ROC)曲线和决策曲线。 结果 216例局部晚期NSCLC患者调强放疗后有65例患者发生急性放射性肺损伤,发生率为30.09%。LASSO分析和Logistic回归分析结果显示,年龄、V5、V20、V30、平均肺剂量、第1秒用力呼气容积(FEV1)、放疗剂量分割模式及图像验证是局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的独立危险因素(OR=2.946~4.688,均P<0.05)。建立预测局部晚期NSCLC患者调强放疗后发生急性放射性肺损伤的风险列线图模型的一致性指数为0.819(95%CI:0.789~0.853),校正曲线与理想曲线相接近,ROC曲线下面积为0.802,决策曲线显示阈值概率在6%~100%时,具有较高的净获益值。 结论 基于年龄、V5、V20、V30、平均肺剂量、FEV1、放疗剂量分割模式及图像验证建立的列线图对局部晚期NSCLC患者调强放疗后急性放射性肺损伤发生风险的预测具有较高的准确率。 Abstract:Objective To investigate the risk factors of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer (NSCLC) after intensity-modulated radio therapy (IMRT) and establish a nomogram model to predict the corresponding risk. Methods The clinical data of 216 patients with locally advanced NSCLC who were treated with IMRT in the Brain Hospital Affiliated to Nanjing Medical University from May 2017 to November 2019 were retrospectively analyzed, including 94 males and 122 females, with an average age of 37–83(61.5±9.6) years old. Based on the occurrence of acute radiation-induced lung injury, the selected patients with locally advanced NSCLC were divided into the acute radiation-induced lung injury group and the non-acute radiation-induced lung injury group. Herein, count data were compared using the χ2 test, LASSO analysis, and Logistic regression analysis used to screen independent risk factors of acute radiation-induced lung injury in patients with locally advanced NSCLC after IMRT. In addition, the R software was used to predict the occurrence of acute radiation in patients with locally advanced NSCLC after IMRT. Risk nomogram model of lung injury, plotting calibration curve, receiver operating characteristic (ROC) curve, and decision curve. Results Among 216 patients with locally advanced NSCLC, acute radiation-induced lung injury occurred in 65 patients after IMRT, with an incidence rate of 30.09%. Logistic regression analysis showed that age, V5, V20, V30, mean lung dose, forced expiratory volume in the first second (FEV1), hypofractionated radiotherapy, and image verification are independent risk factors for acute radiation-induced lung injury in patients with locally advanced NSCLC after IMRT (OR=2.946–4.688, all P<0.05). The consistency index of the nomogram model for predicting the risk of acute radiation-induced lung injury in patients with locally advanced NSCLC after IMRT was 0.819(95%CI: 0.789–0.853), the calibration curve was close to the ideal curve, and the area under the ROC curve was 0.802, the decision curve shows that when the threshold probability is between 6% and 100%, hence, there is a higher net benefit value. Conclusions The nomogram established based on age, V5, V20, V30, mean lung dose, FEV1, hypofractionated radiotherapy, and image verification has high accuracy in predicting the risk of acute radiation-induced lung injury in patients with locally advanced NSCLC after IMRT. -
图 1 LASSO回归分析筛选局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的预测因素图
Figure 1. LASSO regression analysis to screen the predictors of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiation therapy
图 2 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型
Figure 2. A nomogram model for predicting the risk of acute radiation-induced lung injury after intensity-modulated radiation therapy in patients with locally advanced non-small cell lung cancer
图 3 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型的校正曲线
Figure 3. Calibration curve of a nomogram model for predicting the risk of acute radiation-induced lung injury after intensity-modulated radiotherapy in patients with locally advanced non-small cell lung cancer
图 4 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型的受试者工作特征曲线
Figure 4. Receiver operating characteristic curve of the nomogram model for predicting the risk of acute radiation-induced lung injury after intensity-modulated radiation therapy in patients with locally advanced non-small cell lung cancer
图 5 预测局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的风险列线图模型的决策曲线
Figure 5. Decision curve of the nomogram model for predicting the risk of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiation therapy
表 1 急性放射性肺损伤组和无急性放射性肺损伤组局部晚期非小细胞肺癌患者一般资料的比较[例(%)]
Table 1. Comparison of the general data of patients with locally advanced non-small cell lung cancer in the acute radiation-induced lung injury group and the non-acute radiation-induced lung injury group (cases (%))
项目 急性放射性
肺损伤组(n=65)无急性放射性
肺损伤组(n=151)χ2值 P值 项目 急性放射性肺
损伤组(n=65)无急性放射性
肺损伤组(n=151)χ2值 P值 年龄 8.737 0.003 V20 9.510 0.002 ≥70岁 22(33.85) 24(15.89) ≥28% 15(23.08) 12(7.95) <70岁 43(66.15) 127(84.11) <28% 50(76.92) 139(92.05) 性别 0.263 0.608 V30 10.014 0.002 男 30(46.15) 64(42.38) ≥18% 18(27.69) 16(10.60) 女 35(53.85) 87(57.62) <18% 47(72.31) 135(89.40) 糖尿病 0.782 0.376 平均肺剂量 9.248 0.002 有 10(15.38) 31(20.53) ≥13 Gy 20(30.77) 20(13.25) 无 55(84.62) 120(79.47) <13 Gy 45(69.23) 131(86.75) 吸烟史 0.048 0.826 FEV1 8.737 0.003 有 12(18.46) 26(17.22) <70% 22(33.85) 24(15.89) 无 53(81.54) 125(82.78) ≥70% 43(66.15) 127(84.11) 化疗 0.095 0.758 大体肿瘤体积 0.481 0.488 是 15(23.08) 32(21.19) ≥160 cm3 18(27.69) 49(32.45) 否 50(76.92) 119(78.81) <160 cm3 47(72.31) 102(67.55) 体重指数 0.035 0.851 放疗剂量分割模式 9.135 0.003 ≥24 kg/m2 8(12.31) 20(13.25) 大分割 24(36.92) 27(17.88) <24 kg/m2 57(87.69) 131(86.75) 常规分割 41(63.08) 124(82.12) 病理学分期 0.056 0.812 图像验证 8.945 0.003 ⅢA 33(50.77) 74(49.01) 是 49(75.38) 137(90.73) ⅢB 32(49.23) 77(50.99) 否 16(24.62) 14(9.27) 病理学类型 0.509 0.476 慢阻肺 0.039 0.843 腺癌 34(52.31) 71(47.02) 有 13(20.00) 32(21.19) 鳞癌 31(47.69) 80(52.98) 无 52(80.00) 119(78.81) 肿瘤位置 0.254 0.615 间质性肺炎 0.110 0.740 周围型 36(55.38) 78(51.66) 有 10(15.38) 26(17.22) 中央型 29(44.62) 73(48.34) 无 55(84.62) 125(82.78) 射野数 0.381 0.537 肺弥散功能 0.832 0.362 ≥6 20(30.77) 53(35.10) <25 mm Hg/min 17(26.15) 31(20.53) <6 45(69.23) 98(64.90) ≥25 mm Hg/min 48(73.85) 120(79.47) 处方剂量 0.505 0.477 心功能不齐 0.716 0.398 ≥60 Gy 27(41.54) 55(36.42) 有 11(16.92) 19(12.58) <60 Gy 38(58.46) 96(63.58) 无 54(83.08) 132(87.42) V5 8.497 0.004 ≥60% 17(26.15) 16(10.60) <60% 48(73.85) 135(89.40) 注:V5、V20、V30分别为 5、20、30 Gy剂量照射的肺体积占全肺总体积的百分比;FEV1为第1秒用力呼气容积  下载: 导出CSV
下载: 导出CSV
表 2 局部晚期非小细胞肺癌患者调强放疗后发生急性放射性肺损伤的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of acute radiation-induced lung injury in patients with locally advanced non-small cell lung cancer after intensity-modulated radiation therapy
因素 回归系数 标准误 Wald值 P值 OR值 95%CI 年龄 1.225 0.431 8.086 0.004 3.404 1.463~7.918 V5 1.144 0.465 6.052 0.014 3.138 1.262~7.805 V20 1.431 0.513 7.791 0.005 4.183 1.531~11.428 V30 1.434 0.461 9.667 0.002 4.197 1.699~10.365 平均肺剂量 1.479 0.438 11.418 0.001 4.388 1.861~10.346 第1秒用力呼气容积 1.081 0.423 6.533 0.011 2.946 1.287~6.748 放疗剂量分割模式 1.158 0.402 8.306 0.004 3.185 1.449~7.002 图像验证 1.545 0.475 10.596 0.001 4.688 1.849~11.886 注:V5、V20、V30分别为5、20、30 Gy剂量照射的肺体积占全肺总体积的百分比;CI为置信区间
下载: 导出CSV
-
[1] 尤静, 杨丹, 李东明, 等. 同步推量调强放疗在局部晚期非小细胞肺癌中的应用[J]. 中国肺癌杂志, 2019, 22(11): 696−701. DOI: 10.3779/j.issn.1009-3419.2019.11.03.
You J, Yang D, Li DM, et al. Application of simultaneous integrated boost intensity modulated radiotherapy in locally advanced non-small cell lung cancer[J]. Chin J Lung Cancer, 2019, 22(11): 696−701. DOI: 10.3779/j.issn.1009-3419.2019.11.03.[2] 郑连喜, 邓超, 何平, 等. 重组人血管内皮抑制素注射液联合EP化疗[J]. 蚌埠医学院学报, 2020, 45(8): 1013−1016, 1019. DOI: 10.13898/j.cnki.issn.1000-2200.2020.08.006.
Zheng LX, Deng C, He P, et al. Effect of the recombinant human endostatin injection combined with EP chemotherapy and intensity-modulated radiotherapy in patients with advanced non-small cell lung cancer[J]. J Bengbu Med Coll, 2020, 45(8): 1013−1016, 1019. DOI: 10.13898/j.cnki.issn.1000-2200.2020.08.006.[3] 张凌云, 田飞, 龚正, 等. 尼达尼布治疗放射性肺损伤一例并文献复习[J]. 中国呼吸与危重监护杂志, 2021, 20(8): 584−587. DOI: 10.7507/1671-6205.202008044.
Zhang LY, Tian F, Gong Z, et al. Nintedanib in the treatment of a case of radiation-induced lung injury and literature review[J]. Chin J Respir Crit Care Med, 2021, 20(8): 584−587. DOI: 10.7507/1671-6205.202008044.[4] 唐正中, 胡宗涛, 王崇, 等. 局部晚期非小细胞肺癌三维适形放射治疗致放射性肺损伤相关因素探讨[J]. 安徽医药, 2018, 22(6): 1116−1119. DOI: 10.3969/j.issn.1009-6469.2018.06.029.
Tang ZZ, Hu ZT, Wang C, et al. The related factors of radiation-induced lung injury caused by 3DCRT for locally advanced non-small cell lung cancer[J]. Anhui Med Pharm J, 2018, 22(6): 1116−1119. DOI: 10.3969/j.issn.1009-6469.2018.06.029.[5] 中华医学会重症医学分会. 急性肺损伤/急性呼吸窘迫综合征诊断与治疗指南(2006)[J]. 中华内科杂志, 2007, 46(5): 430−435. DOI: 10.3760/j.issn:0578-1426.2007.05.037.
Severe Medicine Branch of Chinese Medical Association. Guidelines for diagnosis and treatment of acute lung injury/acute respiratory distress syndrome (2006)[J]. Chin J Intern Med, 2007, 46(5): 430−435. DOI: 10.3760/j.issn:0578-1426.2007.05.037.[6] Cox JD, Stetz JA, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC)[J]. Int J Radiat Oncol Biol Phys, 1995, 31(5): 1341−1346. DOI: 10.1016/0360-3016(95)00060-C. [7] 陈斌, 石翔翔, 唐涛. 局部晚期周围型非小细胞肺癌调强放疗中大体肿瘤靶区体积变化及肺受量预测研究[J]. 中华肿瘤防治杂志, 2020, 27(14): 1166−1170. DOI: 10.16073/j.cnki.cjcpt.2020.14.10.
Chen B, Shi XX, Tang T. Changes of gross tumor target volume and prediction of lung dose in locally advanced peripheral non-small cell lung cancer treated with intensity-modulated radiotherapy[J]. Chin J Cancer Prev Treat, 2020, 27(14): 1166−1170. DOI: 10.16073/j.cnki.cjcpt.2020.14.10.[8] 朱成斌, 古丽娜尔·吐尔地, 赵辉. 新疆少数民族地区IMRT治疗肺癌诱发的急性放射性肺损伤的危险因素研究[J]. 医学研究杂志, 2019, 48(12): 124−127.
Zhu CB, Tuurdi GL, Zhao H. Risk factors of acute radiation-induced lung injury induced by IMRT in the treatment of lung cancer in ethnic minority areas in Xinjiang[J]. J Med Res, 2019, 48(12): 124−127.[9] 刘青峰, 王葳, 王亿龙. 局部Ⅲ期NSCLC患者调强适形放疗后重度急性放射性肺损伤的危险因素分析[J]. 中国临床研究, 2018, 31(1): 28−31. DOI: 10.13429/j.cnki.cjcr.2018.01.007.
Liu QF, Wang W, Wang YL. Risk factors analysis of severe acute radiation pneumonitis injury following intensity-modulated conformal radiotherapy in local stage Ⅲ non-small cell lung cancer[J]. Chin J Clin Res, 2018, 31(1): 28−31. DOI: 10.13429/j.cnki.cjcr.2018.01.007.[10] Tang X, Li YY, Tian X, et al. Predicting severe acute radiation pneumonitis in patients with non-small cell lung cancer receiving postoperative radiotherapy: development and internal validation of a nomogram based on the clinical and dose–volume histogram parameters[J]. Radiother Oncol, 2019, 132: 197−203. DOI: 10.1016/j.radonc.2018.10.016. [11] 王佩, 岳成山, 王会霞, 等. 食管癌调强放射治疗的初期疗效及急性放射性肺损伤的影响因素分析[J]. 现代生物医学进展, 2020, 20(22): 4373−4377. DOI: 10.13241/j.cnki.pmb.2020.22.039.
Wang P, Yue CS, Wang HX, et al. Analysis of the initial efficacy of intensity modulated radiotherapy for esophageal cancer and the influencing factors of acute radiation-induced lung injury[J]. Prog Mod Biomed, 2020, 20(22): 4373−4377. DOI: 10.13241/j.cnki.pmb.2020.22.039.[12] Zhou ZR, Han Q, Liang SX, et al. Dosimetric factors and Lyman normal-tissue complication modelling analysis for predicting radiation-induced lung injury in postoperative breast cancer radiotherapy: a prospective study[J/OL]. Oncotarget, 2017, 8(20): 33855−33863[2021-12-19]. https://www.oncotarget.com/article/12979/text/. DOI: 10.18632/oncotarget.12979. [13] 许群英, 蒙以良, 黄升武. Ⅲ/Ⅳ期非手术非小细胞肺癌患者行高剂量大分割放疗临床疗效与剂量学参数及放射性肺损伤的关系分析[J]. 癌症进展, 2019, 17(21): 2520−2523.
Xu QY, Meng YL, Huang SW. Analysis of the relationship among clinical efficacy, dosimetric parameters and radiation-induced lung injury in patients with stage Ⅲ/Ⅳ non-small cell lung cancer treated with hypofractionated radiotherapy without surgical management[J]. Oncol Prog, 2019, 17(21): 2520−2523.[14] Pan WY, Bian C, Zou GL, et al. Combing NLR, V20 and mean lung dose to predict radiation induced lung injury in patients with lung cancer treated with intensity modulated radiation therapy and chemotherapy[J/OL]. Oncotarget, 2017, 8(46): 81387−81393[2021-12-19]. https://www.oncotarget.com/article/19032/text/. DOI: 10.18632/oncotarget.19032. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2758
- HTML全文浏览量: 1815
- PDF下载量: 14