


-
据报道,乳腺癌在全球女性恶性肿瘤中的发病率位居第一[1]。放疗可提高乳腺癌患者的术后生存率,降低其局部复发率[2-4]。由于乳腺癌患者预后生存期相对较长,因此减少放疗对心脏和肺等危及器官的不良作用非常重要[5]。目前,越来越多的左侧乳腺癌术后患者采用深吸气屏气(deep inspiration breath-hold,DIBH)放疗,此方法可有效降低心脏等器官的受照剂量[6],但是DIBH技术仅在患者屏气间期直线加速器出束治疗,比传统治疗延长了治疗时间。乳腺癌改良根治术后放疗靶区形状极不规则,容积旋转调强放疗(volumetric modulated arc therapy, VMAT)对复杂靶区更具优势,采用DIBH结合VMAT技术不仅能提高靶区剂量分布,还可显著降低患者正常组织的受照剂量[7-8]。
非均整器(flattening filter free,FFF)模式是一种新型的高剂量率技术,其可明显降低机头散射,缩短放疗照射时间,提高治疗效率[9-10]。直线加速器中加均整器(flattening filter,FF)的作用是为了使靶区内剂量分布均匀,在调强技术未成熟之前,FF对于靶区剂量分布非常重要,随着调强放疗和VMAT的普及,直线加速器均能通过多叶准直器的运动实现靶区内剂量的均匀分布,理论上完全可以移除FF[11]。与FF模式相比较,FFF的射线质变软,剂量率增加,辐射野外散射减少,可降低正常组织的受照剂量,从而降低二次致癌的发生概率[12]。
本研究将多项新技术进行整合,在左侧乳腺癌改良根治术后DIBH放疗中,比较FFF和FF模式下 VMAT计划的剂量学特性以及机器的执行效率,为临床治疗提供一定的参考。
-
完全随机选取2020年12月至2021年5月在西安交通大学第一附属医院行放疗的16例左侧乳腺癌改良根治术后女性患者的临床资料进行回顾性分析,年龄37~61(43.5±5.7)岁。纳入标准:左侧乳腺癌改良根治术后;照射范围包括胸壁、锁骨上下等淋巴结区;一般情况良好,心肺功能基本正常,并且可熟练配合DIBH呼吸模式。本研究经西安交通大学医学院第一附属医院伦理委员会审批通过,批件号:2021伦审科字第(020)号,NO:XJTU1AF2021LSK-020。
-
患者在DIBH呼吸模式下进行CT定位,用乳腺托架固定,所有患者均取仰卧位,双臂外展上举,左臂置于左侧固定位,右臂置于右侧固定位,右手握瑞典Elekta公司的Active Breathing Control呼吸控制开关,使左侧乳腺区域完全暴露,在DIBH状态下,激光灯指示摆位,标记体表摆位标记线,并于相同的屏气状态下,使用荷兰飞利浦公司的Brilliance Big Bore大孔径CT进行扫描,扫描范围上至环状软骨,下至对侧乳腺褶皱下2 cm,扫描层厚0.5 cm, 扫描后将CT图像传输至瑞典Elekta公司的Monaco5.11.03治疗计划系统。
-
参照肿瘤放疗协作组织规范勾画靶区,由1名副主任医师统一勾画临床靶区、计划靶区(plan target volume,PTV)及危及器官,危及器官包括心脏、患侧肺、健侧肺、全肺、健侧乳腺及脊髓等。
-
采用Monaco5.11.03治疗计划系统,对16例患者分别设计FFF和FF 2种VMAT计划,采用瑞典Elekta公司 Versa HD直线加速器6 MV X射线,其中,FFF模式最高剂量率1400 MU/min,FF模式最高剂量率600 MU/min。PTV的处方剂量均为50 Gy/25次。同一患者2种计划均采用相同射野角度及计划优化参数,根据靶区形状设计1个连续弧,起始角度300°±10°,旋转角度200°±10°。采用蒙特卡罗算法,旋转方向设为顺时针,每个扇区设为30°,最大弧数设为2,最大控制点设为120,通量平滑设为中等,最小子野宽度设为0.7 cm, 计算网格设为0.3 cm。优化目标参数设置:心脏V5 Gy<36%、V10 Gy<20%(Vx Gy表示≥x Gy体积占总体积的百分比),平均剂量(Dmean)<6.5 Gy;左肺V5 Gy<52%,V10 Gy<35%,V20 Gy<25%;右肺Dmean<4 Gy,V5 Gy≤10%;右侧乳腺Dmean<5 Gy,脊髓最大剂量(Dmax)≤38 Gy。所有计划均由同1名物理师设计。
-
将FFF-VMAT和FF-VMAT 2种计划均归一为PTV的D95%≥50 Gy(Dx%表示x%靶体积的受照剂量),得到剂量体积直方图(dose volume histogram,DVH) 和等剂量曲线分布,统计靶区PTV的D2%、D50%及D98%,靶区的剂量分布评估:(1)PTV的靶区适形指数(conformity index,CI)=
$ \dfrac{{\mathrm{V}}_{\mathrm{T},\mathrm{r}\mathrm{e}\mathrm{f}}}{{\mathrm{V}}_{\mathrm{T}}} $ ×$ \dfrac{{\mathrm{V}}_{\mathrm{T},\mathrm{r}\mathrm{e}\mathrm{f}}}{{\mathrm{V}}_{\mathrm{r}\mathrm{e}\mathrm{f}}} $ ,其中,$ {\mathrm{V}}_{\mathrm{T},\mathrm{r}\mathrm{e}\mathrm{f}} $ 是处方剂量线包绕PTV的体积,$ {\mathrm{V}}_{\mathrm{T}} $ 是PTV的体积,$ {\mathrm{V}}_{\mathrm{r}\mathrm{e}\mathrm{f}} $ 是处方剂量线所包绕的所有体积,CI值为0~1,其越接近1表示PTV适形度越好[13]。(2)PTV的靶区均匀指数(homogeneity index,HI)=$ \dfrac{{\mathrm{D}}_{2\mathrm{\%}}-{\mathrm{D}}_{98\mathrm{\%}}}{{\mathrm{D}}_{50\mathrm{\%}}} $ ,其中,HI值为0~1,其越接近0表示PTV均匀性越好[13]。(3)PTV的剂量梯度指数(gradient index,GI)$ =\dfrac{{\mathrm{V}}_{50\mathrm{\%}}}{{\mathrm{V}}_{100\mathrm{\%}}} $ ,(VX%表示x%的处方剂量线所包绕的体积),GI越小表示剂量跌落越快[14]。危及器官评价参数包括心脏V5 Gy、V30 Gy、Dmean,左肺(患侧肺)V5 Gy、V10 Gy、V20 Gy、Dmean,右肺(健侧肺)V5 Gy、Dmean,全肺V5 Gy、V10 Gy、V20 Gy、Dmean,右侧乳腺(健侧乳腺)V5 Gy、Dmean,脊髓外放0.5 cm的脊髓危及器官计划体积的Dmean、Dmax,以及5 Gy剂量线所包绕的体积与体表范围内的所有组织体积的百分比。
计划执行效率评估:统计FFF与FF模式下2种VMAT计划的机器总跳数以及Versa HD直线加速器的执行时间。本研究统计的机器执行时间为机器开始出束至整个弧出束结束的连续时间,不包括DIBH间歇的自由呼吸停止出束的时间。
-
应用SPSS 23.0软件对数据进行统计学分析。符合正态分布的计量资料以
$ \bar{{x}}\pm {s} $ 表示,2种计划间比较采用配对t检验(方差齐)。P<0.05为差异有统计学意义。 -
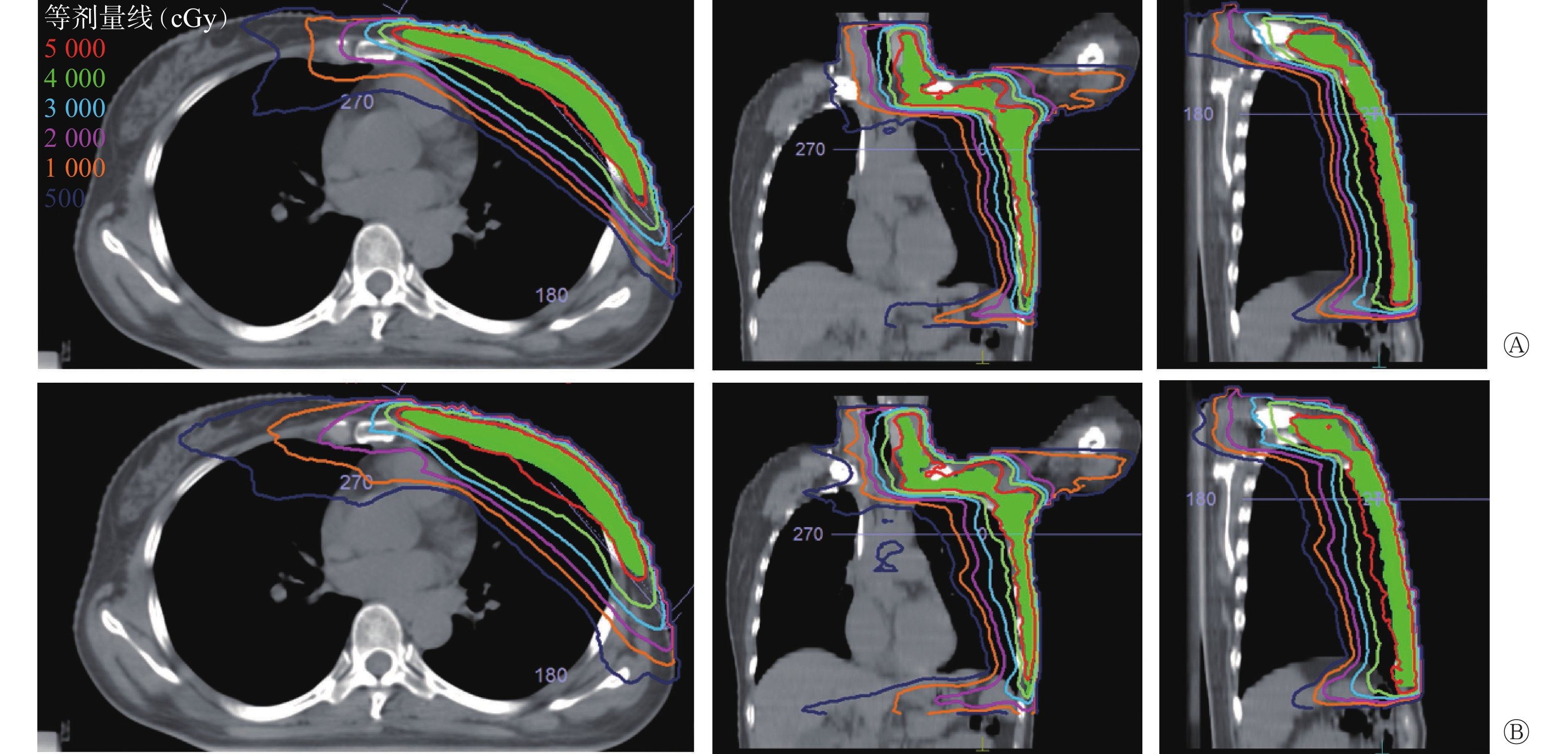
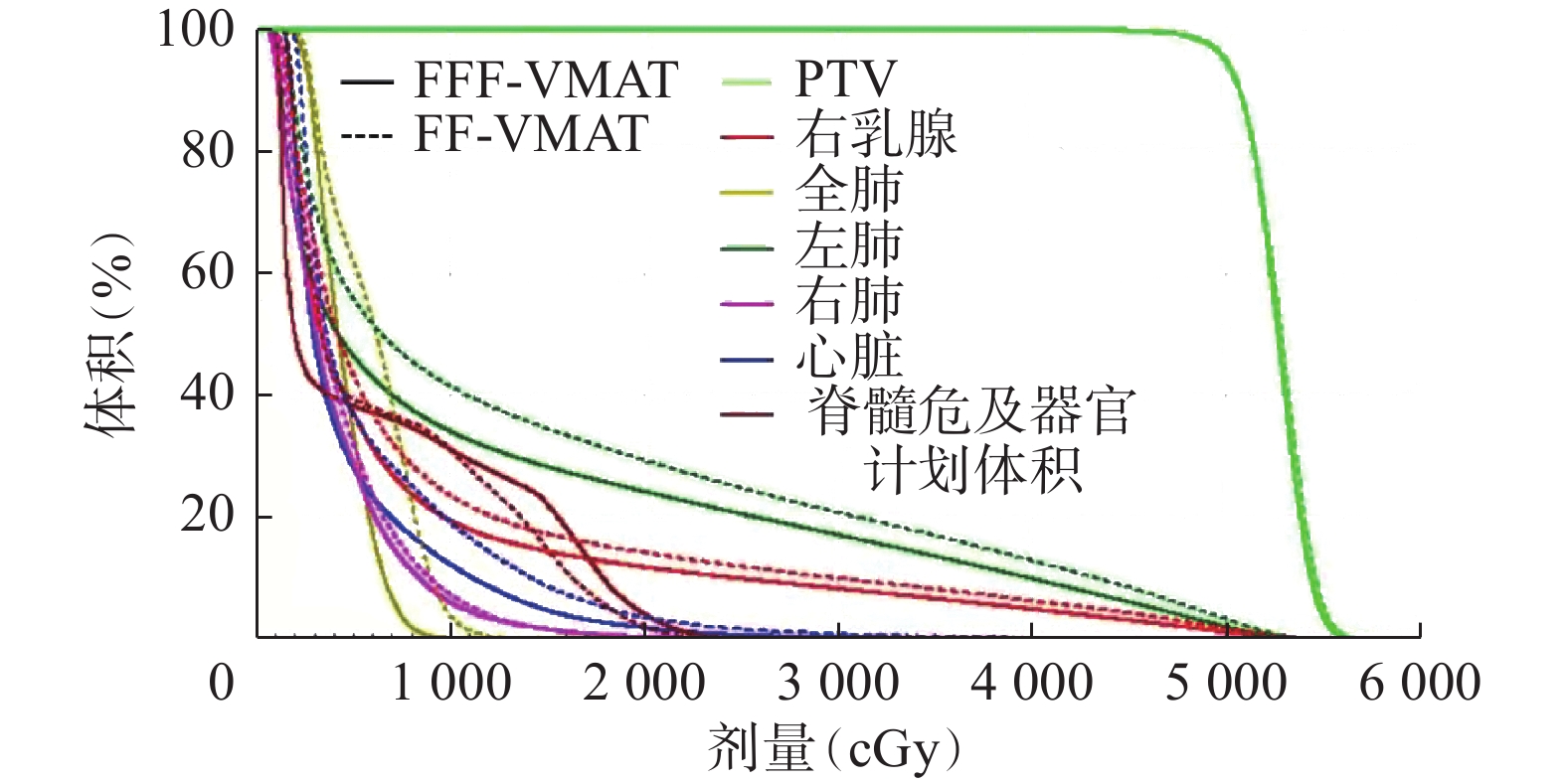
16例乳腺癌改良根治术后患者2种计划均满足95%以上的靶区体积达到处方剂量50 Gy,其中1例患者2种计划的DVH和等剂量曲线分布对比如图1和图2所示,结果显示2种计划的靶区剂量分布相似,但FFF模式下危及器官的受照剂量明显低于FF模式。
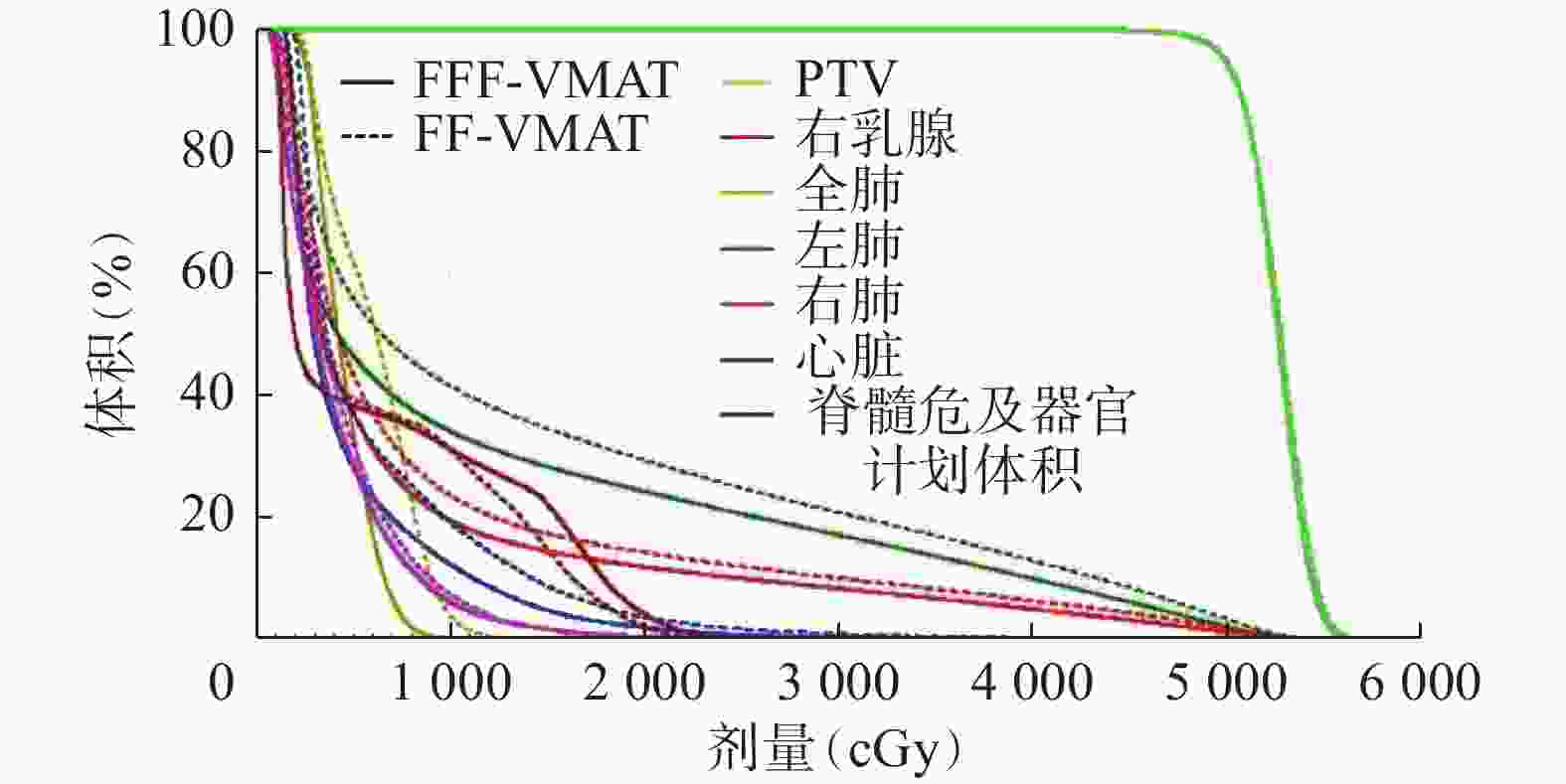
图 1 左侧乳腺癌改良根治术后患者(女性,46岁)2种容积旋转调强技术计划靶区及危及器官的剂量体积直方图
Figure 1. Dose volume histogram comparison of the two volumetric modulated arc therapy plans in a patient (female, 46 years old) with left breast cancer after modified radical mastectomy
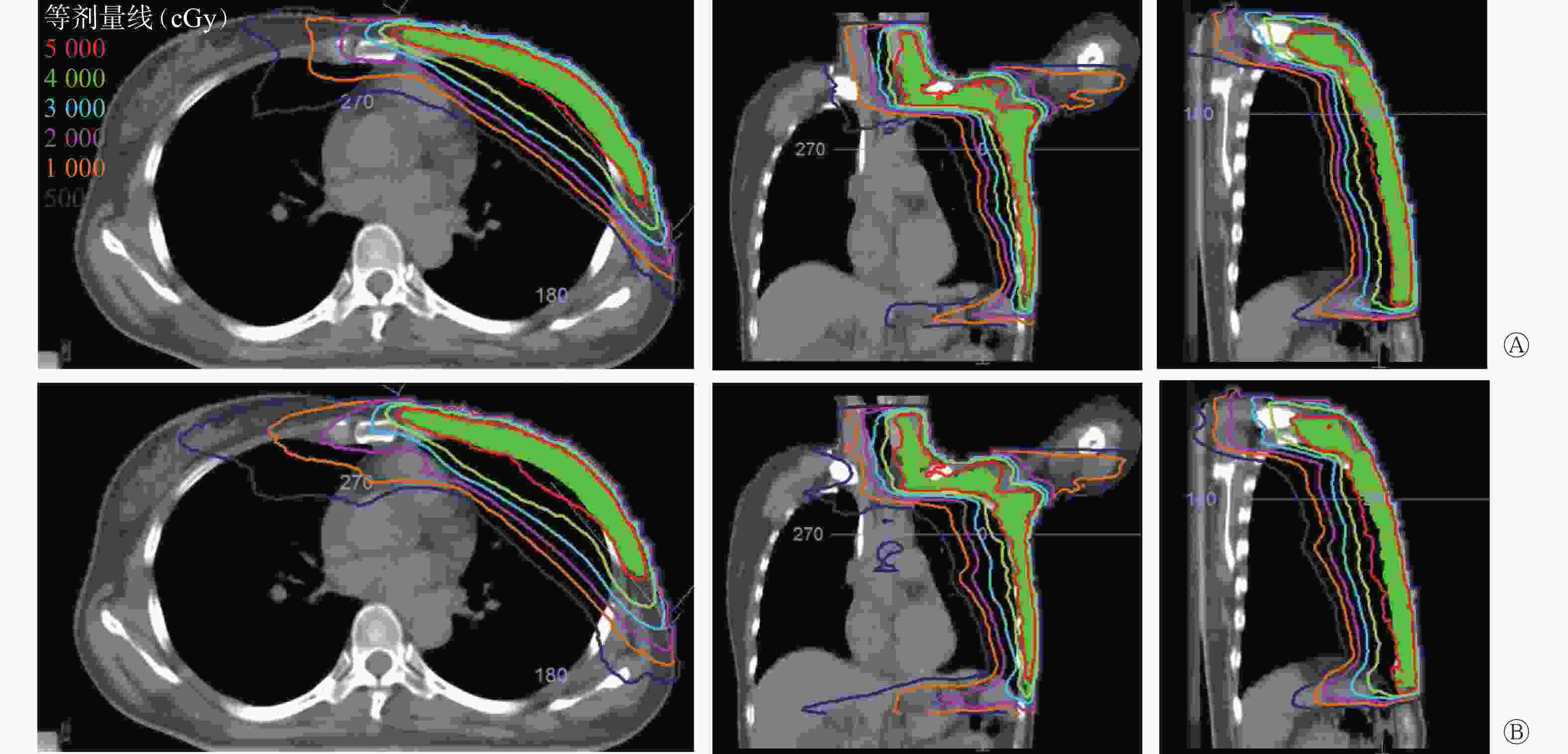
图 2 左侧乳腺癌改良根治术后患者(女性,46岁)2种容积旋转调强放疗计划同一CT图像等剂量线分布比较 A为FFF-VMAT计划;B为FF-VMAT计划。A和B图从左至右依次为横断面、冠状面、矢状面图。FFF为非均整器;VMAT为容积旋转调强放疗;FF为均整器
Figure 2. Comparison of isodose distribution in the same CT images with two volumetric modulated arc therapy plans of a patient (female, 46 years old) with left breast cancer after modified radical mastectomy
-
由表1可知,2种计划的6个靶区剂量学参数D2%、D50%、D98%、CI、 HI、GI均相近,且差异均无统计学意义(均P>0.05);FFF模式机器的总跳数明显高于 FF模式,且为FF模式的1.32倍,差异有统计学意义(P<0.05);但 FFF 模式的执行时间为FF的88.9%,且二者间的差异有统计学意义(P<0.05)。
参数 FFF-VMAT FF-VMAT t值 P值 D2%(cGy) 5640.22±70.09 5613.52±63.07 1.644 0.121 D50%(cGy) 5323.74±48.55 5307.29±51.74 1.462 0.164 D98%(cGy) 4881.38±32.21 4891.64±31.88 −1.386 0.186 适形指数 0.87±0.49 0.87±0.05 −0.490 0.631 均匀指数 0.14±0.02 0.14±0.01 1.415 0.178 梯度指数 3.24±0.66 3.30±0.67 −1.519 0.150 机器跳数(MU) 1073.41±143.79 815.70±87.69 8.665 <0.001 执行时间(s) 128.00±11.64 144.75±11.45 −4.373 0.001 注:FFF为非均整器;VMAT为容积旋转调强放疗;FF为均整器;Dx%表示x%靶体积的受照剂量 表 1 16例左侧乳腺癌改良根治术后女性患者2种VMAT计 划的靶区剂量及机器参数比较(
$ \bar{{x}}\pm {s} $ Table 1. Comparison of target dosimetric and machine parameters between the two volumetric modulated arc therapy plans in 16 female patients with left breast cancer after modified radical mastectomy (
$ \bar{{x}}\pm {s} $ -
2种计划的危及器官受照剂量如表2所示。由表2可知,FFF模式下,心脏受照剂量的V5 Gy、V30 Gy及Dmean,患侧肺V5 Gy、V10 Gy及Dmean,全肺V5 Gy、V10 Gy、V20 Gy及Dmean,患者受照剂量的V5 Gy均低于FF模式,组间比较差异均有统计学意义(均P<0.05);虽然患侧肺V20 Gy,健侧肺Dmean、V5 Gy,健侧乳腺 Dmean,脊髓危及器官计划体积的Dmean、Dmax,均略低于 FF 模式,但其差异均无统计学意义(均P>0.05)。
参数 FFF-VMAT FF-VMAT t值 P值 心脏 V5 Gy(%) 32.19±7.18 34.27±7.29 −2.156 0.048 V30 Gy(%) 1.33±1.07 1.70±1.27 −2.632 0.019 Dmean(cGy) 508.50±84.96 587.43±126.48 −2.689 0.017 左肺(患侧肺) V5 Gy(%) 52.02±3.80 55.82±3.55 −4.741 <0.001 V10 Gy(%) 37.80±5.53 40.65±4.23 −2.494 0.025 V20 Gy(%) 27.45±4.82 29.19±3.94 −2.058 0.057 Dmean(cGy) 1418.31±136.02 1516.83±171.71 −2.467 0.026 右肺(健侧肺) V5 Gy(%) 12.83±2.57 13.59±3.04 −0.986 0.340 Dmean(cGy) 278.43±57.28 294.51±44.58 −0.908 0.378 全肺 V5 Gy(%) 34.88±3.14 36.96±3.92 −2.156 0.048 V10 Gy(%) 21.23±3.44 22.87±3.92 −2.320 0.035 V20 Gy(%) 12.55±1.93 13.71±1.61 −2.600 0.020 Dmean(cGy) 829.55±63.94 919.68±59.36 −3.928 0.001 右乳腺(健侧) V5 Gy(%) 23.41±4.06 23.41±3.99 0.001 0.999 Dmean(cGy) 425.96±88.41 435.89±92.34 −0.830 0.420 脊髓外放0.5 cm Dmax(cGy) 2677.70±471.84 2681.10±506.08 −0.064 0.950 Dmean(cGy) 627.55±159.14 610.19±162.16 1.184 0.255 患者受照剂量 V5 Gy(%) 25.71±3.74 27.48±3.74 −2.465 0.026 注:FFF为非均整器;VMAT为容积旋转调强放疗;FF为均整器;Vx Gy为≥x Gy体积占总体积的百分比;Dmean为平均剂量;Dmax为最大剂量 表 2 16例左侧乳腺癌改良根治术后女性患者2种VMAT计 划的危及器官剂量学比较(
$ \bar{{x}}\pm {s} $ Table 2. Comparison of dosimetry of organs at risk of two volumetric modulated arc therapy plans in 16 female patients with left breast cancer after modified radical mastectomy (
$ \bar{{x}}\pm {s} $ -
乳腺癌术后患者采用DIBH技术,不仅可预防呼吸运动造成的靶区漏照,还可降低心脏及肺等危及器官的受照剂量[15]。然而,由于DIBH仅在患者屏气间期直线加速器出束治疗,会大幅延长治疗时间,导致很多需要DIBH治疗的患者无法耐受[16]。目前国内各大放疗中心均可开展调强放疗和VMAT技术,采用调强放疗,FFF通过多叶准直器运动可满足靶区剂量分布的均匀性[17-18],FFF模式使加速器输出剂量大幅提高,可显著缩短放疗照射时间[10,19]。我们在左侧乳腺癌改良根治术后患者的DIBH VMAT中,分别采用FFF和FF模式进行照射,结果表明2种模式下靶区剂量相似,FFF模式危及器官受照剂量更低,并且可显著缩短治疗时间。
本研究中FFF模式VMAT计划与传统FF模式均能满足临床治疗要求,2种模式靶区覆盖率D2%、D50%及D98%相似,CI、HI及GI比较差异也均无统计学意义(均P>0.05),这与既往相关研究结果一致,FFF模式与FF模式靶区剂量分布无明显差异[20-21]。
在危及器官保护方面,本研究FFF模式的心脏V5 Gy、V30 Gy、Dmean,患侧肺V5 Gy、V10 Gy、Dmean,全肺V5 Gy、V10 Gy、V20 Gy、Dmean,患者受照剂量的V5 Gy均低于FF模式,且差异均有统计学意义(均P<0.05)。在健侧乳腺、健侧肺及脊髓方面, FFF模式略优于FF模式,但差异均无统计学意义(均P>0.05)。有研究结果表明,与传统的FF模式相比,FFF模式去除了均整器,机头内射束特性改变,减少了散射和机头漏射,从而降低了照射野外的剂量[22-23],因此可更好地保护危及器官及正常组织,减少全身低剂量照射,从而降低了二次致癌等并发症发生的概率[24-25]。特别是对于胸壁较易复发的乳腺癌改良根治术后患者,FFF射束中低能部分的X射线更多,有利于提高皮肤浅层剂量,弥补了建成效应造成的剂量不足,更适用于乳腺癌这种接近体表的靶区[26]。总之,与FF模式相比,FFF模式VMAT在危及器官的保护方面更具优势。
从机器效率来看,本研究结果显示,FFF模式的机器跳数是FF模式的1.32倍,但机器出束时间却缩短为FF模式的88.9%,大大缩短了患者的治疗时间,这与Koivumäki等[27]的研究结果一致,虽然FFF模式的机器跳数增加,但出束时间反而减少,因此FFF模式具有更高的机器执行效率。
综上所述,FFF和FF模式VMAT 2种计划均能满足临床治疗需求,2种计划的靶区剂量分布相似,FFF模式在危及器官保护方面优于FF模式,尤其在治疗效率方面,由于DIBH延长了治疗时间,FFF模式的高剂量率可明显缩短DIBH的治疗时间,提高患者的治疗效率和舒适度,使更多的患者可以耐受DIBH治疗,因此FFF模式在左侧乳腺癌改良根治术后患者的DIBH临床治疗中有应用价值,由于本研究仅纳入了16例患者,数据样本偏小,不足以提供足够的依据,后续仍需扩大样本量,进行更深入的研究。
利益冲突 所有作者声明无利益冲突
作者贡献声明 柴林燕负责论文的撰写和放疗计划的设计;王科峰负责数据的统计分析;范秋红负责数据的记录和分析;蒙渡负责靶区的勾画;张晓智负责靶区及放疗计划的审核
非均整器模式在左侧乳腺癌改良根治术后患者深吸气屏气容积旋转调强放疗中的剂量学优势
Dosimetric advantages of flattening filter free technique in deep inspiration breath-hold treatments of left-sided breast cancer after modified radical mastectomy with volumetric modulated arc therapy
-
摘要:
目的 比较非均整器(FFF)模式和均整器(FF)模式在左侧乳腺癌改良根治术后深吸气屏气(DIBH)动态容积旋转调强放疗(VMAT)中的剂量学差异。 方法 回顾性分析2020年12月至2021年5月在西安交通大学第一附属医院行DIBH放疗的16例左侧乳腺癌改良根治术后女性患者的临床资料,年龄37~61(43.5±5.7)岁。对同一患者分别设计FFF和FF模式的VMAT计划,给予计划靶区(PTV)相同的处方剂量50 Gy/25次,在达到相同的剂量归一条件下,比较靶区剂量学、危及器官受量及机器执行效率的差异。组间数据比较采用配对t检验。 结果 2种模式下靶区PTV的D2%、D50%、D98%(Dx%表示x%靶体积的受照剂量)、适形指数、平均指数及梯度指数差异均无统计学意义(t=−1.519~1.644,均P>0.05);FFF模式的心脏V5 Gy、V30 Gy(Vx Gy表示≥x Gy体积占总体积的百分比)及平均剂量(Dmean),患侧肺V5 Gy、V10 Gy及Dmean,全肺V5 Gy、V10 Gy、V20 Gy及Dmean,患者受照剂量的V5 Gy均优于FF模式,组间比较差异均有统计学意义(t=−4.741~−2.156,均P<0.05);FFF模式机器跳数是FF模式的1.32倍[(1073.41±143.79)MU对(815.70±87.69) MU],但执行时间却减少为FF模式的88.9%[(128.00±11.64) s对(144.75±11.45) s],且差异均有统计学意义(t=8.665、−4.373,均P<0.05)。 结论 2种模式下靶区剂量相似,FFF模式危及器官受照剂量更低,并且可显著缩短DIBH治疗时间。 Abstract:Objective To compare the dosimetry difference between flattening filter free (FFF) mode and flattening filter (FF) mode in deep inspiration breath-hold(DIBH) treatments of left-sided breast cancer after modified radical mastectomy with volumetric modulated arc therapy (VMAT). Methods Retrospectively analyzed the clinical data of 16 female patients with left breast cancer after modified radical mastectomy with DIBH radiotherapy in the First Affiliated Hospital of Xi'an Jiaotong University from December 2020 to May 2021, aged 37 to 61 (43.5±5.7) years old. VMAT plans of FFF and FF modes were designed for the same patient, and the same prescription dose of 50 Gy/25 times was set in the planning target volume (PTV). Under the same dose normalization, the dosimetric parameters of the target and the organs at risk(OAR) and treatment efficiency were compared between the two plans. Paired t-test was used to compare the data between groups. Results No significant differences in D2%, D50%, D98%, CI , HI and GI were found in the target area between the two modes (t=−1.519-1.644; all P>0.05). FFF mode was superior to FF mode in protection of OAR, such as V5 Gy, V30 Gy (Vx Gy: ≥x Gy volume as a percentage of total volume) and mean dose (Dmean) of heart; V5 Gy, V10 Gy and Dmean of ipsilateral lung; V5 Gy, V10 Gy, V20 Gy and Dmean of whole lung; and V5 Gy of patient dose, and the differences between the two modes were statistically significant (t=−4.741 to−2.156; all P<0.05). The total monitor units of FFF mode was 1.32 times of that in FF mode ((1073.41±143.79) MU vs.(815.70±87.69) MU), but the total delivery time was reduced to 88.9% of that in FF mode((128.00±11.64) s vs.(144.75±11.45) s), and the differences between the two modes were statistically significant (t=8.665, −4.373; both P<0.05). Conclusion The target dose between the two modes were similar. The FFF mode can remarkably reduce the radiation dose of OAR and normal tissues, and can significantly shorten the time of DIBH therapy. -
图 1 左侧乳腺癌改良根治术后患者(女性,46岁)2种容积旋转调强技术计划靶区及危及器官的剂量体积直方图
Figure 1. Dose volume histogram comparison of the two volumetric modulated arc therapy plans in a patient (female, 46 years old) with left breast cancer after modified radical mastectomy
图 2 左侧乳腺癌改良根治术后患者(女性,46岁)2种容积旋转调强放疗计划同一CT图像等剂量线分布比较 A为FFF-VMAT计划;B为FF-VMAT计划。A和B图从左至右依次为横断面、冠状面、矢状面图。FFF为非均整器;VMAT为容积旋转调强放疗;FF为均整器
Figure 2. Comparison of isodose distribution in the same CT images with two volumetric modulated arc therapy plans of a patient (female, 46 years old) with left breast cancer after modified radical mastectomy
表 1 16例左侧乳腺癌改良根治术后女性患者2种VMAT计 划的靶区剂量及机器参数比较(
$ \bar{{x}}\pm {s} $ Table 1. Comparison of target dosimetric and machine parameters between the two volumetric modulated arc therapy plans in 16 female patients with left breast cancer after modified radical mastectomy (
$ \bar{{x}}\pm {s} $ 参数 FFF-VMAT FF-VMAT t值 P值 D2%(cGy) 5640.22±70.09 5613.52±63.07 1.644 0.121 D50%(cGy) 5323.74±48.55 5307.29±51.74 1.462 0.164 D98%(cGy) 4881.38±32.21 4891.64±31.88 −1.386 0.186 适形指数 0.87±0.49 0.87±0.05 −0.490 0.631 均匀指数 0.14±0.02 0.14±0.01 1.415 0.178 梯度指数 3.24±0.66 3.30±0.67 −1.519 0.150 机器跳数(MU) 1073.41±143.79 815.70±87.69 8.665 <0.001 执行时间(s) 128.00±11.64 144.75±11.45 −4.373 0.001 注:FFF为非均整器;VMAT为容积旋转调强放疗;FF为均整器;Dx%表示x%靶体积的受照剂量  下载: 导出CSV
下载: 导出CSV
表 2 16例左侧乳腺癌改良根治术后女性患者2种VMAT计 划的危及器官剂量学比较(
$ \bar{{x}}\pm {s} $ Table 2. Comparison of dosimetry of organs at risk of two volumetric modulated arc therapy plans in 16 female patients with left breast cancer after modified radical mastectomy (
$ \bar{{x}}\pm {s} $ 参数 FFF-VMAT FF-VMAT t值 P值 心脏 V5 Gy(%) 32.19±7.18 34.27±7.29 −2.156 0.048 V30 Gy(%) 1.33±1.07 1.70±1.27 −2.632 0.019 Dmean(cGy) 508.50±84.96 587.43±126.48 −2.689 0.017 左肺(患侧肺) V5 Gy(%) 52.02±3.80 55.82±3.55 −4.741 <0.001 V10 Gy(%) 37.80±5.53 40.65±4.23 −2.494 0.025 V20 Gy(%) 27.45±4.82 29.19±3.94 −2.058 0.057 Dmean(cGy) 1418.31±136.02 1516.83±171.71 −2.467 0.026 右肺(健侧肺) V5 Gy(%) 12.83±2.57 13.59±3.04 −0.986 0.340 Dmean(cGy) 278.43±57.28 294.51±44.58 −0.908 0.378 全肺 V5 Gy(%) 34.88±3.14 36.96±3.92 −2.156 0.048 V10 Gy(%) 21.23±3.44 22.87±3.92 −2.320 0.035 V20 Gy(%) 12.55±1.93 13.71±1.61 −2.600 0.020 Dmean(cGy) 829.55±63.94 919.68±59.36 −3.928 0.001 右乳腺(健侧) V5 Gy(%) 23.41±4.06 23.41±3.99 0.001 0.999 Dmean(cGy) 425.96±88.41 435.89±92.34 −0.830 0.420 脊髓外放0.5 cm Dmax(cGy) 2677.70±471.84 2681.10±506.08 −0.064 0.950 Dmean(cGy) 627.55±159.14 610.19±162.16 1.184 0.255 患者受照剂量 V5 Gy(%) 25.71±3.74 27.48±3.74 −2.465 0.026 注:FFF为非均整器;VMAT为容积旋转调强放疗;FF为均整器;Vx Gy为≥x Gy体积占总体积的百分比;Dmean为平均剂量;Dmax为最大剂量
下载: 导出CSV
-
[1] Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394−424. DOI: 10.3322/caac.21492. [2] Joseph B, Farooq N, Kumar S, et al. Breast-conserving radiotherapy with simultaneous integrated boost; field-in-field three-dimensional conformal radiotherapy versus inverse intensity-modulated radiotherapy — a dosimetric comparison: do we need intensity-modulated radiotherapy?[J]. South Asian J Cancer, 2018, 7(3): 163−166. DOI: 10.4103/sajc.sajc_82_18. [3] Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10 801 women in 17 randomised trials[J]. Lancet, 2011, 378(9804): 1707−1716. DOI: 10.1016/S0140-6736(11)61629-2. [4] Bartelink H, Horiot JC, Poortmans P, et al. Recurrence rates after treatment of breast cancer with standard radiotherapy with or without additional radiation[J]. N Engl J Med, 2001, 345(19): 1378−1387. DOI: 10.1056/NEJMoa010874. [5] Abdel-Qadir H, Austin PC, Lee DS, et al. A population-based study of cardiovascular mortality following early-stage breast cancer[J]. JAMA Cardiol, 2017, 2(1): 88−93. DOI: 10.1001/jamacardio.2016.3841. [6] Sakka M, Kunzelmann L, Metzger M, et al. Cardiac dose-sparing effects of deep-inspiration breath-hold in left breast irradiation: is IMRT more beneficial than VMAT?[J]. Strahlenther Onkol, 2017, 193(10): 800−811. DOI: 10.1007/s00066-017-1167-0. [7] Tang G, Earl MA, Luan S, et al. Comparing radiation treatments using intensity-modulated beams, multiple arcs, and single arcs[J]. Int J Radiat Oncol Biol Phys, 2010, 76(5): 1554−1562. DOI: 10.1016/j.ijrobp.2009.04.003. [8] Ha B, Suh HS, Lee J, et al. Long-term results of forward intensity-modulated radiation therapy for patients with early-stage breast cancer[J]. Radiat Oncol J, 2013, 31(4): 191−198. DOI: 10.3857/roj.2013.31.4.191. [9] Lechner W, Kragl G, Georg D. Evaluation of treatment plan quality of IMRT and VMAT with and without flattening filter using Pareto optimal fronts[J]. Radiother Oncol, 2013, 109(3): 437−441. DOI: 10.1016/j.radonc.2013.09.020. [10] Fu GS, Li MH, Song YX, et al. A dosimetric evaluation of flattening filter-free volumetric modulated arc therapy in nasopharyngeal carcinoma[J]. J Med Phys, 2014, 39(3): 150−155. DOI: 10.4103/0971-6203.139003. [11] Lim TY, Dragojević I, Hoffman D, et al. Characterization of the HalcyonTM multileaf collimator system[J/OL]. J Appl Clin Med Phys, 2019, 20(4): 106−114[2021-11-18]. https://aapm.onlinelibrary.wiley.com/doi/10.1002/acm2.12568. DOI: 10.1002/acm2.12568. [12] Spruijt KH, Dahele M, Cuijpers JP, et al. Flattening filter free vs flattened beams for breast irradiation[J]. Int J Radiat Oncol Biol Phys, 2013, 85(2): 506−513. DOI: 10.1016/j.ijrobp.2012.03.040. [13] Singla R, King S, Albuquerque K, et al. Simultaneous-integrated boost intensity-modulated radiation therapy (SIB-IMRT) in the treatment of early-stage left-sided breast carcinoma[J]. Med Dosim, 2006, 31(3): 190−196. DOI: 10.1016/j.meddos.2005.11.001. [14] Paddick I, Lippitz B. A simple dose gradient measurement tool to complement the conformity index[J]. J Neurosurg, 2006, 105 Suppl: S194−201. DOI: 10.3171/sup.2006.105.7.194. [15] Browne P, Beaton NR, Sharma H, et al. Identifying breast cancer patients who gain the most dosimetric benefit from deep inspiration breath hold radiotherapy[J]. J Med Radiat Sci, 2020, 67(4): 294−301. DOI: 10.1002/jmrs.415. [16] 刘穆平, 初磊, 邓煜, 等. 呼吸门控技术以及非均整模式应用于早期非小细胞肺癌小病灶立体定向放疗的优势[J]. 肿瘤预防与治疗, 2019, 32(8): 707−710. DOI: 10.3969/j.issn.1674-0904.2019.08.009.
Liu MP, Chu L, Deng Y, et al. Advantages of stereotactic body radiation therapy using flattening filter free techniques and active breathing control for early-stage non-small cell lung cancer with small lesions[J]. J Cancer Control Treat, 2019, 32(8): 707−710. DOI: 10.3969/j.issn.1674-0904.2019.08.009.[17] Li CQ, Chen JH, Zhu J, et al. Plan quality comparison for cervical carcinoma treated with Halcyon and Trilogy intensity-modulated radiotherapy[J/OL]. J Cancer, 2019, 10(24): 6135−6141[2021-11-18]. https://www.jcancer.org/v10p6135.htm. DOI: 10.7150/jca.32500. [18] Mancosu P, Castiglioni S, Reggiori G, et al. Stereotactic body radiation therapy for liver tumours using flattening filter free beam: dosimetric and technical considerations[J/OL]. Radiat Oncol, 2012, 7: 16[2021-11-18]. https://ro-journal.biomedcentral.com/articles/10.1186/1748-717X-7-16. DOI: 10.1186/1748-717X-7-16. [19] Fu WH, Dai JR, Hu YM, et al. Delivery time comparison for intensity-modulated radiation therapy with/without flattening filter: a planning study[J]. Phys Med Biol, 2004, 49(8): 1535−1547. DOI: 10.1088/0031-9155/49/8/011. [20] 贺先桃, 谭军文, 龙雨松, 等. 鼻咽癌FFF与FF模式下VMAT计划剂量学比较[J]. 中华放射肿瘤学杂志, 2018, 27(4): 401−405. DOI: 10.3760/cma.j.issn.1004-4221.2018.04.014.
He XT, Tan JW, Long YS, et al. Comparison of dosimetric characteristics between flattening-filter-free and flattening filter mode VMAT plans in nasopharyngeal carcinoma[J]. Chin J Radiat Oncol, 2018, 27(4): 401−405. DOI: 10.3760/cma.j.issn.1004-4221.2018.04.014.[21] 罗红樱, 周剑良, 单国平, 等. 左侧乳腺癌术后放疗无均整器模式剂量学优势分析[J]. 中国医学物理学杂志, 2021, 38(3): 281−286. DOI: 10.3969/j.issn.1005-202X.2021.03.003.
Luo HY, Zhou JL, Shan GP, et al. Dosimetric advantages of postoperative radiotherapy in flattening filter-free mode for left-sided breast cancer[J]. Chin J Med Phys, 2021, 38(3): 281−286. DOI: 10.3969/j.issn.1005-202X.2021.03.003.[22] Lai YQ, Chen YY, Wu SG, et al. Modified volumetric modulated arc therapy in left sided breast cancer after radical mastectomy with flattening filter free versus flattened beams[J]. Medicine (Baltimore), 2016, 95(14): e3295. DOI: 10.1097/MD.0000000000003295. [23] 李定杰, 刘如, 杨成梁, 等. 脑肿瘤立体定向放射外科中有无均整器模式剂量学比较[J]. 中华放射肿瘤学杂志, 2020, 29(1): 39−42. DOI: 10.3760/cma.j.issn.1004-4221.2020.01.009.
Li DJ, Liu R, Yang CL, et al. Dosimetric comparison between non-coplanar volumetric modulated arc therapy using flattening filter and flattening filter-free beams during stereotactic radiosurgery for brain tumors[J]. Chin J Radiat Oncol, 2020, 29(1): 39−42. DOI: 10.3760/cma.j.issn.1004-4221.2020.01.009.[24] Pokhrel D, Halfman M, Sanford L. FFF-VMAT for SBRT of lung lesions: improves dose coverage at tumor-lung interface compared to flattened beams[J]. J Appl Clin Med Phys, 2020, 21(1): 26−35. DOI: 10.1002/acm2.12764. [25] 张基永, 彭逊. 基于周围型肺癌高剂量率无均整滤过器模式下的2种动态适形弧计划比较[J]. 中南大学学报(医学版), 2021, 46(6): 615−619. DOI: 10.11817/j.issn.1672-7347.2021.200515.
Zhang JY, Peng X. Comparison of 2 dynamic conformal arc plans based on high-dose rate flattening filter free beams for peripheral lung cancer[J]. J Cent South Univ: Med Sci, 2021, 46(6): 615−619. DOI: 10.11817/j.issn.1672-7347.2021.200515.[26] 吴丽丽, 张基永, 黄宝添, 等. 非均整模式光子线在乳腺癌调强放疗的剂量学评估[J]. 中国医学物理学杂志, 2017, 34(11): 1086−1090. DOI: 10.3969/j.issn.1005-202X.2017.11.002.
Wu LL, Zhang JY, Huang BT, et al. Evaluation of intensity-modulated radiotherapy using flattening filter free photon beams for patients with breast cancer[J]. Chin J Med Phys, 2017, 34(11): 1086−1090. DOI: 10.3969/j.issn.1005-202X.2017.11.002.[27] Koivumäki T, Heikkilä J, Väänänen A, et al. Flattening filter free technique in breath-hold treatments of left-sided breast cancer: the effect on beam-on time and dose distributions[J]. Radiother Oncol, 2016, 118(1): 194−198. DOI: 10.1016/j.radonc.2015.11.032. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3346
- HTML全文浏览量: 2403
- PDF下载量: 8







