


-
SPECT/CT放射性核素骨显像是目前最能体现核医学影像技术优势且临床使用频率最高的核医学检查项目之一,约占单光子显像的63.1%[1]。超级骨显像是一种放射性核素骨显像的特殊影像学表现,其最初于1975年由Osmond等[2]提出,指全身骨骼显像中显像剂呈均匀、对称性异常放射性浓聚,骨骼显像异常清晰,而软组织内分布极低,双肾和膀胱不显影或仅隐约显影。超级骨显像见于多种良、恶性疾病,其中最常见于恶性肿瘤广泛性骨转移和代谢性骨病[3-5]。随着影像学技术的发展和仪器设备的革新,SPECT/CT实现了SPECT与CT的同机融合,既能反映病灶的骨盐代谢程度,又能清晰显示局部病灶的解剖结构、形态及骨质密度的改变,实现了“1+1>2”的优势。目前关于超级骨显像的研究多数仅为SPECT全身骨显像,而对SPECT/CT(即SPECT功能显像与CT解剖显像同机融合)的研究尚不成熟,也缺乏SPECT/CT显像结合患者的临床表现、实验室检查指标、病灶的解剖及密度等研究,不能完全体现不同病因导致的超级骨显像的特点。我们回顾性分析97例骨转移瘤和代谢性骨病患者的99Tcm-MDP SPECT/CT超级骨显像影像学特征、临床表现、年龄及实验室检查结果的差异,旨在提高临床医师对超级骨显像的认知。
-
选取2012年6月至2021年7月于宁夏医科大学总医院核医学科行99Tcm-MDP SPECT/CT的47 671例患者中呈超级骨显像的患者97例,其中男性54例、女性43例,年龄25~85(62.4±14.3)岁。对97例患者的临床表现资料、影像学资料、年龄及实验室检查资料进行回顾性分析。根据病因不同将患者分为2组:骨转移瘤组(71例)和代谢性骨病组(26例,包括甲状旁腺瘤9例、肾性骨病6例、骨质疏松症11例)。根据原发肿瘤不同,将71例骨转移瘤组患者分为4个亚组[前列腺癌组(40例)、乳腺癌组(15例)、肺癌组(8例)、消化系统恶性肿瘤组(8例,包括胃癌4例、直肠癌2例、食管癌1例、原发性肝癌1例)]。纳入标准:(1)经99Tcm-MDP SPECT显像诊断为超级骨显像,且阳性病灶行99Tcm-MDP SPECT/CT融合显像;(2)原发部位经组织病理学检查结果证实为恶性肿瘤或经临床诊断为代谢性骨病。排除标准:(1)临床资料不全者;(2)近期使用过唑来膦酸等影响MDP摄取的药物;(3)有外伤史。所有患者均知悉检查流程和注意事项,并于检查前签署了知情同意书。本研究符合《赫尔辛基宣言》的原则。
-
使用美国GE公司Discovery NM/CT 670 Pro型SPECT/CT仪,配备低能高分辨准直器,显像剂为99Tcm-MDP (钼-锝发生器由北京原子高科股份有限公司提供,MDP药盒由江苏原子医学研究所提供),严格按药盒说明书进行标记,放射化学纯度>95%。患者静脉注射7.4×108 Bq 99Tcm-MDP后,嘱患者饮水1 000~1 500 ml,多排尿,显像前尽量排空膀胱,3~5 h内行SPECT全身骨显像,采集速度10~20 cm/min、矩阵256×1024、放大倍数1。对全身骨显像所示阳性病灶进行局部单床位SPECT/CT融合显像,以180°步进式断层采集28帧图像,12 s/帧,能峰140 keV、窗宽20%、矩阵128×128、放大倍数1,采用仪器自带三维Flash迭代法重建,迭代次数8、子集4。随后行同机CT扫描,扫描参数:管电压130 kV、管电流120 mA、层厚3 mm、螺距0.8 mm、旋转速度1 s,采用滤波反投影法重建,再使用SPECT/CT仪自带SyngoMI VA70软件将图像融合。检查时患者取仰卧位,双探头同时采集前、后位图像。
-
由2位具有5年以上工作经验的核医学科主治以上医师共同阅片,分别对每例患者的SPECT全身骨显像图和SPECT/CT融合图进行判断,意见不一致时协商取得一致。
超级骨显像的诊断标准[6]。(1)均匀对称型(I型):全身骨显像放射性核素呈弥漫性摄取增加,分布基本均匀、对称;(2)灶性散在分布型(Ⅱ型):全身骨显像呈散在、多发的放射性核素分布浓集灶;(3)软组织的放射性核素分布极低,双侧肾脏基本不显影。满足(1)+(3)或(2)+(3)均诊断为超级骨显像。
SPECT/CT融合显像骨质破坏的诊断标准[7]。(1)溶骨型:放射性核素分布呈虫蚀状、穿凿骨质缺损、边缘不规则、界限不清晰。(2)成骨型:放射性核素分布呈结节状、斑点状、片状致密度增高,骨小梁紊乱、增厚、粗糙。(3)混合型:兼有上述2种表现。
-
显像前2周内,使用瑞士罗氏公司全自动电化学发光免疫分析仪(Cobase 601)测定患者血钙、血磷、碱性磷酸酶(alkaline phosphatase,ALP)、乳酸脱氢酶(lactate dehydrogenase,LDH)的水平。正常参考值:血钙2.25~2.75 mmol/L、血磷0.97~1.61 mmol/L、ALP (男性 45~125 U/L、女性 50~135 U/L)、LDH 120~250 U/L。
-
应用SPSS 26.0软件对数据进行统计学分析。符合正态分布的计量资料以
$\bar x $ ± s表示,方差齐的组间数据的比较采用独立样本t检验及单因素方差分析;非正态分布的计量资料以M(Q1,Q3)表示,组间的比较采用Wilcoxon秩和检验及Kruskal-Wallis H检验。分类变量(骨痛及骨质破坏类型)的比较采用χ2检验。P<0.05为差异有统计学意义。 -
超级骨显像的阳性率为0.2%(97/47 671),其中骨转移瘤占73.2%(71/97)、代谢性骨病占26.8%(26/97)。所有患者均以骨痛为初发症状,局部骨痛占56.7%(55/97)、无骨痛占30.9%(30/97)、全身骨痛占12.4%(12/97),局部骨痛患者中,腰痛较为常见,占49.1%(27/55)。所有患者均无外伤史。
-
由表1可知,骨转移瘤组以灶性散在分布型(Ⅱ型)为主(85.9%),代谢性骨病组主要呈均匀对称型( Ⅰ型,61.5%),99Tcm-MDP SPECT显像模式组间差异有统计学意义(χ2=21.84,P<0.001); 在SPECT/CT融合显像上,骨转移瘤组病灶多为成骨型或混合型骨质破坏(74.6%、19.7%),而代谢性骨病组病灶多为溶骨型骨质破坏(73.1%)。另外,所有代谢性骨病患者肾脏显影均不清,其中14例颅骨99Tcm-MDP摄取增加,形成“头盔征”;5例表现为肋骨“串珠征”;2例中轴骨99Tcm-MDP摄取增加;6例长骨99Tcm-MDP摄取增加;2例表现为胸骨“领带征”;4例关节周围区域99Tcm-MDP摄取增加。骨转移瘤(前列腺癌患者)及代谢性骨病(甲状旁腺瘤患者)的典型病例图像见图1、2。
组别 99Tcm-MDP SPECT 99Tcm-MDP SPECT/CT Ⅰ型 Ⅱ型 成骨型 溶骨型 混合型 骨转移瘤组(n=71) 10(14.1%) 61(85.9%) 53(74.6%) 4(5.7%) 14(19.7%) 代谢性骨病组(n=26) 16(61.5%) 10(38.5%) 5(19.2%) 19(73.1%) 2(7.7%) χ2值 21.84 43.74 P值 <0.001 <0.001 注:骨转移瘤组以成骨型和混合型骨质破坏为主,而代谢性骨病组以溶骨型骨质破坏为主,差异均有统计学意义(χ2=39.76、15.95,均 P<0.001)。MDP为亚甲基二膦酸盐;SPECT为单光子发射计算机体层摄影术;CT为计算机体层摄影术 表 1 骨转移瘤组与代谢性骨病组患者的影像学特征比较[例(%)]
Table 1. Comparison of imaging features between patients with bone metastases and metabolic bone disease (case(%))

图 1 前列腺癌患者(男性,71 岁)99Tcm-MDP SPECT全身骨显像和胸椎SPECT/CT 显像图
Figure 1. 99Tcm-MDP SPECT whole-body bone scan and thoracic vertebrae SPECT/CT fusion imaging in a patient (male, 71 years old) with prostate cancer

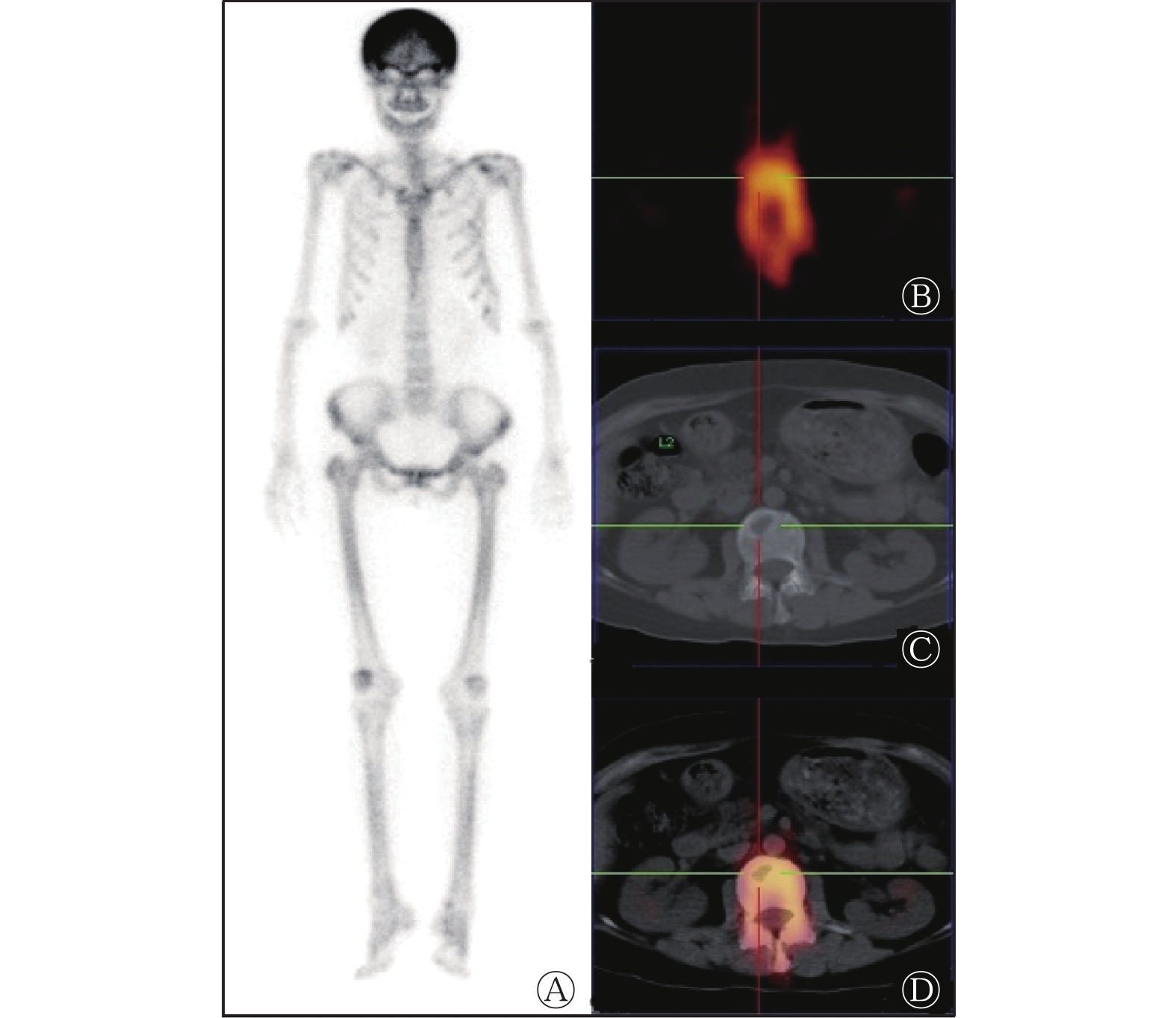
图 2 甲状旁腺瘤患者(女性,49岁)99Tcm-MDP SPECT 全身骨显像和腰椎SPECT/CT 显像图
Figure 2. 99Tcm-MDP SPECT whole-body bone scan and lumbar vertebrae SPECT/CT fusion imaging in a patient (female, 49 years old) with parathyroid adenoma
-
由表2可知,因病变部位不同,骨转移瘤组和代谢性骨病组患者临床表现的差异无统计学意义(P=0.356),局部骨痛的差异有统计学意义(P=0.008)。骨转移瘤组患者的局部骨痛主要为腰痛(60.0%),而代谢性骨病组患者以肋骨痛(40.0%)为主,差异有统计学意义(P=0.003)。由表3可知,骨转移瘤组患者年龄和ALP、LDH水平均高于代谢性骨病组,而血钙水平则低于代谢性骨病组,差异均有统计学意义(均P<0.05);而2组患者在血磷水平上的差异无统计学意义(P>0.05)。
组别 临床表现 局部骨痛 全身骨痛 局部骨痛 无骨痛 腰痛 肋骨痛 四肢痛 其他 骨转移瘤组(n=71) 7(9.9%) 40(56.3%) 24(33.8%) 24(60.0%) 3(7.5%) 6(15.0%) 7(17.5%) 代谢性骨病组(n=26) 5(19.2%) 15(57.7%) 6(23.1%) 3(20.0%) 6(40.0%) 4(26.7%) 2(13.3%) χ2值 2.09 10.88 P值 0.356 0.008 注:骨转移瘤组患者的局部骨痛主要为腰痛,而代谢性骨病组患者的局部骨痛主要为肋骨痛,差异有统计学意义(χ2=11.11,P=0.003) 表 2 骨转移瘤组与代谢性骨病组患者的临床表现和局部骨痛的比较[例(%)]
Table 2. Comparison of clinical manifestations and regional bone pain between patients with bone metastases and metabolic bone diseases (case(%))
组别 年龄( $\bar x \pm s $ 

血钙( $\bar x \pm s $ 

血磷( $\bar x \pm s $ 

ALP[M(Q1, Q3),U/L] LDH[M( Q1, Q3),U/L] 骨转移瘤组(n=71) 65.25±12.32 2.16±0.19 1.04±0.27 520.50(242.25, 1024.50) 338.00(193.50, 677.50) 代谢性骨病组(n=26) 50.85±14.26 2.59±0.35 1.04±0.67 284.35(138.65, 559.00) 172.00(111.25, 249.25) 检验值 t=4.89 t=−5.96 t=0.01 Z=−2.28 Z=−3.65 P值 <0.001 <0.001 0.990 0.023 <0.0001 注:由于14例患者实验室检查指标的水平与显像时间相差较大,且2组患者中有3例无ALP、LDH,故均未进行统计学分析,行统计学分析的患者例数:血钙和血磷各83例、ALP和LDH各80例。实验室检查指标的正常参考值:血钙2.25~2.75 mmol/L、血磷0.97~1.61 mmol/L、ALP (男性45~125 U/L、女性50~135 U/L)、LDH 120~250 U/L。ALP为碱性磷酸酶,LDH为乳酸脱氢酶 表 3 骨转移瘤组与代谢性骨病组患者年龄、实验室检查结果的比较
Table 3. Comparison of age and laboratory examination results between patients with bone metastases and metabolic bone diseases
-
由表4可知,骨转移瘤原发肿瘤中前列腺癌最常见,约占全部恶性肿瘤骨转移的56.3%(40/71),其次为乳腺癌,约占21.1%(15/71)。骨转移瘤组4个亚组患者的99Tcm-MDP SPECT全身骨显像显像模式及99Tcm-MDP SPECT/CT融合显像上骨质破坏类型的差异均无统计学意义(均P>0.05)。
组别 99Tcm-MDP SPECT 99Tcm-MDP SPECT/CT Ⅰ型 Ⅱ型 成骨型 溶骨型 混合型 前列腺癌组(n=40) 5(12.5%) 35(87.5%) 32(80.0%) 1(2.5%) 7(17.5%) 乳腺癌组(n=15) 1(6.7%) 14(93.3%) 9(60.0%) 2(13.3%) 4(26.7%) 肺癌组(n=8) 2(25.0%) 6(75.0%) 6(75.0%) 0 2(25.0%) 消化系统恶性肿瘤组(n=8) 2(25.0%) 6(75.0%) 6(75.0%) 1(12.5%) 1(12.5%) χ2值 2.71 5.12 P值 0.360 0.460 注:MDP为亚甲基二膦盐酸;SPECT为单光子发射计算机体层摄影术;CT为计算机体层摄影术 表 4 骨转移瘤组4个亚组患者的影像学特征的比较[例(%)]
Table 4. Comparison of imaging features among the four groups of bone metastases group (case (%))
由表5可知,骨转移瘤组4个亚组患者的主要临床表现和局部骨痛的差异均无统计学意义(均P>0.05)。由表6可知,骨转移瘤组4个亚组患者的年龄和实验室检查结果有所不同:乳腺癌患者年龄最小、前列腺癌患者年龄最大,乳腺癌患者血钙水平最高,肺癌患者LDH水平最高,4个亚组之间比较差异均有统计学意义(均P<0.05);4个亚组间血磷和ALP水平的差异均无统计学意义(均P>0.05)。
组别 临床表现 局部骨痛 全身骨痛 局部骨痛 无骨痛 腰痛 肋骨痛 四肢痛 其他 前列腺癌组(n=40) 3(7.5%) 24(60.0%) 13(32.5%) 15(62.5%) 0 6(25.0%) 3(12.5%) 乳腺癌组(n=15) 3(20.0%) 10(66.7%) 2(13.3%) 6(20.0%) 2(40.0%) 0(26.7%) 2(13.3%) 肺癌组(n=8) 0 4(50.0%) 4(50.0%) 1(25.0%) 1(25.0%) 0 2(50.0%) 消化系统恶性肿瘤组(n=8) 1(12.5%) 2(25.0%) 5(62.5%) 2(100%) 0 0 0 χ2值 8.71 13.07 P值 0.141 0.070 表 5 骨转移瘤组4个亚组患者临床表现和局部骨痛的比较[例(%)]
Table 5. Comparison of clinical manifestations and regional bone pain among the four groups of bone metastases group (case (%))
组别 年龄( $\bar x \pm s $ 

血钙( $\bar x \pm s $ 

血磷( $\bar x \pm s $ 

ALP[M(Q1, Q3), U/L] LDH[M(Q1, Q3), U/L] 前列腺癌组(n=40) 70.80±8.11 2.10±0.17 1.01±0.24 620.00(308.00, 1080.00) 264.00(189.00, 590.00) 乳腺癌组(n =15) 51.73±8.45 2.31±0.20 1.19±0.25 289.00(178.75, 517.75) 414.50(228.25, 728.50) 肺癌组(n=8) 60.75±10.60 2.21±0.12 1.08±0.20 1030.00(227.00, 1473.00) 886.00(684.00, 1215.00) 消化系统恶性肿瘤组( n=8) 67.38±17.34 2.07±0.14 0.88±0.40 533.50(136.50, 933.50) 149.50(112.25, 539.75) 检验值 F=14.43 F=5.13 F=2.41 H=6.28 H=13.47 P值 <0.001 0.003 0.077 0.099 0.004 注:由于14例患者实验室检查指标的水平与显像时间相差较大,且骨转移瘤组患者中有1例无ALP、LDH,故均未进行统计学分析,行统计学分析的患者例数:血钙和血磷各57例、ALP和LDH各56例。实验室检查指标的正常参考值:血钙 2.25~2.75 mmol/L、血磷0.97~1.61 mmol/L、ALP (男性 45~125 U/L、女性 50~135 U/L)、LDH 120~250 U/L。ALP为碱性磷酸酶,LDH为乳酸脱氢酶 表 6 骨转移瘤组4个亚组患者年龄、实验室检查结果的比较
Table 6. Comparison of age and laboratory examination results among the four groups of bone metastases group
-
超级骨显像是一种特殊的影像学表现,常见于恶性肿瘤骨转移、代谢性骨病[甲状旁腺功能亢进症、肾性骨营养不良症、Paget(佩吉特)病等]、血液系统疾病和其他少见疾病(如肥大性骨关节病、甲状腺功能亢进、骨纤维结构不良和肢端肥大症等)[8]。曾令鹏等[9]的研究结果显示,恶性肿瘤骨转移中约有1.3%可出现超级骨显像,其中前列腺癌最常见,其次是乳腺癌和肺癌,其他肿瘤如膀胱移行细胞癌、髓质甲状腺癌、小涎腺癌、尤因肉瘤、食管鳞状细胞癌和鼻咽癌等也可出现。本研究结果显示,在行99Tcm-MDP SPECT/CT显像的 47 671例患者中,超级骨显像的阳性率为0.2%,其中骨转移瘤最常见,占73.2%,其次为代谢性骨病。骨转移瘤原发肿瘤中前列腺癌最常见,约占全部恶性肿瘤骨转移的56.3%,其次为乳腺癌,约占21.1%,与上述研究结果一致。
一般在恶性肿瘤中晚期,血供丰富的骨骼成为最常见的转移组织之一[10],起初为局部骨转移,而后进展为全身多部位骨转移。在全身骨显像中表现为超级骨显像的患者均为全身多部位骨转移,SPECT全身骨显像以灶性散在分布型为主;而代谢性骨病钙磷代谢紊乱,SPECT全身骨显像多为均匀分布型。
在本研究中,所有代谢性骨病患者的肾脏显影均不清,其中14例颅骨99Tcm-MDP摄取增加,形成“头盔征”、5例肋骨“串珠征”、2例中轴骨99Tcm-MDP摄取增加、6例长骨99Tcm-MDP摄取增加、4例关节周围区域99Tcm-MDP摄取增加、2例胸骨“领带征”。肾脏显影不清晰或不显影与颅骨99Tcm-MDP摄取增加最常见。但是,SPECT全身骨显像对病灶解剖结构、密度及定位显示欠佳,因此,我们对阳性病灶再次行SPECT/CT融合显像。贺煜[11]的研究结果显示,SPECT/CT融合显像的灵敏度、特异度和准确率均明显高于全身骨显像。
不同病因的超级骨显像患者在SPECT/CT融合显像上表现不一。骨转移瘤的病理基础为恶性细胞通过释放细胞因子和生长因子等中断正常骨细胞的转换[12]。维持骨代谢平衡需要破骨细胞诱导的骨吸收和成骨细胞诱导的骨形成之间的动态平衡和耦合[13] 。肿瘤细胞可导致成骨细胞和破骨细胞的失衡,从而中断骨重建[14]。溶骨型骨转移的一个重要条件是破骨细胞的激活,最终诱导破骨细胞的形成,导致骨吸收。相反,成骨型骨转移由各种因子引起成骨细胞增殖、分化以及骨形成,刺激骨形成是骨转移形成的主要因素,从而会形成成骨细胞(或骨硬化)型转移灶[15-16]。本研究结果显示,骨转移瘤组病灶在SPECT/CT融合显像上多数为成骨型或混合型骨质破坏,其中前列腺癌患者中有80%为成骨型骨质破坏。但Fang和Xu[17]的研究结果显示,绝大多数恶性肿瘤患者骨转移为溶骨型骨质破坏,少数患者为成骨型骨质破坏,其中成骨型骨质破坏明显见于前列腺癌患者。本研究与上述研究结果不同,可能原因是本研究中前列腺癌样本量较其他肿瘤样本量大。代谢性骨病患者骨代谢增高,骨吸收增加,全身骨组织广泛脱钙,从而导致多数患者的SPECT/CT融合显像呈现溶骨型骨质破坏。但是有部分骨转移瘤患者与代谢性骨病患者的SPECT/CT融合图像不易区分,因此需要结合患者的临床表现及相关实验室检查指标加以鉴别。
骨转移瘤和代谢性骨病患者均以局部骨痛为主要临床表现,癌细胞浸润到骨组织或释放破骨细胞活化因子可导致骨损害,引起单部位或多部位骨痛,甚至骨折[18]。代谢性骨病呈高转化型骨病,也可引起骨痛。但是不同病因引起局部骨痛的具体部位有所不同。本研究中我们发现,骨转移瘤组和代谢性骨病组患者的主要临床表现分别为腰痛和肋骨痛。可能原因是骨转移优先累及红骨髓比较丰富的中轴骨,导致腰痛。而代谢性骨病为弥漫性骨代谢增高,首先引起较微弱的骨疼痛,由于肋骨较为薄弱,故多为肋骨痛。但由于30.9%的患者无骨痛表现,因此有时容易漏诊,需要结合相关实验室检查指标加以鉴别。
不同病因超级骨显像患者的实验室检查指标亦有所不同。曾令鹏等[9]通过分析58例患者的超级骨显像图发现,相较于代谢性骨病组,骨转移瘤组患者年龄一般较大,ALP水平较高,血钙水平较低,因此结合患者年龄和ALP、血钙水平鉴别2种病因的超级骨显像有一定的价值。本研究结果显示,骨转移瘤组患者年龄、ALP和LDH水平较高,而血钙水平较低,2组间的差异均有统计学意义;而血磷水平间的差异无统计学意义。在骨转移瘤组中,患者多为成骨型骨质破坏,骨的重建占优势,从而致使血液中钙减少。相反,代谢性骨病患者多为溶骨型骨质破坏,骨质溶解,骨内大量钙流失至细胞外液,超过了肾脏和肠道清除血钙的能力,使得血钙水平升高;另外,骨质疏松症、甲状旁腺功能亢进症、慢性肾功能衰竭均可导致钙、碳酸盐和磷酸盐外流[19-20]。因此,代谢性骨病患者的血钙水平高于骨转移瘤患者。由于钙磷代谢平衡,理论上应该得出骨转移瘤患者血磷水平升高,但是本研究结果显示,二者并无较大差别,且保持正常水平,其最可能的原因是血磷受患者自身饮食影响较大。麦家杰等[21]的研究结果显示, ALP水平能更好地反映成骨细胞代谢水平,由于骨转移瘤多为成骨型骨质破坏,因此骨转移瘤患者的ALP水平高于代谢性骨病患者,本研究与上述研究结果一致。在组织损伤后或在疾病状态下LDH的水平会升高,同时有研究者指出,LDH是已知的反映全身癌症负担的酶,可作为肿瘤生物标志物,反映肿瘤活动的强度以及预测预后[22-23]。本研究中我们发现,肺癌患者的LDH水平显著高于其他恶性肿瘤患者,可能原因是肺癌的恶性程度较大。LDH为糖酵解途径中的重要酶类,受肿瘤细胞坏死、代谢转换率加快、细胞膜通透性增加等因素影响[24]。
本研究尚有不足之处,尽管本研究已纳入近10年的样本,且本院为宁夏地区肿瘤患者的主要就诊医院,但总体样本量仍较小,期待更大样本量的SPECT/CT超级骨显像的临床分析。
综上所述,超级骨显像的病因多样,以骨转移瘤最常见,其次为代谢性骨病。不同病因超级骨显像患者的SPECT/CT及临床表现不同,骨转移瘤组在SPECT/CT上主要为灶性散在分布型(Ⅱ型)的成骨型骨质破坏;而代谢性骨病组主要为均匀对称型(I型)的溶骨型骨质破坏。所有患者均以局部骨痛为主要临床表现,骨转移瘤患者腰痛最常见,而代谢性骨病患者以肋骨痛为主。骨转移瘤患者年龄、ALP和LDH水平更高,而血钙则更低。SPECT/CT在骨转移瘤和代谢性骨病的超级骨显像鉴别中有一定价值。
利益冲突 所有作者声明无利益冲突
作者贡献声明 于亚萍负责数据的收集、论文的撰写;李永亮负责数据的收集与整理;冯蓓、姜杨宏岩负责图像的获取、数据的统计学分析;赵倩负责论文框架的设计、审核与校对
SPECT/CT超级骨显像影像学特征、临床表现、年龄及实验室检查指标的分析
Analysis of imaging features, clinical manifestations, age and laboratory examination indexes of SPECT/CT super bone scan
-
摘要:
目的 探讨99Tcm-亚甲基二膦酸盐(MDP) SPECT/CT超级骨显像患者的影像学特征、临床表现、年龄及实验室检查结果的差异。 方法 收集2012年6月至2021年7月于宁夏医科大学总医院行99Tcm-MDP SPECT/CT显像的47 671例患者中呈超级骨显像的97例患者,其中男性54例、女性43例,年龄25~85(62.4±14.3)岁,回顾性分析97例患者的临床表现资料、影像学资料、年龄及实验室检查资料。根据病因不同,将患者分为骨转移瘤组(71例)与代谢性骨病组(26例,包括甲状旁腺瘤9例、肾性骨病6例、骨质疏松症11例)。根据原发肿瘤不同,将71例骨转移瘤组患者分为4个亚组[前列腺癌组(40例)、乳腺癌组(15例)、肺癌组(8例)、消化系统恶性肿瘤组(8例,包括胃癌4例、直肠癌2例、食管癌1例、原发性肝癌1例)]。统计分析骨转移瘤组与代谢性骨病组以及骨转移瘤组4个亚组之间99Tcm-MDP SPECT全身骨显像的特征、SPECT/CT融合显像的特征、临床表现、年龄和实验室检查[血钙、血磷、碱性磷酸酶(ALP)、乳酸脱氢酶(LDH)]结果的差异。计量资料的组间比较采用独立样本t检验、单因素方差分析、Wilcoxon秩和检验及Kruskal-Wallis H检验;分类变量资料的组间比较采用χ2检验。 结果 骨转移瘤(73.2%,71/97)是导致超级骨显像的最常见病因[在其原发肿瘤中,前列腺癌较常见(56.3%,40/71)],其次为代谢性骨病(26.8%,26/97)。骨转移瘤组以灶性散在分布型(Ⅱ型)为主(85.9%,61/71),代谢性骨病组主要呈均匀对称型( Ⅰ型)(61.5%,16/26),2组比较差异有统计学意义(χ2=21.84,P<0.001)。骨转移瘤组以成骨型(74.6%,53/71)和混合型(19.7%、14/71)骨质破坏为主,而代谢性骨病组以溶骨型(73.1%,19/26)骨质破坏为主,差异均有统计学意义(χ2=39.76、15.95,均P<0.001)。所有患者均以骨痛为初发症状,局部骨痛为主要临床表现(56.7%,55/97)。骨转移瘤组以腰痛最常见(60.0%,24/40),代谢性骨病组多为肋骨痛(40.0%,6/15),2组比较差异有统计学意义(χ2=11.11,P<0.05)。骨转移瘤组患者的年龄和ALP、LDH水平均高于代谢性骨病组,而血钙水平则低于代谢性骨病组,差异均有统计学意义(t=4.89,Z=−2.28、−3.65,t=−5.96,均P<0.05);而2组患者在血磷水平上的差异无统计学意义(t=0.01,P>0.05)。骨转移瘤组4个亚组在SPECT全身骨显像的显像模式、SPECT/CT融合显像中的骨质破坏类型、临床表现、局部骨痛部位间的差异均无统计学意义(χ2=2.71~13.07,均P>0.05) 。骨转移瘤组4个亚组间进行比较,乳腺癌组患者年龄最小、前列腺癌组患者年龄最大,乳腺癌组患者血钙水平最高,肺癌组患者LDH水平最高,且差异均有统计学意义(F=14.43、5.13,H=13.47,均P<0.05);血磷和ALP水平的差异均无统计学意义(F=2.41,H=6.28,均 P>0.05)。 结论 超级骨显像病因中以骨转移瘤最常见,其次为代谢性骨病。2种病因超级骨显像患者在99Tcm-MDP SPECT全身骨显像、病灶处99Tcm-MDP SPECT/CT融合显像、临床表现、年龄及实验室检查结果方面均有差异,99Tcm-MDP SPECT/CT在2种病因超级骨显像的鉴别中有一定价值。 -
关键词:
- 体层摄影术,发射型计算机,单光子 /
- 体层摄影术,X线计算机 /
- 99m锝美罗酸盐 /
- 骨肿瘤 /
- 肿瘤转移 /
- 超级骨显像
Abstract:Objective To explore the differences in the imaging features, clinical manifestations, age, and laboratory examination results of patients who underwent 99Tcm-methylenediphosphonate (MDP) SPECT/CT super bone scan. Methods A total of 97 patients with super bone scan, including 54 males and 43 females, aged 25–85 (62.4±14.3) years, were recruited from 47 671 patients who underwent 99Tcm-MDP SPECT/CT imaging in the General Hospital of Ningxia Medical University from June 2012 to July 2021. The clinical manifestation, imaging, age, and laboratory examination data of the 97 patients were retrospectively analyzed. In accordance with different etiologies, the patients were divided into the bone metastases group (71 cases) and the metabolic bone disease group (26 cases, including parathyroid adenoma (9 cases), renal bone disease (6 cases), and osteoporosis (11 cases)). In accordance with the location of the primary tumor, 71 patients with bone metastases were divided into four subgroups (prostate cancer group (40 cases); breast cancer group (15 cases); lung cancer group (8 cases); malignant digestive system tumors (8 cases), including gastric cancer (4 cases), rectal cancer (2 cases), esophageal cancer (1 case) and primary liver cancer (1 case)). The differences in 99Tcm-MDP SPECT whole-body bone scan and SPECT/CT fusion imaging features, clinical manifestations, age, and laboratory examination (serum calcium, serum phosphorus, alkaline phosphatase (ALP), and lactate dehydrogenase (LDH)) results between the bone metastasis group and the metabolic bone disease group and among the four subgroups of the bone metastasis group were statistically analyzed. Independent samples t-test, one-way ANOVA, Wilcoxon rank sum test, and Kruskal-Wallis H test were used to compare measurement data, and χ2 test was applied to compare classified variable data. Results Bone metastases (73.2%, 71/97) were the most common cause of super bone scan (among the primary tumors, prostate cancer was more common (56.3%, 40/71), followed by metabolic bone disease (26.8%, 26/97)). The bone metastasis group mainly exhibited focal scattered distribution type (type Ⅱ, 85.9%, 61/71), and the metabolic bone disease group presented mainly homogeneous and symmetrical type (type Ⅰ, 61.5%, 16/26), and the difference between the two groups was statistically significant (χ2=21.84, P<0.001). Osteogenic (74.6%, 53/71) and mixed types (19.7%, 14/71) were the main types of bone destruction in the bone metastases group, while osteolytic type (73.1%, 19/26) was the main type of bone destruction in the metabolic bone disease group, and the differences were statistically significant (χ2=39.76, 15.95; both P<0.001). In all patients, bone pain was the first symptom, and regional bone pain was the main clinical manifestation (56.7%, 55/97). Low back pain was the most common symptom in the bone metastasis group (60.0%, 24/40) and rib pain was the most common symptom in the metabolic bone disease group (40.0%, 6/15) with a significant difference between the two groups (χ2=11.11, P<0.05). Patients with bone metastasis had higher age, serum ALP and LDH levels and lower serum calcium levels than patients with metabolic osteopathy with statistically significant differences (t=4.89; Z=−2.28, −3.65; t=−5.96; all P<0.05). However, there was no significant difference in serum phosphorus levels between the two groups (t=0.01, P>0.05). No significant differences in the types of bone destruction, clinical manifestations, and local bone pain sites in SPECT whole-body bone scan and SPECT/CT fusion imaging were found among the four subgroups of the bone metastasis group (χ2=2.71–13.07; all P>0.05). Among the four subgroups of the bone metastasis group, the patients with breast cancer had the lowest age and the highest serum calcium levels, the patients with prostate cancer had the highest age, and the patients with lung cancer had the highest LDH levels, the differences were statistically significant (F=14.43, 5.13; H=13.47; all P<0.05). There were no significant differences in serum phosphorus and ALP levels (F=2.41; H=6.28; both P>0.05). Conclusions Bone metastases, followed by metabolic bone disease, are the most common causes for super bone scan. There were differences in 99Tcm-MDP SPECT whole body bone scan, focal 99Tcm-MDP SPECT/CT fusion imaging, clinical manifestation, age, and laboratory examination results in patiens with the two etiologies of super bone scan. 99Tcm-MDP SPECT/CT has a certain value in the identification of the two etiologies by super bone scan. -
图 1 前列腺癌患者(男性,71 岁)99Tcm-MDP SPECT全身骨显像和胸椎SPECT/CT 显像图
Figure 1. 99Tcm-MDP SPECT whole-body bone scan and thoracic vertebrae SPECT/CT fusion imaging in a patient (male, 71 years old) with prostate cancer
图 2 甲状旁腺瘤患者(女性,49岁)99Tcm-MDP SPECT 全身骨显像和腰椎SPECT/CT 显像图
Figure 2. 99Tcm-MDP SPECT whole-body bone scan and lumbar vertebrae SPECT/CT fusion imaging in a patient (female, 49 years old) with parathyroid adenoma
表 1 骨转移瘤组与代谢性骨病组患者的影像学特征比较[例(%)]
Table 1. Comparison of imaging features between patients with bone metastases and metabolic bone disease (case(%))
组别 99Tcm-MDP SPECT 99Tcm-MDP SPECT/CT Ⅰ型 Ⅱ型 成骨型 溶骨型 混合型 骨转移瘤组(n=71) 10(14.1%) 61(85.9%) 53(74.6%) 4(5.7%) 14(19.7%) 代谢性骨病组(n=26) 16(61.5%) 10(38.5%) 5(19.2%) 19(73.1%) 2(7.7%) χ2值 21.84 43.74 P值 <0.001 <0.001 注:骨转移瘤组以成骨型和混合型骨质破坏为主,而代谢性骨病组以溶骨型骨质破坏为主,差异均有统计学意义(χ2=39.76、15.95,均 P<0.001)。MDP为亚甲基二膦酸盐;SPECT为单光子发射计算机体层摄影术;CT为计算机体层摄影术  下载: 导出CSV
下载: 导出CSV
表 2 骨转移瘤组与代谢性骨病组患者的临床表现和局部骨痛的比较[例(%)]
Table 2. Comparison of clinical manifestations and regional bone pain between patients with bone metastases and metabolic bone diseases (case(%))
组别 临床表现 局部骨痛 全身骨痛 局部骨痛 无骨痛 腰痛 肋骨痛 四肢痛 其他 骨转移瘤组(n=71) 7(9.9%) 40(56.3%) 24(33.8%) 24(60.0%) 3(7.5%) 6(15.0%) 7(17.5%) 代谢性骨病组(n=26) 5(19.2%) 15(57.7%) 6(23.1%) 3(20.0%) 6(40.0%) 4(26.7%) 2(13.3%) χ2值 2.09 10.88 P值 0.356 0.008 注:骨转移瘤组患者的局部骨痛主要为腰痛,而代谢性骨病组患者的局部骨痛主要为肋骨痛,差异有统计学意义(χ2=11.11,P=0.003)
下载: 导出CSV
表 3 骨转移瘤组与代谢性骨病组患者年龄、实验室检查结果的比较
Table 3. Comparison of age and laboratory examination results between patients with bone metastases and metabolic bone diseases
组别 年龄( $\bar x \pm s $ 血钙( $\bar x \pm s $ 血磷( $\bar x \pm s $ ALP[M(Q1, Q3),U/L] LDH[M( Q1, Q3),U/L] 骨转移瘤组(n=71) 65.25±12.32 2.16±0.19 1.04±0.27 520.50(242.25, 1024.50) 338.00(193.50, 677.50) 代谢性骨病组(n=26) 50.85±14.26 2.59±0.35 1.04±0.67 284.35(138.65, 559.00) 172.00(111.25, 249.25) 检验值 t=4.89 t=−5.96 t=0.01 Z=−2.28 Z=−3.65 P值 <0.001 <0.001 0.990 0.023 <0.0001 注:由于14例患者实验室检查指标的水平与显像时间相差较大,且2组患者中有3例无ALP、LDH,故均未进行统计学分析,行统计学分析的患者例数:血钙和血磷各83例、ALP和LDH各80例。实验室检查指标的正常参考值:血钙2.25~2.75 mmol/L、血磷0.97~1.61 mmol/L、ALP (男性45~125 U/L、女性50~135 U/L)、LDH 120~250 U/L。ALP为碱性磷酸酶,LDH为乳酸脱氢酶
下载: 导出CSV
表 4 骨转移瘤组4个亚组患者的影像学特征的比较[例(%)]
Table 4. Comparison of imaging features among the four groups of bone metastases group (case (%))
组别 99Tcm-MDP SPECT 99Tcm-MDP SPECT/CT Ⅰ型 Ⅱ型 成骨型 溶骨型 混合型 前列腺癌组(n=40) 5(12.5%) 35(87.5%) 32(80.0%) 1(2.5%) 7(17.5%) 乳腺癌组(n=15) 1(6.7%) 14(93.3%) 9(60.0%) 2(13.3%) 4(26.7%) 肺癌组(n=8) 2(25.0%) 6(75.0%) 6(75.0%) 0 2(25.0%) 消化系统恶性肿瘤组(n=8) 2(25.0%) 6(75.0%) 6(75.0%) 1(12.5%) 1(12.5%) χ2值 2.71 5.12 P值 0.360 0.460 注:MDP为亚甲基二膦盐酸;SPECT为单光子发射计算机体层摄影术;CT为计算机体层摄影术
下载: 导出CSV
表 5 骨转移瘤组4个亚组患者临床表现和局部骨痛的比较[例(%)]
Table 5. Comparison of clinical manifestations and regional bone pain among the four groups of bone metastases group (case (%))
组别 临床表现 局部骨痛 全身骨痛 局部骨痛 无骨痛 腰痛 肋骨痛 四肢痛 其他 前列腺癌组(n=40) 3(7.5%) 24(60.0%) 13(32.5%) 15(62.5%) 0 6(25.0%) 3(12.5%) 乳腺癌组(n=15) 3(20.0%) 10(66.7%) 2(13.3%) 6(20.0%) 2(40.0%) 0(26.7%) 2(13.3%) 肺癌组(n=8) 0 4(50.0%) 4(50.0%) 1(25.0%) 1(25.0%) 0 2(50.0%) 消化系统恶性肿瘤组(n=8) 1(12.5%) 2(25.0%) 5(62.5%) 2(100%) 0 0 0 χ2值 8.71 13.07 P值 0.141 0.070
下载: 导出CSV
表 6 骨转移瘤组4个亚组患者年龄、实验室检查结果的比较
Table 6. Comparison of age and laboratory examination results among the four groups of bone metastases group
组别 年龄( $\bar x \pm s $ 血钙( $\bar x \pm s $ 血磷( $\bar x \pm s $ ALP[M(Q1, Q3), U/L] LDH[M(Q1, Q3), U/L] 前列腺癌组(n=40) 70.80±8.11 2.10±0.17 1.01±0.24 620.00(308.00, 1080.00) 264.00(189.00, 590.00) 乳腺癌组(n =15) 51.73±8.45 2.31±0.20 1.19±0.25 289.00(178.75, 517.75) 414.50(228.25, 728.50) 肺癌组(n=8) 60.75±10.60 2.21±0.12 1.08±0.20 1030.00(227.00, 1473.00) 886.00(684.00, 1215.00) 消化系统恶性肿瘤组( n=8) 67.38±17.34 2.07±0.14 0.88±0.40 533.50(136.50, 933.50) 149.50(112.25, 539.75) 检验值 F=14.43 F=5.13 F=2.41 H=6.28 H=13.47 P值 <0.001 0.003 0.077 0.099 0.004 注:由于14例患者实验室检查指标的水平与显像时间相差较大,且骨转移瘤组患者中有1例无ALP、LDH,故均未进行统计学分析,行统计学分析的患者例数:血钙和血磷各57例、ALP和LDH各56例。实验室检查指标的正常参考值:血钙 2.25~2.75 mmol/L、血磷0.97~1.61 mmol/L、ALP (男性 45~125 U/L、女性 50~135 U/L)、LDH 120~250 U/L。ALP为碱性磷酸酶,LDH为乳酸脱氢酶
下载: 导出CSV
-
[1] 中华医学会核医学分会. 2020年全国核医学现状普查结果简报[J]. 中华核医学与分子影像杂志, 2020, 40(12): 747−749. DOI: 10.3760/cma.j.cn321828-20201109-00403.
Chinese Society of Nuclear Medicine. A brief report on the results of the national survey of nuclear medicine in 2020[J]. Chin J Nucl Med Mol Imaging, 2020, 40(12): 747−749. DOI: 10.3760/cma.j.cn321828-20201109-00403.[2] Osmond 3rd JD, Pendergrass HP, Potsaid MS. Accuracy of 99mTC-diphosphonate bone scans and roentgenograms in the detection of prostate, breast and lung carcinoma metastases[J]. Am J Roentgenol Radium Ther Nucl Med, 1975, 125(4): 972−977. DOI: 10.2214/ajr.125.4.972. [3] Manohar PR, Rather TA, Khan SH, et al. Skeletal metastases presenting as superscan on technetium 99m methylene diphosphonate whole body bone scintigraphy in different type of cancers: a 5-year retro-prospective study[J]. World J Nucl Med, 2017, 16(1): 39−44. DOI: 10.4103/1450-1147.181153. [4] Chatterjee P, Mukherjee A, Mitra D, et al. Superscan on methylene diphosphonate skeletal scintigraphy in prostatic adenocarcinoma: a common finding but rare etiology[J]. Indian J Nucl Med, 2017, 32(4): 369−371. DOI: 10.4103/ijnm.ijnm_95_17. [5] Liu SZ, Zhou X, Song A, et al. Super bone scan in osteopetrosis[J]. Endocr Pract, 2020, 26(11): 1390. DOI: 10.4158/EP-2020-0077. [6] 杨爱民, 王淑霞, 邓惠兴, 等. 放射性核素骨显像“超级影像”的特点[J]. 实用放射学杂志, 2007, 23(2): 236−237, 270. DOI: 10.3969/j.issn.1002-1671.2007.02.029.
Yang AM, Wang SX, Deng HX, et al. Characters of "super bone scan" in radionuclide bone imaging[J]. J Pract Radiol, 2007, 23(2): 236−237, 270. DOI: 10.3969/j.issn.1002-1671.2007.02.029.[7] 鲁智勇. 骨转移瘤的CT诊断分析与应用价值[J]. 医学理论与实践, 2013, 26(22): 3031−3032. DOI: 10.19381/j.issn.1001-7585.2013.22.060.
Lu ZY. CT diagnosis and application value of bone metastases[J]. J Med Theory Pract, 2013, 26(22): 3031−3032. DOI: 10.19381/j.issn.1001-7585.2013.22.060.[8] 李悦芃, 王芬, 茅江峰, 等. 全身疼痛-高碱性磷酸酶血症-超级骨显像: 恶性肿瘤骨转移一例[J]. 中华内分泌代谢杂志, 2017, 33(8): 696−698. DOI: 10.3760/cma.j.issn.1000-6699.2017.08.013.
Li YP, Wang F, Mao JF, et al. Generalized pain-hyperphosphatasemia-super bone scan: a case report of malignant tumor with bone metastasis[J]. Chin J Endocrinol Metab, 2017, 33(8): 696−698. DOI: 10.3760/cma.j.issn.1000-6699.2017.08.013.[9] 曾令鹏, 罗侃莹, 张庆, 等. 58例超级骨显像分析[J]. 中国临床医学影像杂志, 2020, 31(6): 446−449. DOI: 10.12117/jccmi.2020.06.017.
Zeng LP, Luo KY, Zhang Q, et al. Analysis of super bone imaging in 58 cases[J]. J Chin Clin Med Imaging, 2020, 31(6): 446−449. DOI: 10.12117/jccmi.2020.06.017.[10] 郝捷, 陈万青. 2012年中国肿瘤登记年报[M]. 北京: 军事医学科学出版社, 2012.
Hao J, Chen WQ. 2012 Chinese cancer registry annual report[M]. Beijing: Military Medical Science Press, 2012.[11] 贺煜. 单光子发射计算机断层成像/CT融合显像与全身骨显像在诊断单发骨转移瘤中的效能比较[J]. 山西医药杂志, 2020, 49(20): 2774−2775. DOI: 10.3969/j.issn.0253-9926.2020.20.018.
He Y. Comparison of single photon emission computed tomography/CT fusion imaging and whole-body bone imaging in the diagnosis of single bone metastases[J]. Shanxi Med J, 2020, 49(20): 2774−2775. DOI: 10.3969/j.issn.0253-9926.2020.20.018.[12] O'Sullivan GJ, Carty FL, Cronin CG. Imaging of bone metastasis: an update[J/OL]. World J Radiol, 2015, 7(8): 202−211[2021-07-28]. https://www.wjgnet.com/1949-8470/full/v7/i8/202.htm. DOI: 10.4329/wjr.v7.i8.202. [13] Chen X, Wang ZQ, Duan N, et al. Osteoblast-osteoclast interactions[J]. Connect Tissue Res, 2018, 59(2): 99−107. DOI: 10.1080/03008207.2017.1290085. [14] Xu S, Yang F, Liu RW, et al. Serum microRNA-139-5p is downregulated in lung cancer patients with lytic bone metastasis[J]. Oncol Rep, 2018, 39(5): 2376−2384. DOI: 10.3892/or.2018.6316. [15] Wang MN, Xia F, Wei YQ, et al. Molecular mechanisms and clinical management of cancer bone metastasis[J]. Bone Res, 2020, 8(1): 30. DOI: 10.1038/s41413-020-00105-1. [16] 瓦俄, 方珏敏, 许青. 成骨与溶骨性骨转移机制差异及靶向药物进展[J]. 现代肿瘤医学, 2017, 25(22): 3699−3703. DOI: 10.3969/j.issn.1672-4992.2017.22.038.
Wael A, Fang JM, Xu Q. Differences of osteoblastic and osteolytic bone metastases in molecular mechanisms and the advances in their targeted therapy[J]. J Mod Oncol, 2017, 25(22): 3699−3703. DOI: 10.3969/j.issn.1672-4992.2017.22.038.[17] Fang J, Xu Q. Differences of osteoblastic bone metastases and osteolytic bone metastases in clinical features and molecular characteristics[J]. Clin Transl Oncol, 2015, 17(3): 173−179. DOI: 10.1007/s12094-014-1247-x. [18] 孟祥玲. 前列腺癌骨髓转移继发骨髓纤维化1例分析[J]. 现代肿瘤医学, 2013, 21(9): 2116. DOI: 10.3969/j.issn.1672-4992.2013.09.66.
Meng XL. Bone marrow fibrosis secondary to bone marrow metastasis of prostate cancer: an analysis of 1 case[J]. J Mod Oncol, 2013, 21(9): 2116. DOI: 10.3969/j.issn.1672-4992.2013.09.66.[19] Bushinsky DA, Wolbach W, Sessler NE, et al. Physicochemical effects of acidosis on bone calcium flux and surface ion composition[J]. J Bone Miner Res, 1993, 8(1): 93−102. DOI: 10.1002/jbmr.5650080112. [20] 邱杰山, 张文华, 周子英, 等. 慢性肾脏病5期患者碳酸氢盐水平与矿物质和骨代谢异常的相关性分析[J]. 中国骨质疏松杂志, 2019, 25(7): 969−974. DOI: 10.3969/j.issn.1006-7108.2019.07.017.
Qiu JS, Zhang WH, Zhou ZY, et al. The correlation between bicarbonate level and mineral and bone metabolism abnormality in patients with stage 5 chronic kidney disease[J]. Chin J Osteopor, 2019, 25(7): 969−974. DOI: 10.3969/j.issn.1006-7108.2019.07.017.[21] 麦家杰, 张金山, 李志钊, 等. 血清碱性磷酸酶、Ca2+水平在肺癌早期骨转移诊断中的临床意义[J]. 中国中西医结合影像学杂志, 2019, 17(5): 484−488. DOI: 10.3969/j.issn.1672-0512.2019.05.013.
Mai JJ, Zhang JS, Li ZZ, et al. Clinical significance of serum ALP and Ca2+ level in the diagnosis of early bone metastasis of lung cancer[J]. Chin Imaging J Integr Tradit West Med, 2019, 17(5): 484−488. DOI: 10.3969/j.issn.1672-0512.2019.05.013.[22] Marais LC, Bertie J, Rodseth R, et al. Pre-treatment serum lactate dehydrogenase and alkaline phosphatase as predictors of metastases in extremity osteosarcoma[J]. J Bone Oncol, 2015, 4(3): 80−84. DOI: 10.1016/j.jbo.2015.09.002. [23] Liang HG, Ma D, Xu Y, et al. Elevated levels of pre-treatment lactate dehydrogenase are an unfavorable predictor factor in patients with EML4-ALK rearrangement non-small cell lung cancer treated with crizotinib[J/OL]. Cancer Manag Res, 2019, 11: 8191−8200[2021-07-28]. https://www.dovepress.com/elevated-levels-of-pre-treatment-lactate-dehydrogenase-are-an-unfavora-peer-reviewed-fulltext-article-CMAR. DOI: 10.2147/CMAR.S213572. [24] 王宇琛, 章春芝, 王大伟, 等. 血清CYfra21-1、LDH、NSE水平检测在肺癌患者辅助诊断中的应用[J]. 分子诊断与治疗杂志, 2020, 12(9): 1226−1229, 1233. DOI: 10.3969/j.issn.1674-6929.2020.09.024.
Wang YC, Zhang CZ, Wang DW, et al. Application of serum CYfra21-1, LDH and NSE levels in the auxiliary diagnosis of lung cancer[J]. J Mol Diagn Ther, 2020, 12(9): 1226−1229, 1233. DOI: 10.3969/j.issn.1674-6929.2020.09.024. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 4095
- HTML全文浏览量: 3478
- PDF下载量: 32
