



-
早期肺腺癌是指肿瘤长径≤30 mm的ⅠA期肺癌[1],其病理变化一般是从不典型腺瘤样增生进展为原位癌,再到微浸润性腺癌(minimally invasive adenocarcinoma,MIA)、浸润性腺癌(invasive adenocarcinoma,IAC),但少数肺腺癌却不经过这一变化过程,直接发展为侵袭性极强的IAC [2],因此,掌握肺腺癌的浸润性影像学特征,准确、及早地发现这一变化,尽早对患者进行手术至关重要。笔者根据病理亚型将101例早期肺腺癌患者分组并进行对照分析,复习相关文献,旨在提高临床医师对其影像学诊断及浸润性CT征象的认识。
-
回顾性分析2015年1月至2020年10月惠州市中心人民医院收治的经手术后组织病理学检查结果证实的101例肺腺癌患者的薄层CT影像学资料和临床资料,其中,男性42例、女性59例,年龄28~75(56.5±9.4)岁;95例无任何临床症状,为体检时意外发现,6例咳嗽、咳痰;10例有吸烟史。根据2011 年国际肺癌研究联合会、美国胸科学会、欧洲呼吸协会联合发布的肺腺癌国际多学科分类标准[3],将患者分为浸润前组(25例,包括不典型腺瘤样增生和原位癌)和浸润组(76例,包括MIA和IAC)。本研究经惠州市中心人民医院伦理委员会审批同意(编号:KYLL2020077),所有患者均于检查前签署了知情同意书。
纳入标准:(1) 临床分期为肺腺癌0期、ⅠA期;(2)肺结节长径≤30 mm;(3)有胸部薄层CT或靶向扫描相关影像学资料;(4)图像清晰、无呼吸伪影。排除标准:(1)已有转移;(2)无胸部薄层CT相关影像学资料;(3)图像不清晰、伪影面积大。
-
使用美国通用公司的64排LightSpeed VCT及荷兰飞利浦公司的MX16-slice 16排螺旋CT扫描仪行常规胸部CT平扫,参数:管电压120 kV、管电流300 mA、扫描层厚3 mm、层间距3 mm;吸气后屏气扫描,扫描范围从肺尖到肺底。91例患者行结节薄层CT重建,层厚1.25 mm、层间距1.25 mm;10例行结节小视野靶扫描,扫描视野15 cm、层厚1.25 mm、层间距0.625 mm。肺窗设置为窗宽1500 HU、窗位−550 HU,纵隔窗设置为窗宽350 HU、窗位65 HU。
-
薄层CT图像数据通过美国通用公司的ADW4.5肺结节软件进行分析,由2位3年以上主治医师在不知道组织病理学检查结果的情况下独立对图像进行测量、计算和分析,意见不一时,由主任医师指导、讨论后达成统一。基于肺窗对以下几个方面进行观察、测量和计算。(1)结节基本征象:形态、密度、内部特征(实性成分、支气管征、血管征、空泡征)、边缘特征(光整、分叶征、毛刺征、胸膜凹陷征);(2)测量和计算内容:结节长径、CT值、相对CT值、结节体积、CT值/体积的比值。
测量CT值时避开血管,纯磨玻璃结节(pure ground-glass nodule,pGGN )和实性结节的CT值选取3个ROI,计算均值;混合磨玻璃结节(mixed ground-glass nodule, mGGN)的CT值=pGGN成分比例×pGGN CT值+实性结节比例×实性结节CT值;相对CT值=结节CT值−邻近正常肺CT值。
-
pGGN:高于肺、低于邻近血管密度,内可见支气管影、血管影;实性结节:高于或等于邻近血管密度;mGGN:磨玻璃内部出现实性成分,需排除血管影所致[4]。支气管:支气管分级0级为正常,1级为扩张,2级为管壁增厚、毛糙,3级为狭窄、中断;血管束:血管分级0级为正常,1级为增粗、模糊,2级为扭曲、血管壁不光整、僵硬,3级为正常血管破坏且显示不清[5-6]。
-
应用SPSS21.0软件进行统计学分析。符合正态分布的计量资料以
$ \bar x $ ±s表示,组间比较采用独立样本t检验;非正态分布的计量资料以M(Q1,Q3)表示,组间比较采用Mann-Whitney U检验;计数资料的组间比较采用χ2检验或Fisher确切概率法。P<0.05为差异有统计学意义。通过ROC曲线及AUC预测诊断效能,使用约登指数确定最佳临界值。对AUC诊断效能进行分级:0.5~0.7为较低,0.7~0.9为中等,>0.9为较高。 -
浸润前组有男性11例、女性14例,浸润组有男性31例、女性45例,2组患者的性别分布差异无统计学意义(χ2=0.08,P=0.778);浸润组患者的年龄大于浸润前组,且差异有统计学意义[(59.4±9.8)岁对(53.6±9.0)岁,t=2.86,P=0.007]。浸润组中有5例患者的癌胚抗原(carcinoembryonic antigen,CEA)水平升高(平均升高约2.8 μg/L),与非浸润组的差异无统计学意义(Fisher确切概率法,P=0.329)。
-
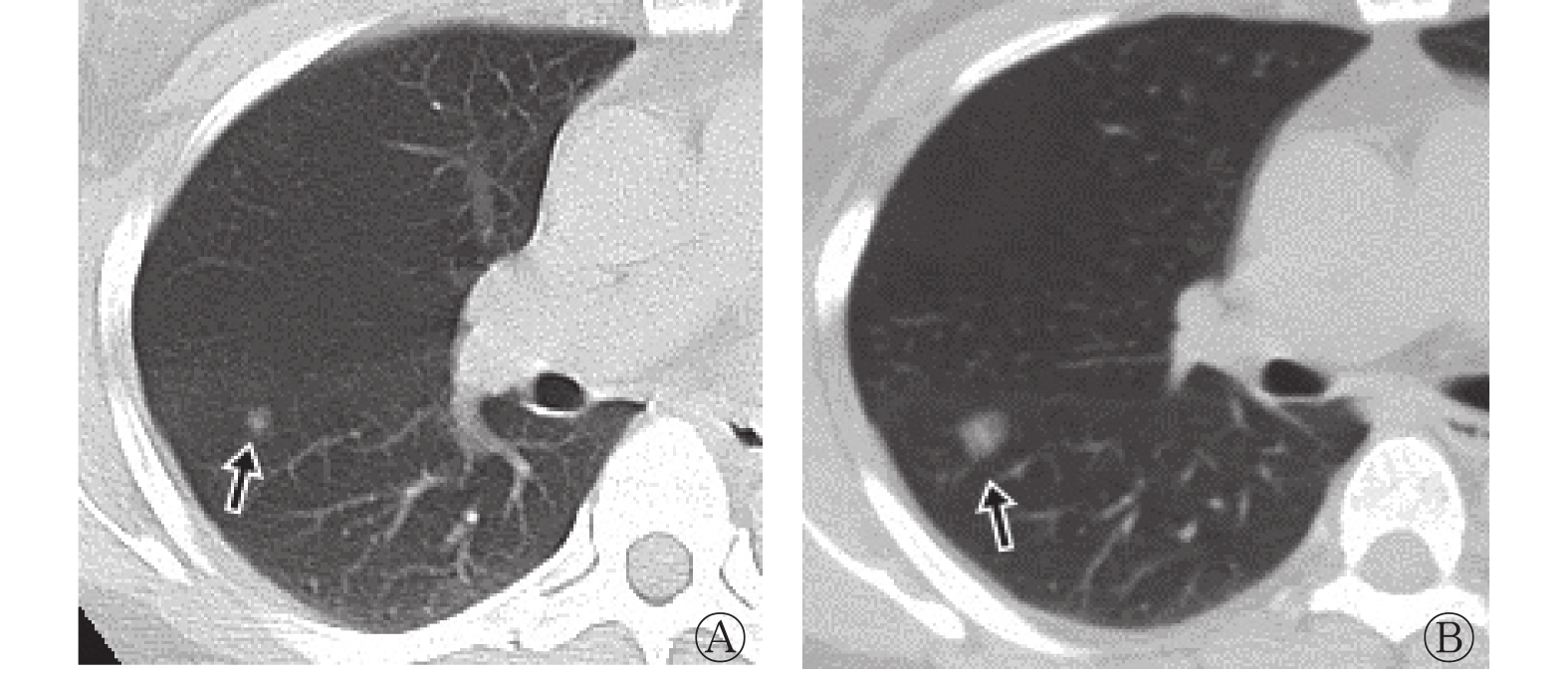
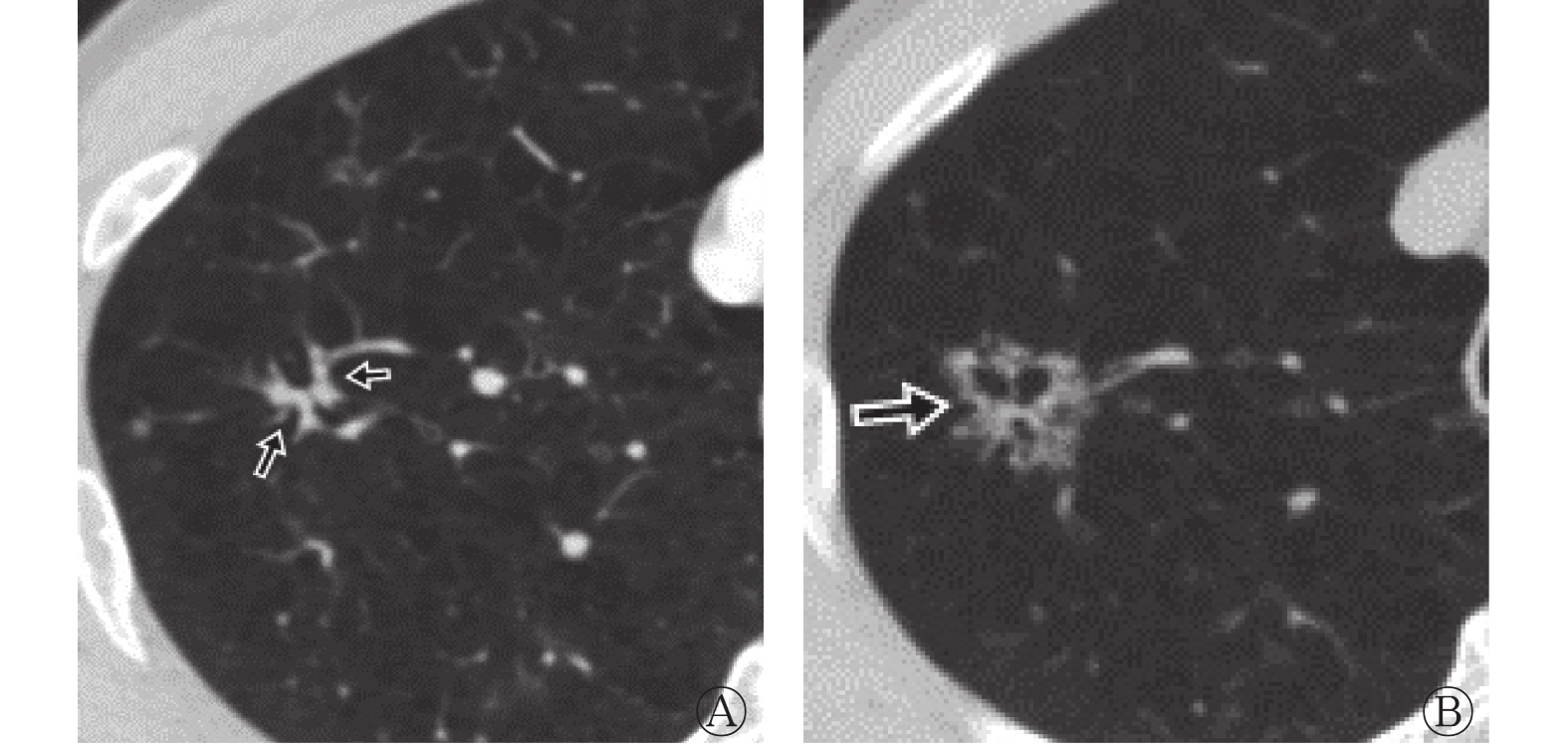
浸润前组25例患者中CT表现为pGGN 20例(80.0%)、mGGN 5例(20.0%);结节形态不规则2例、卵圆形23例;边缘光整17例(图1)、浅分叶征8例;空泡征2例、1级血管征4例(图2)、1级支气管征1例。

图 1 右肺上叶后段原位肺腺癌患者(女性,47岁)的薄层CT图
Figure 1. The thin-slice CT images of a patient (female, 47 years old) with adenocarcinoma in situ in the posterior segment of upper lobe of the right lung

图 2 右肺下叶背段微浸润肺腺癌患者(女性,44岁)的薄层CT图
Figure 2. The thin-slice CT images of a patient (female, 44 years old) with a microinvasive adenocarcinoma in the dorsal segment of lower lobe of the right lung
浸润组76例患者中CT表现为pGGN 13例(17.1%)、mGGN 26例(34.2%)、实性结节 37例(48.7%);形态不规则8例[其中4例沿支气管血管束生长(图3)]、卵圆形68例;分叶征56例、毛刺征54例、胸膜凹陷征36例;空泡征25例(图3B),支气管征:1级3例、2级7例、3级10例,血管征:1级20例、2级10例、3级3例。

图 3 右肺上叶浸润肺腺癌患者(男性,71岁)的薄层CT图
Figure 3. The thin-slice CT images of a patient (male, 71 years old) with invasive adenocarcinoma in the upper lobe of the right lung
-
由表1可知,结节的形态组间差异无统计学意义(P>0.05);浸润组患者结节内部出现实性成分、支气管征、血管征、空泡征的概率均高于浸润前组(均P<0.05);浸润前组患者结节边缘光整的概率高于浸润组(P<0.001),浸润组患者结节边缘出现分叶征、毛刺征、胸膜凹陷征的概率均高于浸润前组(均P<0.001)。由表2可知,与浸润前组比较,浸润组患者结节的CT值、结节体积、CT值/体积的比值、结节长径均较大,而相对CT值较小,且差异均有统计学意义(均P<0.001)。
组别 形态(规则/不规则) 实性成分 支气管征 血管征 空泡征 边缘特征 光整 分叶征 毛刺征 胸膜凹陷征 浸润前组(n=25) 23(92.0)/2(8.0) 5(20.0) 1(4.0) 4(16.0) 2(8.0) 17(68.0) 8(32.0) 0 0 浸润组(n=76) 68(89.5)/8(10.5) 63(82.9) 20(26.3) 33(43.4) 25(32.9) 8(10.5) 56(73.7) 54(71.1) 36(47.4) χ2值 0.00 33.82 4.14 4.97 4.75 33.36 14.08 − − P值 1.000 <0.001 0.036 0.026 0.029 <0.001 <0.001 <0.001 <0.001 注:−表示采用Fisher确切概率法,无检验值。CT为计算机体层摄影术 表 1 浸润前组与浸润组肺腺癌患者的CT征象比较[例(%)]
Table 1. Comparison of CT features of patients with lung adenocarcinoma between pre-invasion group and invasive group [case (%)]
组别 CT值(HU) 相对CT值(HU) 结节体积(cm3) CT值/体积的比值 结节长径(mm) 浸润前组(n=25) −537.00(−612.00, −418.00) −289.00(−412.00,−210.50) 0.18(0.14, 0.26) −2685.00(−3564.00, −1972.00) 7.50(6.50, 8.25) 浸润组(n=76) −61.00(−318.25, 21.50) −758.50(−839.00, −534.25) 0.86(0.44, 2.16) −48.19(−422.14, 12.80) 13.00(11.00, 16.00) Z值 −5.82 −5.71 −5.43 −6.51 −6.03 P值 <0.001 <0.001 <0.001 <0.001 <0.001 注:相对CT值=结节CT值−邻近正常肺CT值。CT为计算机体层摄影术 表 2 浸润前组与浸润组肺腺癌患者的CT定量参数比较 [M(Q1,Q3)]
Table 2. Comparison of CT quantitative parameters of patients with lung adenocarcinoma between pre-invasion group and invasive group[M (Q1, Q3)]
由图4可见,浸润前病变与浸润性病变的最佳临界值:当结节长径≥8.75 mm时,灵敏度为87.5%、特异度为84.0%;当结节体积≥0.31 cm3时,灵敏度为82.9%、特异度为88.0%;当CT值为−464 HU时,灵敏度为89.5%、特异度为72.0%;当CT值/体积的比值为−1681.7时,灵敏度为93.4%、特异度为88.0%。结节长径、CT值、结节体积、CT值/体积的比值的AUC分别为0.902(95%CI:0.843~0.962)、0.889(95%CI:0.824~0.955)、0.863(95%CI:0.784~0.942)、0.936(95%CI:0.886~0.985)。

图 4 结节长径、结节体积、CT值、CT值/体积的比值鉴别浸润前与浸润性肺腺癌病变的受试者工作特征曲线
Figure 4. Receiver operating characteristic curves of the long diameter, volume, CT value, and CT value/volume ratio of the lesions distinguishing pre-invasion and invasive lung adenocarcinoma lesions
-
早期肺腺癌在从浸润前病变发展为MIA、IAC的过程中,肿瘤不断增大、变实,其侵袭性也逐步增强。CT值是鉴别浸润前病变与浸润性病变的重要指标,有研究结果显示临界CT值范围为−500~−400 HU[1],本研究结果显示,最佳临界CT值为−464 HU,浸润组的CT值大于浸润前组,差异有统计学意义,与李琼等[7]的研究结果相近。Lee等[8]认为,可将结节长径为10 mm作为诊断浸润前病变与浸润性病变的临界值,贾承晔等[9]认为,结节长径的最佳临界值为11.4 mm。本研究结果显示,浸润组的结节在长径、体积方面均大于浸润前组(均P<0.001),当结节长径≥8.75 mm时,该病变具有浸润倾向的可能性大;结节的密度不同,肿瘤是否存在浸润倾向的临界值也不同。CT值/体积的比值反映的是单位体积内的CT值,一般情况下,比值越大,结节内部的肿瘤细胞密度越大。本研究结果显示,浸润组的CT值/体积的比值大于浸润前组(P<0.001),当CT值/体积比值≥−1681.7时,提示浸润性病变的可能性大。本研究结果提示,结节长径、CT值/体积比值具有高效的诊断效能(AUC>0.9),CT值、结节体积也具有中等的诊断效能(AUC>0.8)。
实性成分的大小和所占比例对判断mGGN是否具有浸润倾向有重要意义。大量研究结果显示,MIA、IAC结节内部的实性成分是肿瘤浸润性成分及塌陷的肺泡,实性成分比例越高,其浸润性可能越大[10-11]。有研究结果显示,若结节的实性成分长径≥6 mm,则高度提示IAC[12]。本研究结果显示,浸润前组pGGN占80.0%、mGGN占20.0%;浸润组pGGN占17.1%、mGGN占34.2%、实性结节占48.7%,浸润组实性成分显著多于浸润前组,与以上研究结果基本一致。
随着肿瘤侵袭性的增强,内部正常血管、支气管逐渐受到侵犯、破坏。浸润前病变由于没有侵犯间质及血管,内部常常可见正常血管穿行,有时病灶边缘可见血管阻挡征,即pGGN生长受正常血管阻挡形成平直血管边缘,但当肿瘤进展为MIA、IAC时,肿瘤实性成分增多,细胞密度增大,血供需求增加,导致异形血管增多、正常血管增粗或被破坏[2, 13]。在本研究中,浸润组有43.4%的结节出现血管征,浸润前组有16.0%的结节可见血管征,且均为1级表现,浸润组出现血管征的概率高于浸润前组(P<0.05),与以往文献报道[2, 13]基本一致。支气管征早期可表现为支气管扩张、管壁增厚或毛糙,最后出现管腔狭窄,甚至中断;有研究结果显示,支气管壁增厚与肿瘤突破肺泡沿支气管浸润有关,是早期肺腺癌浸润性的重要征象[6]。在本研究中,浸润组中20例患者的结节内部可见支气管征,而浸润前组仅有1例,2组间差异有统计学意义。以上结果表明,支气管征级别越高,浸润性病变的可能性越大。空泡(腔)是指肿瘤内部尚未破坏的肺泡、气道或支气管阻塞后过度充气的肺泡,常常位于肿瘤内部或边缘,且容易被误认为是空洞或肺大疱,随着肿瘤进展原有空泡(腔)被肿瘤占据而消失;在本研究中,浸润组出现空泡征的比例显著高于浸润前组,与文献报道[8, 14]相符。
分叶征、毛刺征及胸膜凹陷征是鉴别良恶性肺结节的重要影像学特征。我们认为,肺结节从浸润前病变发展为MIA、IAC,其病灶的边缘逐渐变得不光整,最后出现分叶征、毛刺征,二者的出现比例随浸润级别的升高而增加,与文献报道[14]一致。位于胸膜下的MIA、IAC易出现胸膜凹陷征,有研究者认为,胸膜凹陷征是由于肿瘤刺激周边纤维组织增生产生向心收缩力形成的,其恶性程度越大,出现比例越高[5, 15-16],甚至有学者认为,出现胸膜凹陷征就具有手术指征[17]。在本研究中,浸润组中47.4%患者的结节出现胸膜凹陷征,而浸润前组中并未有患者出现,差异有统计学意义。
肿瘤标志物对肺腺癌的诊断具有重要意义[18],对性质未明的肺结节,结合肿瘤标志物有助于提高肺腺癌术前诊断的准确率。在本研究中,浸润组有5例患者CEA水平升高,其中1例多次复查均表现出CEA水平升高,胸部CT检查结果显示,其肺内存在实性小结节,术后经组织病理学检查结果证实为IAC。但本研究中患者的CEA水平在组间的差异无统计学意义,出现这一情况的原因可能是样本量太小,早期肺腺癌CEA水平升高的概率较小。因此,早期肺腺癌患者血清肿瘤标志物水平不一定升高,但出现持续升高具有提示意义。
本研究也存在一定的局限性:(1)本研究为单中心、回顾性分析,存在选择性偏倚;(2)样本量较小,且2组样本量不一致。
综上所述,早期肺腺癌的浸润性与其结节体积、密度、内部特征、边缘特征有关。在临床实际工作中,需多平面仔细观察相关征象,综合分析,有助于判断其是否具有浸润倾向。
利益冲突 所有作者声明无利益冲突
作者贡献声明 林红东负责论文的设计、研究过程的实施、数据的分析、论文的撰写;张志艳、叶新苗负责图像的分析、数据的收集;周玉祥负责论文的审阅
薄层CT对早期肺腺癌的浸润性征象分析
Analysis of invasive signs of early lung adenocarcinoma by thin-slice CT
-
摘要:
目的 探讨早期肺腺癌的浸润性CT征象,为临床选择合理的治疗方案提供依据。 方法 回顾性分析2015年1月至2020年10月惠州市中心人民医院收治的经手术后组织病理学检查结果证实的101例肺腺癌患者[男性42例、女性59例,年龄28~75(56.5±9.4)岁]的薄层CT影像学资料,包括结节内部特征(实性成分、血管征、支气管征、空泡征)、边缘特征(光整、分叶征、毛刺征、胸膜凹陷征)、结节长径、CT值、相对CT值、结节体积、CT值/体积的比值等。根据病理亚型将患者分为浸润前组(25例)和浸润组(76例),并对2组数据进行对照分析。 计量资料的比较采用Mann-Whitney U检验和独立样本t检验,计数资料的比较采用χ2检验或Fisher确切概率法,并绘制受试者工作特征(ROC)曲线,计算最佳临界值和曲线下面积(AUC)。 结果 浸润前组25例患者中有纯磨玻璃结节20例(80.0%)、混合磨玻璃结节5例(20.0%)。浸润组76例患者中有纯磨玻璃结节13例(17.1%)、混合磨玻璃结节26例(34.2%)、实性结节37例(48.7%)。浸润组患者结节内部出现实性成分、支气管征、血管征、空泡征的概率均高于浸润前组,且差异均有统计学意义[82.9%(63/76)对20.0%(5/25)、26.3%(20/76)对4.0%(1/25)、43.4%(33/76)对16.0%(4/25)、32.9%(25/76)对8.0%(2/25),χ2=4.14~33.82,均P<0.05]。浸润前组患者结节边缘光整的概率高于浸润组,且差异有统计学意义[68.0%(17/25)对10.5%(8/76),χ2=33.36,P<0.001],浸润组患者结节边缘出现分叶征、毛刺征、胸膜凹陷征的概率均高于浸润前组,且差异均有统计学意义[73.7%(56/76)对32.0%(8/25)、71.1%(54/76)对0、47.4%(36/76)对0,χ2=14.08、Fisher确切概率法,均P<0.001]。浸润前组与浸润组患者的结节长径[7.50(6.50, 8.25) mm对13.00(11.00, 16.00) mm]、CT值[−537.00(−612.00, −418.00) HU对−61.00(−318.25, 21.50) HU]、相对CT值[−289.00(−412.00, −210.50) HU对−758.50(−839.00, −534.25) HU]、结节体积[ 0.18(0.14, 0.26) cm3对 0.86(0.44, 2.16) cm3]、CT值/体积的比值[−2685.00(−3564.00, −1972.00)对−48.19(−422.14,12.80)]的差异均有统计学意义(Z=−6.51~−5.43,均P<0.001)。浸润前病变与浸润性病变的最佳临界值:当结节长径≥8.75 mm时,灵敏度为87.5%、特异度为84.0%;当结节体积≥0.31 cm3时,灵敏度为82.9%、特异度为88.0%;当CT值为−464 HU时,灵敏度为89.5%、特异度为72.0%;当CT值/体积的比值为−1681.7时,灵敏度为93.4%、特异度为88.0%。结节长径、CT值、结节体积、CT值/体积的比值的AUC分别为0.902(95%CI:0.843~0.962)、0.889(95%CI:0.824~0.955)、0.863(95%CI:0.784~0.942)、0.936(95%CI:0.886~0.985)。 结论 早期肺腺癌的浸润性CT征象与其结节体积、长径、密度、内部特征、边缘特征有关,需多平面仔细观察相关征象,综合分析,一旦发现其具有浸润倾向,应及早手术。 -
关键词:
- 肺腺癌 /
- 体层摄影术,X线计算机 /
- 肿瘤浸润 /
- 磨玻璃结节 /
- 征象
Abstract:Objective To investigate the invasive signs of early lung adenocarcinoma by thin-slice CT and to provide the basis for selecting rational clinical treatment. Methods Thin-slice CT findings of 101 patients (42 males and 59 females, aged 28–75 (56.5±9.4) years) with lung adenocarcinoma confirmed by surgical histopathology examination in Huizhou Central People's Hospital from January 2015 to October 2020 were retrospectively analyzed. The imaging characteristics of nodules including internal characteristics (solid component, vascular sign, bronchial sign, and vacuole sign), marginal characteristics (smooth edges, lobulation sign, spiculated sign, and pleural indentation sign), long diameter, CT value, relative CT value, volume, and CT value/volume ratio. According to pathological subtypes, 25 patients were classified into the pre-invasion group, and 76 were classified into the invasive group. Two groups were compared, and Mann-Whitney U test and independent sample t test were used to compare the measurement data. χ2 test and Fisher's exact probability method were used for counting data comparison. Receiver operating characteristic curves were drawn and the optimal critical value and the area under the curve (AUC) were calculated. Results The pre-invasion group (25 cases) had 20 cases (80.0%) of pure ground-glass nodules and 5 cases (20.0%) of mixed ground-glass nodules. The invasion group (76 cases) had 13 cases (17.1%) of pure ground-glass nodules, 26 cases (34.2%) of mixed ground-glass nodules, and 37 cases (48.7%) of solid nodules. The probability of the internal characteristics of nodules including solid components, vascular signs, bronchial signs, and vacuole signs in the invasion group were significantly higher than that in the pre-invasion group (82.9% (63/76) vs. 20.0% (5/25), 26.3% (20/76) vs. 4.0% (1/25), 43.4% (33/76) vs. 16.0% (4/25), 32.9% (25/76) vs. 8.0% (2/25); χ2=4.14–33.82; all P<0.05). The probability of smooth edges in the pre-invasion group was significantly higher than that in the invasion group (68.0% (17/25) vs. 10.5% (8/76), χ2=33.36, P<0.001). The probability of lobulation signs, spiculated signs, and pleural indentation signs in the invasion group were significantly higher than that in the pre-invasion group (73.7% (56/76) vs. 32.0% (8/25), 71.1% (54/76) vs. 0, 47.4% (36/76) vs. 0; χ2=14.08, Fisher's exact probability method; all P<0.001). Statistically significant differences existed in long diameter (7.50 (6.50, 8.25) mm vs. 13.00 (11.00, 16.00) mm), CT value (−537.00 (−612.00, −418.00) HU vs. −61.00 (−318.25, 21.50) HU), relative CT value (−289.00 (−412.00, −210.50) HU vs. −758.50 (−839.00, −534.25) HU), volume (0.18 (0.14, 0.26) cm3 vs. 0.86 (0.44, 2.16) cm3), CT value/volume ratio (−2685.00 (−3564.00, −1972.00) vs. −48.19 (−422.14, 12.80)) between pre-invasion group and invasion group (Z=−6.51 to −5.43; all P<0.001). Optimal cutoff values existed between the pre-invasive and invasive lesions. When the long diameter of nodules was ≥8.75 mm, the sensitivity and specificity were 87.5% and 84.0%, respectively. When the nodule volume was ≥0.31 cm3, the sensitivity and specificity were 82.9% and 88.0%, respectively. When the CT value was −464 HU, the sensitivity and specificity were 89.5% and 72.0%, respectively. When the CT value/volume ratio was −1681.7, the sensitivity and specificity were 93.4% and 88.0%, respectively. The AUC of long diameter, CT value, volume, and CT value/volume ratio of nodules were 0.902 (95%CI: 0.843–0.962), 0.889 (95%CI: 0.824–0.955), 0.863 (95%CI: 0.784–0.942), and 0.936 (95%CI: 0.886–0.985), respectively. Conclusions CT findings of the invasion signs of early lung adenocarcinoma are related to the volume, length, density, internal characteristics, and marginal characteristics of the nodules. The relevant signs need to be carefully observed in multiple planes and for a comprehensive analysis. Once found that it has a tendency to infiltrate, it should be operated as soon as possible. -
Key words:
- Adenocarcinoma of lung /
- Tomography, X-ray computed /
- Neoplasm invasiveness /
- Ground-glass nodule /
- Sign
-
图 1 右肺上叶后段原位肺腺癌患者(女性,47岁)的薄层CT图
Figure 1. The thin-slice CT images of a patient (female, 47 years old) with adenocarcinoma in situ in the posterior segment of upper lobe of the right lung
图 2 右肺下叶背段微浸润肺腺癌患者(女性,44岁)的薄层CT图
Figure 2. The thin-slice CT images of a patient (female, 44 years old) with a microinvasive adenocarcinoma in the dorsal segment of lower lobe of the right lung
图 3 右肺上叶浸润肺腺癌患者(男性,71岁)的薄层CT图
Figure 3. The thin-slice CT images of a patient (male, 71 years old) with invasive adenocarcinoma in the upper lobe of the right lung
图 4 结节长径、结节体积、CT值、CT值/体积的比值鉴别浸润前与浸润性肺腺癌病变的受试者工作特征曲线
Figure 4. Receiver operating characteristic curves of the long diameter, volume, CT value, and CT value/volume ratio of the lesions distinguishing pre-invasion and invasive lung adenocarcinoma lesions
表 1 浸润前组与浸润组肺腺癌患者的CT征象比较[例(%)]
Table 1. Comparison of CT features of patients with lung adenocarcinoma between pre-invasion group and invasive group [case (%)]
组别 形态(规则/不规则) 实性成分 支气管征 血管征 空泡征 边缘特征 光整 分叶征 毛刺征 胸膜凹陷征 浸润前组(n=25) 23(92.0)/2(8.0) 5(20.0) 1(4.0) 4(16.0) 2(8.0) 17(68.0) 8(32.0) 0 0 浸润组(n=76) 68(89.5)/8(10.5) 63(82.9) 20(26.3) 33(43.4) 25(32.9) 8(10.5) 56(73.7) 54(71.1) 36(47.4) χ2值 0.00 33.82 4.14 4.97 4.75 33.36 14.08 − − P值 1.000 <0.001 0.036 0.026 0.029 <0.001 <0.001 <0.001 <0.001 注:−表示采用Fisher确切概率法,无检验值。CT为计算机体层摄影术  下载: 导出CSV
下载: 导出CSV
表 2 浸润前组与浸润组肺腺癌患者的CT定量参数比较 [M(Q1,Q3)]
Table 2. Comparison of CT quantitative parameters of patients with lung adenocarcinoma between pre-invasion group and invasive group[M (Q1, Q3)]
组别 CT值(HU) 相对CT值(HU) 结节体积(cm3) CT值/体积的比值 结节长径(mm) 浸润前组(n=25) −537.00(−612.00, −418.00) −289.00(−412.00,−210.50) 0.18(0.14, 0.26) −2685.00(−3564.00, −1972.00) 7.50(6.50, 8.25) 浸润组(n=76) −61.00(−318.25, 21.50) −758.50(−839.00, −534.25) 0.86(0.44, 2.16) −48.19(−422.14, 12.80) 13.00(11.00, 16.00) Z值 −5.82 −5.71 −5.43 −6.51 −6.03 P值 <0.001 <0.001 <0.001 <0.001 <0.001 注:相对CT值=结节CT值−邻近正常肺CT值。CT为计算机体层摄影术
下载: 导出CSV
-
[1] 张国桢, 蔡庆, 张伟强. 早期微小肺腺癌CT影像与病理的相关性[J]. 诊断学理论与实践, 2018, 17(5): 490−493. DOI: 10.16150/j.1671-2870.2018.05.002.
Zhang GZ, Cai Q, Zhang WQ. Correlation of CT imaging with pathological manifestations in early-stage micro-adenocarcinoma of lung[J]. J Diagn Concepts Pract, 2018, 17(5): 490−493. DOI: 10.16150/j.1671-2870.2018.05.002.[2] Liang J, Xu XQ, Xu H, et al. Using the CT features to differentiate invasive pulmonary adenocarcinoma from pre-invasive lesion appearing as pure or mixed ground-glass nodules[J]. Br J Radiol, 2015, 88(1053): 20140811. DOI: 10.1259/bjr.20140811. [3] Travis WD, Brambilla E, Noguchi M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma[J]. J Thorac Oncol, 2011, 6(2): 244−285. DOI: 10.1097/JTO.0b013e318206a221. [4] 中华医学会呼吸病学分会肺癌学组, 中国肺癌防治联盟专家组. 肺结节诊治中国专家共识(2018年版)[J]. 中华结核和呼吸杂志, 2018, 41(10): 763−771. DOI: 10.3760/cma.j.issn.1001-0939.2018.10.004.
Lung Cancer Group, Respiratory Branch, Chinese Medical Association, Expert Group of China Lung Cancer Prevention and Treatment Alliance. Chinese expert consensus on diagnosis and treatment of pulmonary nodules (2018 Edition)[J]. Chin J Tubere Respir Dis, 2018, 41(10): 763−771. DOI: 10.3760/cma.j.issn.1001-0939.2018.10.004.[5] 刘晨鹭, 蔡庆, 沈玉英, 等. 微小磨玻璃结节样肺腺癌的HRCT血管征研究[J]. 实用放射学杂志, 2018, 34(1): 31−34, 50. DOI: 10.3969/j.issn.1002-1671.2018.01.009.
Liu CL, Cai Q, Shen YY, et al. HRCT vascular sign research in tiny ground glass nodules-like lung adenocarcinoma[J]. J Pract Radiol, 2018, 34(1): 31−34, 50. DOI: 10.3969/j.issn.1002-1671.2018.01.009.[6] 高益萍, 黎良山, 沈志炜, 等. 肺结节CT靶扫描及重建技术对肺腺癌支气管改变的诊断价值分析[J]. 中国医学计算机成像杂志, 2019, 25(2): 129−132. DOI: 10.3969/j.issn.1006-5741.2019.02.008.
Gao YP, Li LS, Shen ZW, et al. Application of CT target scanning and reconstruction technique in evaluating bronchial changes of pulmonary nodules[J]. Chin Comput Med Imaging, 2019, 25(2): 129−132. DOI: 10.3969/j.issn.1006-5741.2019.02.008.[7] 李琼, 范丽, 顾亚峰, 等. 三维平均CT值和PET/CT最大标准化摄取值预测磨玻璃密度结节型肺腺癌侵袭性的研究[J]. 实用放射学杂志, 2016, 32(6): 867−870. DOI: 10.3969/j.issn.1002-1671.2016.06.011.
Li Q, Fan L, Gu YF, et al. A study of three-dimensional mean computed tomography value and maximum standardized uptake value for predicting pathological invasiveness in pulmonary adenocarcinoma patients with ground-glass nodules[J]. J Pract Radiol, 2016, 32(6): 867−870. DOI: 10.3969/j.issn.1002-1671.2016.06.011.[8] Lee SM, Park CM, Goo JM, et al. Invasive pulmonary adenocarcinomas versus preinvasive lesions appearing as ground-glass nodules: differentiation by using CT features[J]. Radiology, 2013, 268(1): 265−273. DOI: 10.1148/radiol.13120949. [9] 贾承晔, 杨署, 王宇辰, 等. 纯磨玻璃密度肺腺癌浸润前及浸润性病灶的高分辨率CT特征分析[J]. 实用放射学杂志, 2020, 36(1): 34−37. DOI: 10.3969/j.issn.1002-1671.2020.01.009.
Jia CY, Yang S, Wang YC, et al. HRCT findings of pre-invasive and invasive lung adenocarcinoma presented as pure ground-glass opacity[J]. J Pract Radiol, 2020, 36(1): 34−37. DOI: 10.3969/j.issn.1002-1671.2020.01.009.[10] 林栋, 于洋力, 陈晓桑, 等. 薄层CT参数与1~2 cm亚实性结节肺腺癌浸润程度及组织学亚型相关性分析: 单中心回顾性研究[J]. 中华胸心血管外科杂志, 2020, 36(9): 549−552. DOI: 10.3760/cma.j.cn112434-20200727-00348.
Lin D, Yu YL, Chen XS, et al. The association between the thin-section computed tomography parameters and the invasion and histological subtypes of subsolid nodules measuring 1−2 centimeters in diameter as lung adenocarcinoma: a retrospective study from one single center[J]. Chin J Thorac Cardiovasc Surg, 2020, 36(9): 549−552. DOI: 10.3760/cma.j.cn112434-20200727-00348.[11] 何小群, 罗天友, 李琦, 等. 浸润性肺腺癌不同病理亚型的临床病理及CT特征分析[J]. 第三军医大学学报, 2020, 42(19): 1950−1956. DOI: 10.16016/j.1000-5404.202004321.
He XQ, Luo TY, Li Q, et al. Clinicopathological characteristics and CT features of invasive adenocarcinoma of the lung with different pathological subtypes[J]. J Third Mil Med Univ, 2020, 42(19): 1950−1956. DOI: 10.16016/j.1000-5404.202004321.[12] 高丰, 葛虓俊, 李铭, 等. 不同病理类型肺部磨玻璃结节的CT诊断[J]. 中华肿瘤杂志, 2014, 36(3): 188−192. DOI: 10.3760/cma.j.issn.0253-3766.2014.03.006.
Gao F, Ge XJ, Li M, et al. CT diagnosis of different pathological types of ground-glass nodules[J]. Chin J Oncol, 2014, 36(3): 188−192. DOI: 10.3760/cma.j.issn.0253-3766.2014.03.006.[13] 康柳青, 黎海亮, 张孝先, 等. 磨玻璃密度肺腺癌内血管异常CT表现与病理亚型及磨玻璃分型的相关性[J]. 中国医学影像技术, 2018, 34(4): 548−552. DOI: 10.13929/j.1003-3289.201707059.
Kang LQ, Li HL, Zhang XX, et al. Correlation between CT manifestations of intramural vascular abnormalities and pathological subtypes, ground glass types in ground-glass opacity lung adenocarcinoma[J]. Chin J Med Imaging Technol, 2018, 34(4): 548−552. DOI: 10.13929/j.1003-3289.201707059.[14] 吴芳, 蔡祖龙, 田树平, 等. 1 cm以下磨玻璃密度肺腺癌的CT征象与病理亚型及免疫组织化学的相关性[J]. 中国医学科学院学报, 2015, 37(2): 163−170.
Wu F, Cai ZL, Tian SP, et al. Correlations between pathologic subtypes/immunohistochemical implication and CT characteristics of lung adenocarcinoma ≤1 cm with ground-glass opacity[J]. Acta Acad Med Sin, 2015, 37(2): 163−170.[15] Kobayashi Y, Sakao Y, Deshpande GA, et al. The association between baseline clinical-radiological characteristics and growth of pulmonary nodules with ground-glass opacity[J]. Lung Cancer, 2014, 83(1): 61−66. DOI: 10.1016/j.lungcan.2013.10.017. [16] 张峥, 李柏冬, 罗婷. 磨玻璃密度结节表现的浸润性肺腺癌的影像学特征[J]. 中国医科大学学报, 2019, 48(8): 762−764. DOI: 10.12007/j.issn.0258-4646.2019.08.020.
Zhang Z, Li BD, Luo T. Computed tomography features of invasive pulmonary adenocarcinomas appearing as ground-glass opacities[J]. J Chin Med Univ, 2019, 48(8): 762−764. DOI: 10.12007/j.issn.0258-4646.2019.08.020.[17] Ichinose J, Kohno T, Fujimori S, et al. Invasiveness and malignant potential of pulmonary lesions presenting as pure ground-glass opacities[J]. Ann Thorac Cardiovasc Surg, 2014, 20(5): 347−352. DOI: 10.5761/atcs.oa.13-00005. [18] 王一北, 陈宽冰, 张洪岩, 等. 血清肿瘤标记物对肺部结节的诊断价值[J]. 临床肺科杂志, 2017, 22(4): 598−601. DOI: 10.3969/j.issn.1009-6663.2017.04.005.
Wang YB, Chen KB, Zhang HY, et al. Value of serum tumor markers in diagnosis of pulmonary nodules[J]. J Clin Pulm Med, 2017, 22(4): 598−601. DOI: 10.3969/j.issn.1009-6663.2017.04.005. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3831
- HTML全文浏览量: 2972
- PDF下载量: 17
