




-
心脑血管疾病在我国较为常见,其因发病率高、致残率高、致死率高而广受重视[1]。研究结果表明,冠状动脉病变的程度与头颈动脉病变有着密切的关系,并且可能增加发生缺血性脑卒中的危险[1-5],因此,心脑血管疾病与动脉粥样硬化密切相关。当血管内存在易损斑块时,随时都有可能破裂而形成血栓,导致血流迅速中断,出现心脑血管急性事件,据统计,超过70%的心脑血管急性事件由此类斑块诱发[6]。同时行冠状动脉和头颈部动脉CT血管造影(CT angiography,CTA),即第三代双源低剂量CT心脑血管一体化成像,在保证图像质量的同时,显著降低了辐射剂量,具有较高的学术及应用价值。传统的心脑血管疾病的危险因素包括年龄、性别、超重与肥胖、吸烟史、高血压、总胆固醇水平和糖尿病等[2],然而约20%发生心脑血管急性事件的患者并无这些危险因素[6],Framingham风险评分作为近期发生恶性心脑血管事件预警模型的价值受到争议[3-8],临床上迫切需要更为准确的预警模型来预测发生心脑血管疾病的风险。
传统的多层螺旋CT行冠状动脉、头颈部动脉一体化成像的总辐射剂量高、对比剂用量大、操作费时且局限于低心率患者。如果能突破心率限制行心脑血管联合成像,一次完成3个部位的扫描,则可进一步降低辐射剂量和对比剂用量。随着影像技术的发展,这一问题逐渐被解决,心脑血管联合扫描一体化成像技术日益成熟,其优点显著:无创、操作简单快捷、大大降低了辐射剂量、可以迅速了解病情变化、准确性较高,其临床应用日益广泛。本研究拟通过第三代双源低剂量CT心脑血管一体化成像早期识别易损斑块,结合临床生化指标,建立心脑血管疾病发病风险预警模型,进一步提高早期预测心脑血管疾病发病风险的能力,为临床早期干预、降低心脑血管急性事件的发生率提供依据。
-
前瞻性选择2016年1月至2019年1月在包头市中心医院行第三代双源低剂量CT心脑血管一体化成像的患者,连续纳入614例。纳入标准:(1)有冠状动脉或脑血管疾病易患因素(糖尿病、高血脂、高血压、吸烟史、心脑血管疾病家族史等)的高危人群;(2)无CTA检查禁忌证;(3)了解 CTA 扫描及研究方案,并签署了知情同意书。排除标准:(1)有对比剂过敏史;(2)有严重肝、肾功能不全病史(肾小球滤过率<60 ml/min);(3)心功能不全;(4)安装起搏器;(5)患瓣膜病或其他心脏疾病,如心肌病或先天性心脏病;(6)各种病因的肺动脉高压;(7)怀孕或育龄、哺乳期妇女;(8)相关研究数据不全。本研究获得内蒙古医科大学伦理委员会的批准,文号为YKD2015061(包头市中心医院属于内蒙古医科大学的教学医院)。
根据排除标准,共排除15例患者。纳入研究的599例患者中,因在随访过程中失访99例,最终入组500例。其中,男性245例、女性255例;年龄(57.8±14.2)岁,年龄范围为43~72岁;体质指数为(25.70±3.58) kg/m2,范围为22.12~29.28 kg/m2;心率为(80.36±43.31)次/min,范围为37~124次/min。根据CTA特征,将500例患者分为易损斑块组200例、稳定斑块组97例和正常组203例;稳定斑块组和正常组合称为非易损斑块组(300例)。
-
患者均采用前瞻性心电门控大螺距扫描方式进行扫描。扫描仪为德国西门子第三代双源低剂量SOMATOM Force CT仪。探测器准直为2×192×0.6 mm,旋转时间为0.25 s,螺距为3.2,管电压采用 CARE kV 技术自动调节[9],管电流采用CARE Dose 4D技术自动调节。扫描前由扫描医师指导患者做呼吸训练,常规舌下给予硝酸甘油2喷。先行冠状动脉钙化评分扫描,然后实施心脑血管一体化联合增强扫描。扫描方向为从足向头;扫描范围从膈顶至颅顶(心脏+头颈部范围)。心率≤65次/min时,采用舒张期成像,即R-R间期(两次心跳之间的时间间隔)的55%;心率>65次/min时,采用收缩期成像,即R-R间期的30%。采用Bolus-tracking方法注射对比剂,使用双筒高压注射器(德国Ulrich Medical公司)以流率4.5 ml/s肘静脉注射碘海醇(美国GE公司的OmniPaque 350)50 ml,在升主动脉根部设置ROI(阈值为100 HU),峰值时间延迟8 s后开始扫描。
-
采用高级模拟迭代重建技术(德国西门子公司的Forchheim)进行后处理,原始数据传到工作站,采用Circulation软件(德国西门子公司)和软组织卷积核(B36f)(德国西门子公司)进行冠状动脉血管重建,有血管壁钙化者,采用锐利组织卷积核(B46)重建图像来补偿伪像。心血管图像经最大密度投影(maximum intensity projection,MIP)、曲面重建(curved planar reformation,CPR)、容积再现(volume rendering,VR)和心血管优化分析软件处理[9]。脑血管重建方法:采用数字减影血管造影系统自动去骨减影软件(德国西门子公司)行MIP及VR,重建层厚1 mm,间隔0.9 mm,卷积核D30f。
-
易损斑块的CTA特征[10-11]:(1)低CT衰减,CT值较低,范围为20~60 HU;(2)血管正性重构指数≥1.1;(3)点状钙化,明确显示为密集度较高的斑块,体积较小,周围有非钙化组织,最大径多在3 mm以下;(4)“餐巾环”征,表现为低密度斑块核心周围被高密度环环绕。稳定斑块的CTA特征是只含有钙化斑块。由2名副主任以上职称的从事心脑血管CT成像诊断的医师根据CTA特征判断其是否为易损斑块。采用Cohen's Kappa系数分析评价图像质量评分一致性:Kappa值>0.81为一致性极好;Kappa值在0.61~0.80为一致性良好;Kappa值在0.41~0.60为一致性中等;Kappa值在0.21~0.40为一致性一般;Kappa值<0.20为一致性差。
-
患者完成CTA检查后,对其随访6个月至2年。随访内容包括:(1)是否发生主要心脑血管不良事件(major adverse cardiovascular and cerebrovascular events,MACCE),包括心绞痛、心肌梗死、恶性心律失常、心源性猝死、脑血管意外等;(2)收集临床生化指标。
-
采用SPSS 20.0软件进行统计学分析。符合正态分布的计量资料以
$ \bar x \pm s$ 表示,多组间比较采用方差分析;呈偏态分布的计量资料以M (Q1,Q3)表示,两组间比较采用非参数U检验,多组间比较采用非参数Kruskal-Wallis检验。计数资料以率表示,组间比较采用卡方检验。采用多因素Logistic回归分析易损斑块与危险因素、MACCE等的相关性。易损斑块与非易损斑块组间各指标单因素比较分析采用两样本t检验(方差齐)。P<0.05为差异有统计学意义。 -
由表1可知,易损斑块组患者的年龄、体质指数、血糖、同型半胱氨酸、甘油三酯、低密度脂蛋白、载脂蛋白E、脂蛋白、胱抑素C、C反应蛋白、血沉、糖化血红蛋白c水平均明显高于非易损斑块组,且差异均有统计学意义(均P<0.05)。易损斑块组的MACCE、高血压、糖尿病、冠心病发生率均高于非易损斑块组,且差异均有统计学意义(均P<0.05);高密度脂蛋白、乳酸脱氢酶、肌酸激酶水平均明显低于非易损斑块组,且差异均有统计学意义(均P<0.05)。
基线资料 正常组
(n=203)稳定斑块组
(n=97)易损斑块组
(n=200)检验值 P值 年龄( $ \bar x \pm s$ 

54.0±10.3 60.8±9.5 61.9±10.3 F=60.212 <0.001 男性[例(%)] 89(43.8) 51(52.6) 105(52.5) χ2=3.638 0.162 MACCE [例(%)] 1(0.5) 50(51.5) 122(61.0) χ2=178.272 <0.001 体质指数( $ \bar x \pm s$ 

24.94±3.72 25.03±3.05 25.70±3.58 F=4.636 0.032 心率( $ \bar x \pm s$ 

76.08±12.66 80.36±43.31 74.61±13.84 F=0.422 0.516 高血压[例(%)] 61(30.0) 52(53.6) 116(58.0) χ2=34.662 <0.001 糖尿病[例(%)] 18(8.9) 17(17.5) 60(30.0) χ2=29.405 <0.001 高血脂[例(%)] 4(2.0) 7(7.2) 6(3.0) χ2=5.662 0.059 冠心病[例(%)] 9(4.4) 14(14.4) 34(17.0) χ2=16.847 <0.001 血糖( $ \bar x \pm s$ 

6.35±1.99 6.87±2.09 7.47±2.41 F=26.354 <0.001 同型半胱氨酸( $ \bar x \pm s$ 

11.77±3.97 13.45±4.17 14.14±4.15 F=33.891 <0.001 甘油三酯( $ \bar x \pm s$ 

1.91±0.79 2.34±0.91 2.47±0.99 F=40.249 <0.001 总胆固醇( $ \bar x \pm s$ 

4.43±0.87 4.34±1.21 4.32±1.05 F=0.807 0.370 高密度脂蛋白( $ \bar x \pm s$ 

1.18±0.28 1.12±0.25 1.04±0.23 F=18.273 <0.001 低密度脂蛋白( $ \bar x \pm s$ 

1.97±1.00 2.26±1.07 2.45±1.13 F=20.326 <0.001 载脂蛋白A1( $ \bar x \pm s$ 

1.50±0.31 1.34±0.25 1.40±0.22 F=1.697 0.195 载脂蛋白B( $ \bar x \pm s$ 

0.87±0.18 0.93±0.20 0.89±0.24 F=0.044 0.834 载脂蛋白E( $ \bar x \pm s$ 

56.81±18.49 61.89±17.42 64.72±19.68 F=17.924 <0.001 脂蛋白( $ \bar x \pm s$ 

244.34±65.25 255.06±67.36 261.96±71.08 F=6.777 0.010 胱抑素C( $ \bar x \pm s$ 

0.81±0.34 0.95±0.36 1.02±0.34 F=35.842 <0.001 C反应蛋白( $ \bar x \pm s$ 

2.00±1.13 11.89±4.67 13.20±5.26 F=678.519 <0.001 血沉( $ \bar x \pm s$ 

6.50±2.86 7.87±4.02 17.23±5.86 F=509.717 <0.001 糖化血红蛋白c( $ \bar x \pm s$ 

6.59±2.02 7.13±2.02 8.94±2.12 F=128.750 <0.001 乳酸脱氢酶( $ \bar x \pm s$ 

191.50±55.17 186.50±45.68 154.44±24.40 F=7.825 0.008 CK-MB[M(Q1,Q3),ng/ml] 2.00(0.95,5.40) 2.40(1.05,4.65) 0.90(0.60,1.45) H=3.545 0.170 肌酸激酶[M(Q1,Q3),U/L] 107.00(61.00,283.50) 85.50(61.25,160.00) 56.00(35.50,74.00) H=4.384 0.012 肌红蛋白[M(Q1,Q3),g/ml] 39.80(23.95,89.00) 64.85(34.60,126.00) 20.40(13.30,30.50) H=3.667 0.160 注:CT为计算机体层摄影术;MACCE 为主要心脑血管不良事件;CK-MB为肌酸激酶同工酶 表 1 同时行冠状动脉和头颈部动脉CT血管造影的500例有心脑血管疾病易患因素患者的基线资料
Table 1. Baseline data of 500 patients with cardiovascular and cerebrovascular disease susceptibility factors who received CT angiography of both coronary and head and neck arteries
-
由表2可知,易损斑块组患者的年龄、体质指数、血糖、同型半胱氨酸、甘油三酯、低密度脂蛋白、载脂蛋白E、脂蛋白、胱抑素C、C反应蛋白、血沉、糖化血红蛋白c水平均明显高于非易损斑块组,且差异均有统计学意义(均P<0.05)。易损斑块组的MACCE、高血压、糖尿病、冠心病发生率均高于非易损斑块组,且差异均有统计学意义(均P<0.05);易损斑块组的高密度脂蛋白、乳酸脱氢酶、肌酸激酶水平均明显低于非易损斑块组,且差异均有统计学意义(均P<0.05)。
变量 非易损斑块组
(n=300)易损斑块组
(n=200)检验值 P值 年龄( $ \bar x \pm s$ 

56.2±10.5 61.9±10.3 t=5.989 <0.001 男性[例(%)] 140(46.7) 105(52.5) χ2=1.634 0.201 MACCE[例(%)] 51(17.0) 122(61.0) χ2=102.667 <0.001 体质指数( $ \bar x \pm s$ 

24.97±3.51 25.70±3.58 t=2.267 0.024 心率( $ \bar x \pm s$ 

77.45±26.66 74.61±13.84 t=1.389 0.166 高血压[例(%)] 113(37.7) 116(58.0) χ2=19.986 <0.001 糖尿病[例(%)] 35(11.7) 60(30.0) χ2=26.207 <0.001 高血脂[例(%)] 11(3.7) 6(3.0) χ2=0.162 0.687 冠心病[例(%)] 23(7.7) 34(17.0) χ2=10.349 <0.001 血糖( $ \bar x \pm s$ 

6.52±2.03 7.47±2.41 t=4.738 <0.001 同型半胱氨酸( $ \bar x \pm s$ 

12.32±4.11 14.14±4.15 t=4.848 <0.001 甘油三酯( $ \bar x \pm s$ 

2.05±0.85 2.47±0.99 t=5.148 <0.001 总胆固醇( $ \bar x \pm s$ 

4.41±0.98 4.32±1.05 t=0.772 0.441 高密度脂蛋白( $ \bar x \pm s$ 

1.16±0.27 1.04±0.23 t=4.062 <0.001 低密度脂蛋白( $ \bar x \pm s$ 

2.06±1.03 2.45±1.13 t=3.922 <0.001 载脂蛋白A1( $ \bar x \pm s$ 

1.42±0.29 1.40±0.22 t=0.443 0.659 载脂蛋白B( $ \bar x \pm s$ 

0.90±0.19 0.89±0.24 t=0.210 0.835 载脂蛋白E( $ \bar x \pm s$ 

58.45±18.28 64.72±19.68 t=3.643 <0.001 脂蛋白( $ \bar x \pm s$ 

247.81±66.02 261.96±71.08 t=2.278 0.023 胱抑素C( $ \bar x \pm s$ 

0.86±0.35 1.02±0.34 t=5.016 <0.001 C反应蛋白( $ \bar x \pm s$ 

5.20±1.41 13.20±5.26 t=16.376 <0.001 血沉( $ \bar x \pm s$ 

6.94±3.34 17.23±5.86 t=24.930 <0.001 糖化血红蛋白c( $ \bar x \pm s$ 

6.77±2.03 8.94±2.12 t=11.498 <0.001 乳酸脱氢酶( $ \bar x \pm s$ 

188.64±47.97 154.44±24.40 t=2.965 0.005 CK-MB[M(Q1,Q3),ng/ml] 2.00(1.10,5.40) 0.90(0.60,1.45) Z=1.883 0.060 肌酸激酶[M(Q1,Q3),U/L] 88.00(61.00,173.50) 56.00(35.50,74.00) Z=−2.065 0.039 肌红蛋白[M(Q1,Q3),g/ml] 54.10(30.05,96.95) 20.40(13.30,30.50) Z=−1.742 0.082 注:MACCE 为主要心脑血管不良事件;CK-MB为肌酸激酶同工酶 表 2 2组有心脑血管疾病易患因素患者间各指标的单因素分析
Table 2. Univariate analysis of each index between two groups of patients with cardiovascular and cerebrovascular disease susceptibility factors
-
以是否为易损斑块为因变量、上述单因素分析有统计学意义的变量为自变量,多因素Logistic回归分析结果见表3。年龄、高血压、糖尿病、高血糖、同型半胱氨酸、C反应蛋白这6个指标为易损斑块的危险因素。
因素 B S.E Wald P值 OR 95%CI 下限 上限 年龄 0.027 0.012 5.085 0.024 1.027 1.004 1.052 糖尿病 0.911 0.304 8.974 0.003 2.488 1.370 4.517 高血糖 0.204 0.055 13.585 <0.001 1.227 1.100 1.368 C反应蛋白 0.699 0.345 4.091 0.043 2.011 1.022 3.958 高血压 0.503 0.244 4.259 0.039 1.654 1.026 2.667 同型半胱氨酸 0.075 0.029 6.978 0.008 1.078 1.020 1.140 脂蛋白 0.003 0.002 2.895 0.089 1.003 1.000 1.007 注:B为回归系数;S.E为回归系数的标准误;Wald为回归系数的Wald χ2检验;OR为优势比;CI为置信区间 表 3 有心脑血管疾病易患因素患者易损斑块发生的多因素Logistic回归分析
Table 3. Multivariate Logistic regression analysis of vulnerable plaque in patients with cardiovascular and cerebrovascular disease susceptibility factors
-
与非易损斑块组患者相比,易损斑块组患者发生MACCE的时间更早[(1.1±0.3)年对(0.8±0.2)年],患者年龄更小[(59.9±13.7)岁对(54.1±8.5)岁],且差异均有统计学意义(t=7.775,P<0.001;t=2.059,P=0.043)。
通过对易损斑块组患者分析发现,发生MACCE的患者有122例,未发生MACCE的患者有78例。发生MACCE的患者多合并多个易损斑块征象,发生与未发生MACCE患者的易损斑块征象情况比较详见表4。
组别 低CT衰减 血管正性重构指数 点状钙化 “餐巾环”征 无 有 无 有 无 有 无 有 发生MACCE的患者(n=122) 22(18.0) 100(82.0) 39(32.0) 83(68.0) 72(59.0) 50(41.0) 42(34.4) 80(65.6) 未发生MACCE的患者(n=78) 64(82.1) 14(17.9) 55(70.5) 23(29.5) 56(71.8) 22(28.2) 54(69.2) 24(30.8) χ2值 4.057 2.789 4.665 3.274 P值 0.025 0.033 0.021 0.044 注:MACCE为主要心脑血管不良事件;CT为计算机体层摄影术 表 4 发生与未发生MACCE患者的易损斑块征象情况比较[例(%)]
Table 4. Comparison of vulnerable plaque signs between patients with and without major adverse cardiovascular and cerebrovascular events (case (%))
-
由表5可知,有易损斑块的患者发生MACCE的概率是无易损斑块患者的7.637倍。
因素 B S.E. Wald P值 OR 95%CI 下限 上限 易损斑块 2.033 0.211 92.579 <0.001 7.637 5.047 11.554 注:MACCE为主要心脑血管不良事件;B为回归系数;S.E为回归系数的标准误;Wald为回归系数的Wald χ2检验;OR为优势比;CI为置信区间 表 5 有心脑血管疾病易患因素患者的易损斑块与MACCE的多因素Logistic分析
Table 5. Multivariate Logistic analysis of vulnerable plaques and major adverse cardiovascular and cerebrovascular events in patients with cardiovascular and cerebrovascular disease susceptibility factors
-
易损斑块组发生MACCE的122例患者中,发生心血管不良事件的有85例,发生脑血管意外的有37例(表6)。发生心血管不良事件的85例患者中稳定性心绞痛(stable angina pectoris,SAP)患者47例、急性冠状动脉综合征(acute coronary syndrome,ACS)患者38例。由表7可知,点状钙化斑块在ACS患者中出现的更频繁,大钙化斑块在SAP患者中更常见。另外,ACS患者斑块的平均最低密度CT值低于SAP患者,且差异有统计学意义(P<0.05)。
组别 正常 稳定性心绞痛 恶性心律失常 心梗 支架或搭桥 心源性猝死 脑血管意外 非易损斑块组(n=300) 249(83.0) 23(7.7) 3(1.0) 6(2.0) 7(2.3) 0(0.0) 12(4.0) 易损斑块组(n=200) 78(39.0) 47(23.5) 8(4.0) 8(4.0) 20(10.0) 2(1.0) 37(18.5) 合计 327(65.4) 70(14.0) 11(2.2) 14(2.8) 27(5.4) 2(0.4) 49(9.8) 注:MACCE为主要心脑血管不良事件 表 6 2组有心脑血管疾病易患因素患者发生MACCE的类别统计[例(%)]
Table 6. Category statistics of major adverse cardiovascular and cerebrovascular events in two groups of patients with cardiovascular and cerebrovascular disease susceptibility factors (case (%))
组别 点状钙化斑块
(%)大钙化斑块
(%)CT值( $ \bar x \pm s$ 

斑块负荷( $ \bar x \pm s $ 

有 无 有 无 ACS患者(n=38) 19(50.0) 19(50.0) 7(18.4) 31(81.6) 78±39 100.6±43.3 SAP患者(n=47) 8(17.0) 39(83.0) 18(38.3) 29(61.7) 114±55 90.3±42.6 χ2值 10.543 3.999 2.330 0.519 P值 0.002 0.046 0.025 0.084 注:ACS为急性冠状动脉综合征;SAP为稳定性心绞痛 表 7 2组发生心血管不良事件患者的斑块成分及钙化形态特征的比较
Table 7. Comparison of plaque composition and morphological characteristics of calcification between two groups of patients with cardiovascular adverse events
-
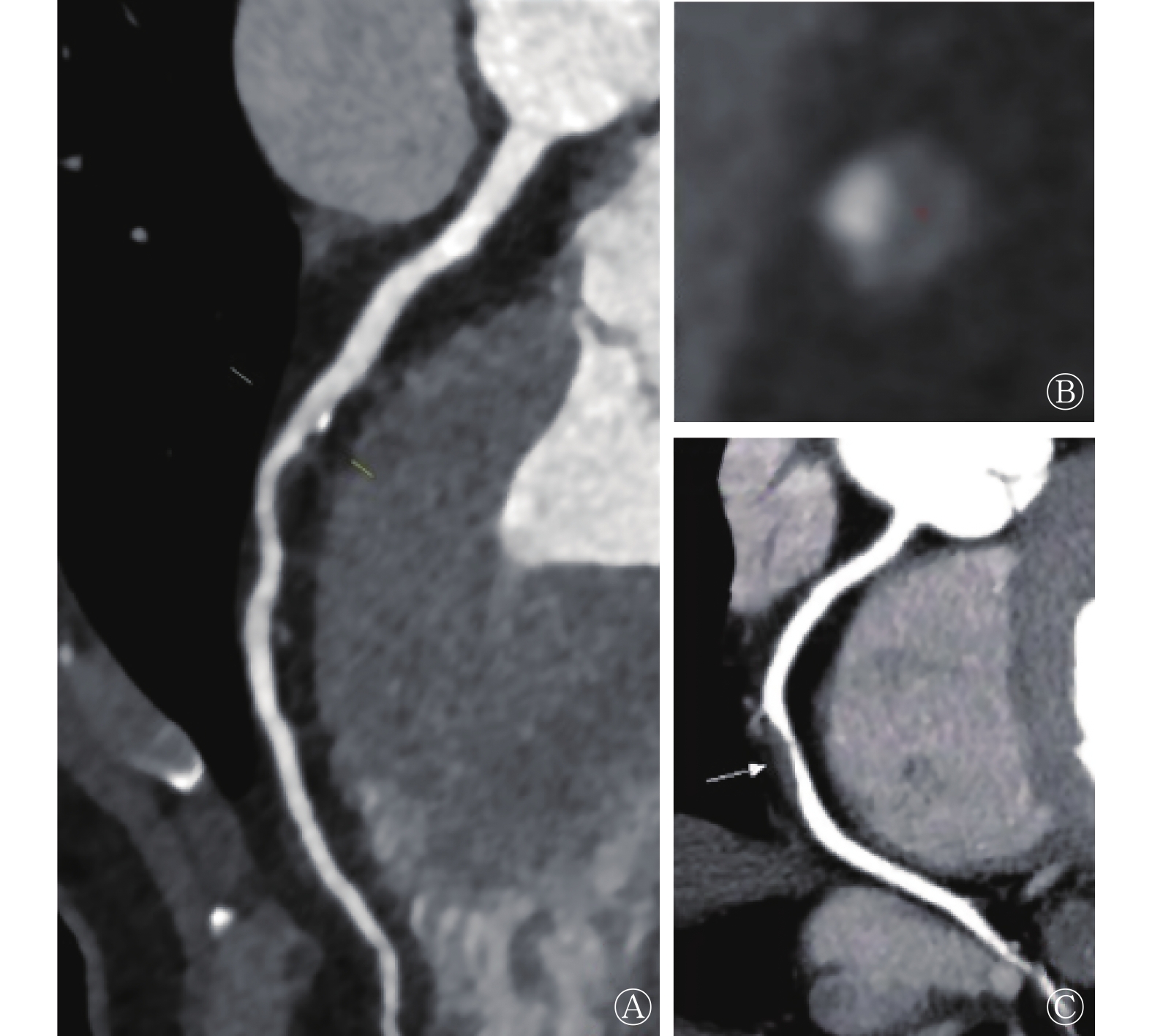
易损斑块的CTA特征主要表现为低CT衰减、血管正性重构指数、点状钙化、“餐巾环”征。典型CT特征图见图1~2,典型病例图见图3~5。

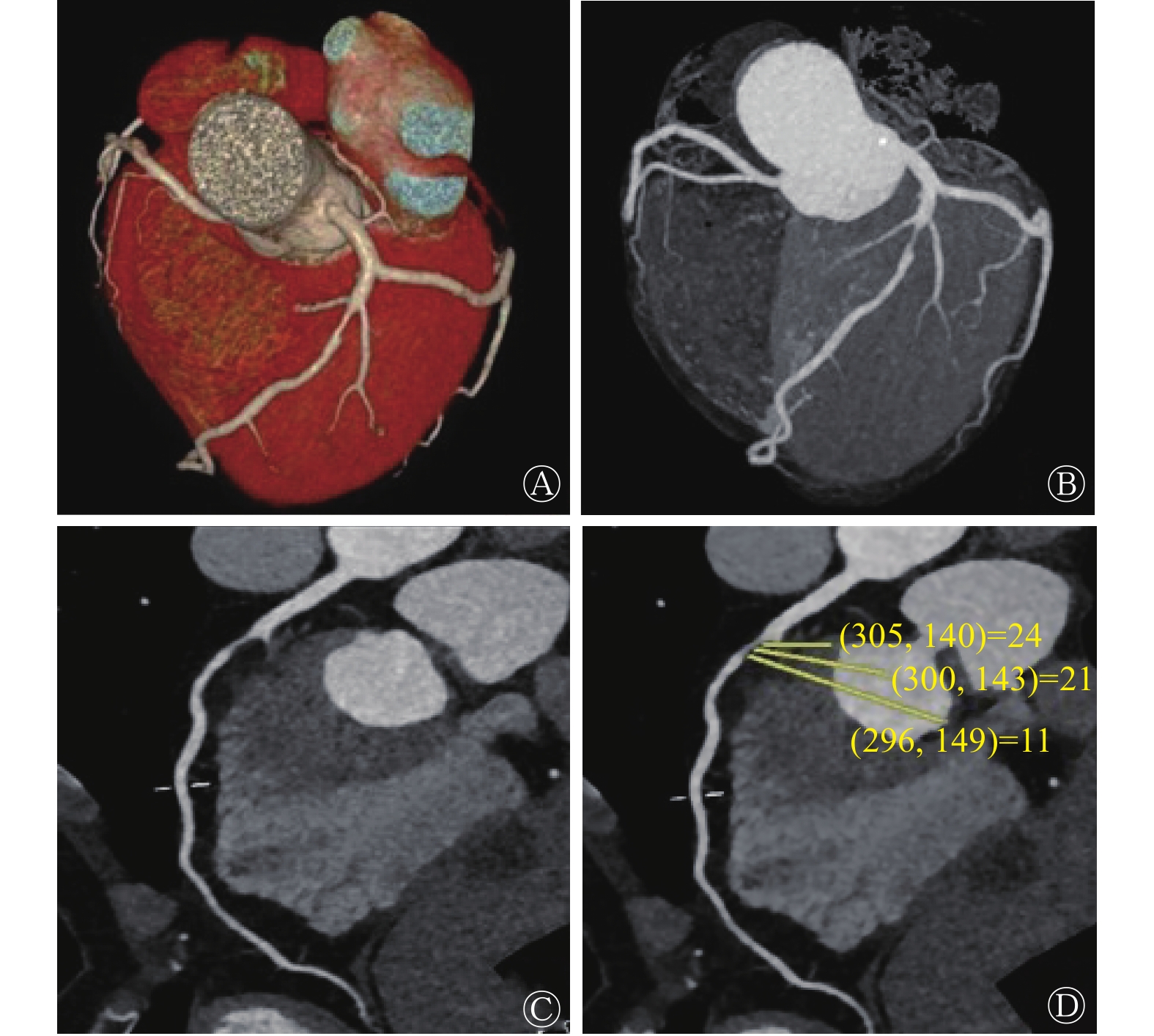
图 1 有心脑血管疾病易患因素患者的冠状动脉容积再现图(A)、冠状动脉重建最大密度投影图(B)与前降支曲面重建图(C、D)
Figure 1. Coronary artery volume reconstruction (A), maximum intensity projection of coronary artery reconstruction (B) and curved planar reformation of anterior descending branch (C and D) of a patient with cardiovascular and cerebrovascular disease susceptibility factors

图 2 有心脑血管疾病易患因素患者的冠状动脉曲面重建图
Figure 2. Curved planar reformation of coronary artery surface of a patient with cardiovascular and cerebrovascular disease susceptibility factors

图 3 有心脑血管疾病易患因素患者的心脑血管容积再现图(A)、冠状动脉容积再现图(B)及冠状动脉重建最大密度投影图(C)
Figure 3. Cardio-cerebrovascular volume reconstruction (A), coronary artery volume reconstruction (B), and maximum intensity projection of coronary artery reconstruction (C) of a patient with cardiovascular and cerebrovascular disease susceptibility factors

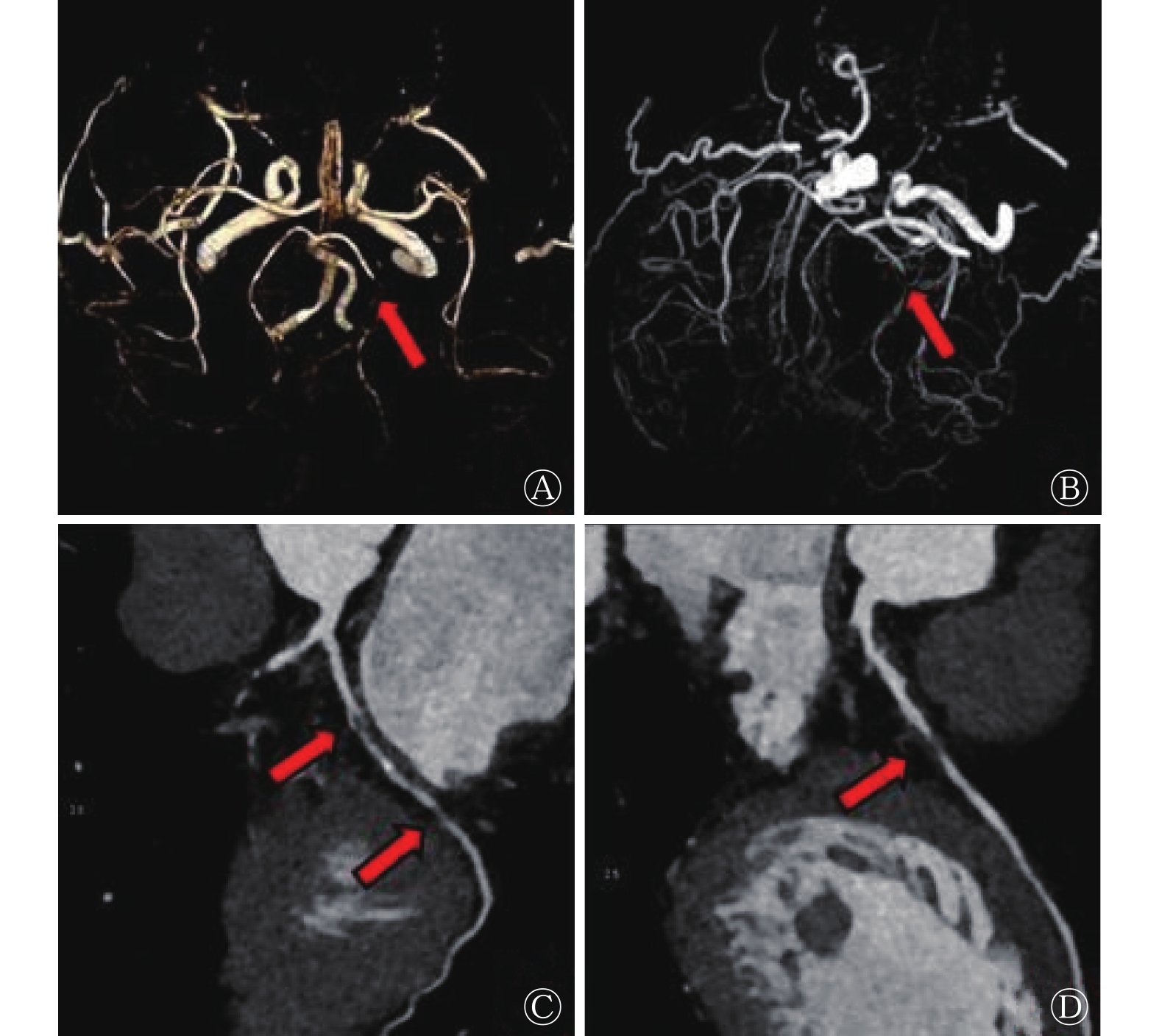
图 4 有心脑血管疾病易患因素患者的脑血管容积再现图(后面观)(A)、脑血管重建最大密度投影图(后面观)(B)、左冠状动脉回旋支曲面重建图(C)及左冠状动脉前降支曲面重建图(D)
Figure 4. Head vascular volume reconstruction (back view) (A), maximum intensity projection of head vascular reconstruction (back view) (B), curved planar reformation of left coronary artery circumflex branch (C) and curved planar reformation of the anterior descending branch of the left coronary artery (D) of a patient with cardiovascular and cerebrovascular disease susceptibility factors

图 5 有心脑血管疾病易患因素患者左冠状动脉支架置入术前(A、B、D)和术后(C)的冠状动脉造影图
Figure 5. Coronary angiography images of a patient with cardiovascular and cerebrovascular disease susceptibility factors before (A, B, D) and after (C) left coronary artery stent implantation
-
与有创性的冠状动脉造影检查相比,CTA最大的实际应用价值就是能显示各种类型的斑块,并且能对斑块进行定量或半定量分析。从斑块性质方面看,我们发现心脑血管中存在易损斑块及混合斑块的患者发生MACCE的风险明显高于钙化斑块患者。运用第三代双源低剂量CT大螺距扫描模式实施心脑血管一体化成像,对心脑血管动脉易损斑块具有良好的诊断价值,同时也是无创的、对MACCE有预警价值的危险分层工具。通过了解心脑血管动脉易损斑块的危险因素,可知易损斑块阳性对于MACCE的发生具有良好的预测价值,有助于指导临床医师采取有效干预措施。
相关研究结果表明,CT对评估斑块易损性有重要意义[9, 11]。也有研究结果表明,MACCE患者责任病灶的斑块面积及重构指数均远高于正常健康人群;就钙化形态而言,ACS患者常表现为非钙化或伴细小斑点状钙化的斑块[12-13]。本研究对比分析了易损和非易损斑块患者随访过程中MACCE的发生率,结果表明前者的发生率更高。此外,与未发生MACCE的患者相比,发生MACCE的患者的低CT衰减、血管正性重构指数等相关指标都明显升高,且差异均有统计学意义,据此也可以判断在进行MACCE预测分析方面,点状钙化、低CT衰减、“餐巾环”征等相关指标具有一定的预测价值。
本研究结果显示,年龄、糖尿病、高血糖、C反应蛋白、高血压、同型半胱氨酸这6个指标为易损斑块发生的危险因素。本研究结果还表明,ACS患者斑块最低平均密度CT值为(78±39) HU,SAP患者为(114±55) HU。而一些学者选择了斑块CT值<50 HU来判断易损斑块,不过在阈值较低的情况下,该标准识别易损斑块的特异性可能受到影响[14]。点状钙化预测值诊断ACS的灵敏度一般不超过60%,最低密度CT值<35 HU诊断ACS的灵敏度可达到89% ,而相应的阴性预测值高于90%,而在此预测过程中,同时存在此两项特征时,阳性预测值可达到96%,遇到此种情况可判断斑块的易损性较高[14]。点状钙化与易损斑块同时存在时,易脱落导致血管栓塞,进而导致MACCE及心电生理紊乱。
由于本研究为单中心研究,存在诸多局限与不足,应进一步深入研究脂蛋白磷脂酶A2、基质金属蛋白酶及干扰素等炎症因子和相关基因序列对心脑血管动脉易损斑块危险因素的影响。同时,本研究的随访绝大多数是通过电话完成的,不可避免患者或患者家属存在统计学回忆偏倚,但我们在随访中应用了各种方法,例如联系主管医师及翻阅病历等,尽可能保证全面收集相关信息,综合进行分析,在一定程度上减少了回忆偏倚。本研究仅对易损斑块的特征进行了统计,未充分统计CT中的其他参数,尤其是对第三代双源CT的数据与诊断预测价值未做进一步分析,这也是我们后续研究分析的方向。
利益冲突 所有作者声明无利益冲突
作者贡献声明 王蓉负责现场试验、数据的采集、论文的撰写;籍庆余负责数据的采集与分析;杜娇负责病例的筛选、数据的整理;刘晓林负责数据的分析与整理;穆耀强、李林涛、张永春负责临床随访、论文的审阅;孙凯负责研究的设计、论文的审阅
第三代双源低剂量CT心脑血管一体化成像评价斑块易损性及其早期预警价值的研究
Evaluation of plaque vulnerability and early warning value of the third-generation dual-source low-dose CT integrative cardio-cerebrovascular imaging
-
摘要:
目的 使用第三代双源低剂量CT心脑血管一体化成像[即同时行冠状动脉和头颈部动脉CT血管造影(CTA)]对有心脑血管危险因素的高危人群进行筛查,通过分析易损斑块发生的危险因素,为临床提供心脑血管疾病的早期预警。 方法 前瞻性选择包头市中心医院2016年1月至2019年1月临床上需要同时进行冠状动脉和头颈部动脉CTA的患者,连续纳入614例。根据纳入排除标准,最终选择500例患者,其中,男性245例、女性255例,年龄(57.8±14.2)岁。根据CTA特征,将500例患者分为易损斑块组200例、稳定斑块组97例和正常组203例,其中稳定斑块组和正常组合称为非易损斑块组。通过对易损斑块患者发生的主要心脑血管不良事件(MACCE)进行随访,构建多因素Logistic模型对易损斑块发生的危险因素进行分析,评价斑块易损性。计数资料组间比较采用卡方检验;符合正态分布的计量资料的多组间比较采用方差分析;呈偏态分布的计量资料的两组间比较采用非参数U检验,多组间比较采用非参数Kruskal-Wallis检验。采用多因素Logistic回归分析,分析易损斑块与危险因素、MACCE的相关性。易损斑块和非易损斑块组间各指标单因素比较分析采用两样本t检验。 结果 (1)易损斑块组患者的年龄、体质指数、血糖、同型半胱氨酸、甘油三酯、低密度脂蛋白、载脂蛋白E、脂蛋白、胱抑素C、C反应蛋白、血沉、糖化血红蛋白c水平均明显高于非易损斑块组,且差异均有统计学意义(t=2.267~24.930,均P<0.05)。易损斑块组的MACCE、高血压、糖尿病、冠心病发生率均高于非易损斑块组,且差异均有统计学意义(χ2=10.349~102.667,均P<0.05);易损斑块组的高密度脂蛋白、乳酸脱氢酶、肌酸激酶水平均明显低于非易损斑块组,且差异均有统计学意义(t=4.062、2.965,Z=−2.065,均P<0.05)。(2)年龄(OR=1.027,95%CI:1.004~1.052)、高血压(OR=1.654,95%CI:1.026~2.667)、糖尿病(OR=2.488,95%CI:1.370~4.517)、高血糖(OR=1.227,95%CI:1.100~1.368)、同型半胱氨酸(OR=1.078,95%CI:1.020~1.140)、C反应蛋白(OR=2.011,95%CI:1.022~3.958)这6个指标为易损斑块发生的危险因素。(3)与非易损斑块组患者相比,易损斑块组患者发生MACCE的时间更早[(1.1±0.3)年对(0.8±0.2)年],患者年龄更小[(59.9±13.7)岁对(54.1±8.5)岁],且差异均有统计学意义(t=7.775,P<0.001;t=2.059,P=0.043)。(4)发生MACCE的患者多合并多个易损斑块征象。(5)有易损斑块的患者发生MACCE的概率是无易损斑块患者的7.637倍,易损斑块是MACCE事件的独立危险因素(OR=7.637,95%CI:5.047~11.554)。 结论 使用第三代双源低剂量CT心脑血管一体化成像评估心脑血管动脉易损斑块对心脑血管疾病早期预警具有重要价值。 -
关键词:
- 计算机体层摄影血管造影术 /
- 危险因素 /
- 心血管疾病 /
- 脑血管障碍 /
- 易损斑块
Abstract:Objective To screen the high-risk population with cardiovascular and cerebrovascular risk factors using third-generation dual-source low-dose computed tomography (CT) integrative cardio-cerebrovascular imaging (i.e., simultaneous coronary artery and head and neck artery computed tomography angiography (CTA)), and to provide early warning of cardiovascular and cerebrovascular diseases by analyzing the risk factors for the occurrence of vulnerable plaques. Methods Patients requiring simultaneous coronary artery and head and neck artery CTA were prospectively selected from the Baotou Central Hospital from January 2016 to January 2019, and 614 cases were consecutively included. According to the inclusion and exclusion criteria, 500 patients were selected, including 245 males and 255 females. The age was (57.8±14.2) years. Based on CTA characteristics, the 500 patients were divided into the vulnerable plaque group (200 cases), the stable plaque group (97 cases), and the normal plaque group (203 cases). The stable plaque group and the normal plaque group were called the non-vulnerable plaque group. Through the follow-up of major cardiovascular and cerebrovascular adverse events (MACCE) in patients with vulnerable plaque, the multivariate logistic model was constructed to analyze the vulnerable plaque risk factors and evaluate the plaque block vulnerability. Chi-square test was used to compare the counting data groups. Analysis of variance was used to compare the measurement data with normal distribution between multiple groups. The comparison between two groups of econometric data with skewed distribution used a non parametric U-test, while the comparison between multiple groups used a non parametric Kruskal-Wallis test. Multivariate Logistic regression analysis was used to examine the correlation between vulnerable plaques, risk factors, and MACCE. Two-sample t test was used for the single-factor comparative analysis of indicators between the vulnerable plaque group and the non-vulnerable plaque group. Results (1) The levels of age, body mass index, blood glucose, homocysteine, triglyceride, low-density lipoprotein, apolipoprotein E, lipoprotein, cystatin C, C-reactive protein, erythrocyte sedimentation rate, and glycosylated hemoglobin c in the vulnerable plaque group were significantly higher than those in the non-vulnerable plaque group, and the differences were statistically significant (t=2.267−24.930, all P<0.05). The incidence of MACCE, hypertension, diabetes, coronary heart disease in the vulnerable plaque group were higher than those in the non-vulnerable plaque group, and the differences were statistically significant (χ2=10.349−102.667, all P<0.05). High-density lipoprotein, lactate dehydrogenase, and the level of creatine kinase were significantly lower in the vulnerable plaque group than those in the non-vulnerable plaque group, and the differences were statistically significant (t=4.062, 2.965, Z=−2.065; all P<0.05). (2) Age (OR=1.027, 95%CI: 1.004–1.052), hypertension (OR=1.654, 95%CI: 1.026–2.667), glycosuria (OR=2.488, 95%CI: 1.370–4.517), hyperglycemia (OR=1.227, 95%CI: 1.100–1.368), homocysteine (OR=1.078, 95%CI: 1.020–1.140), and C-reactive protein (OR=2.011, 95%CI: 1.022–3.958) were risk factors for vulnerable plaques. (3) Compared with the non-vulnerable plaque group, the onset of MACCE in the vulnerable plaque group was earlier ((1.1±0.3) years vs. (0.8±0.2) years), and the patients were younger ((59.9±13.7) years vs. (54.1±8.5) years). All the differences were statistically significant (t=7.775, P<0.001; t=2.059, P=0.043). (4) More patients with MACCE had multiple signs of vulnerable plaques. (5) The probability of MACCE in patients with vulnerable plaque was 7.637 times higher than that in patients without vulnerable plaque. Vulnerable plaque was an independent risk factor for MACCE (OR=7.637, 95%CI: 5.047–11.554). Conclusion The third-generation dual-source low-dose CT integrated cardio-cerebrovascular imaging is of great value for the early warning of cardiovascular and cerebrovascular diseases. -
图 1 有心脑血管疾病易患因素患者的冠状动脉容积再现图(A)、冠状动脉重建最大密度投影图(B)与前降支曲面重建图(C、D)
Figure 1. Coronary artery volume reconstruction (A), maximum intensity projection of coronary artery reconstruction (B) and curved planar reformation of anterior descending branch (C and D) of a patient with cardiovascular and cerebrovascular disease susceptibility factors
图 2 有心脑血管疾病易患因素患者的冠状动脉曲面重建图
Figure 2. Curved planar reformation of coronary artery surface of a patient with cardiovascular and cerebrovascular disease susceptibility factors
图 3 有心脑血管疾病易患因素患者的心脑血管容积再现图(A)、冠状动脉容积再现图(B)及冠状动脉重建最大密度投影图(C)
Figure 3. Cardio-cerebrovascular volume reconstruction (A), coronary artery volume reconstruction (B), and maximum intensity projection of coronary artery reconstruction (C) of a patient with cardiovascular and cerebrovascular disease susceptibility factors
图 4 有心脑血管疾病易患因素患者的脑血管容积再现图(后面观)(A)、脑血管重建最大密度投影图(后面观)(B)、左冠状动脉回旋支曲面重建图(C)及左冠状动脉前降支曲面重建图(D)
Figure 4. Head vascular volume reconstruction (back view) (A), maximum intensity projection of head vascular reconstruction (back view) (B), curved planar reformation of left coronary artery circumflex branch (C) and curved planar reformation of the anterior descending branch of the left coronary artery (D) of a patient with cardiovascular and cerebrovascular disease susceptibility factors
图 5 有心脑血管疾病易患因素患者左冠状动脉支架置入术前(A、B、D)和术后(C)的冠状动脉造影图
Figure 5. Coronary angiography images of a patient with cardiovascular and cerebrovascular disease susceptibility factors before (A, B, D) and after (C) left coronary artery stent implantation
表 1 同时行冠状动脉和头颈部动脉CT血管造影的500例有心脑血管疾病易患因素患者的基线资料
Table 1. Baseline data of 500 patients with cardiovascular and cerebrovascular disease susceptibility factors who received CT angiography of both coronary and head and neck arteries
基线资料 正常组
(n=203)稳定斑块组
(n=97)易损斑块组
(n=200)检验值 P值 年龄( $ \bar x \pm s$ 54.0±10.3 60.8±9.5 61.9±10.3 F=60.212 <0.001 男性[例(%)] 89(43.8) 51(52.6) 105(52.5) χ2=3.638 0.162 MACCE [例(%)] 1(0.5) 50(51.5) 122(61.0) χ2=178.272 <0.001 体质指数( $ \bar x \pm s$ 24.94±3.72 25.03±3.05 25.70±3.58 F=4.636 0.032 心率( $ \bar x \pm s$ 76.08±12.66 80.36±43.31 74.61±13.84 F=0.422 0.516 高血压[例(%)] 61(30.0) 52(53.6) 116(58.0) χ2=34.662 <0.001 糖尿病[例(%)] 18(8.9) 17(17.5) 60(30.0) χ2=29.405 <0.001 高血脂[例(%)] 4(2.0) 7(7.2) 6(3.0) χ2=5.662 0.059 冠心病[例(%)] 9(4.4) 14(14.4) 34(17.0) χ2=16.847 <0.001 血糖( $ \bar x \pm s$ 6.35±1.99 6.87±2.09 7.47±2.41 F=26.354 <0.001 同型半胱氨酸( $ \bar x \pm s$ 11.77±3.97 13.45±4.17 14.14±4.15 F=33.891 <0.001 甘油三酯( $ \bar x \pm s$ 1.91±0.79 2.34±0.91 2.47±0.99 F=40.249 <0.001 总胆固醇( $ \bar x \pm s$ 4.43±0.87 4.34±1.21 4.32±1.05 F=0.807 0.370 高密度脂蛋白( $ \bar x \pm s$ 1.18±0.28 1.12±0.25 1.04±0.23 F=18.273 <0.001 低密度脂蛋白( $ \bar x \pm s$ 1.97±1.00 2.26±1.07 2.45±1.13 F=20.326 <0.001 载脂蛋白A1( $ \bar x \pm s$ 1.50±0.31 1.34±0.25 1.40±0.22 F=1.697 0.195 载脂蛋白B( $ \bar x \pm s$ 0.87±0.18 0.93±0.20 0.89±0.24 F=0.044 0.834 载脂蛋白E( $ \bar x \pm s$ 56.81±18.49 61.89±17.42 64.72±19.68 F=17.924 <0.001 脂蛋白( $ \bar x \pm s$ 244.34±65.25 255.06±67.36 261.96±71.08 F=6.777 0.010 胱抑素C( $ \bar x \pm s$ 0.81±0.34 0.95±0.36 1.02±0.34 F=35.842 <0.001 C反应蛋白( $ \bar x \pm s$ 2.00±1.13 11.89±4.67 13.20±5.26 F=678.519 <0.001 血沉( $ \bar x \pm s$ 6.50±2.86 7.87±4.02 17.23±5.86 F=509.717 <0.001 糖化血红蛋白c( $ \bar x \pm s$ 6.59±2.02 7.13±2.02 8.94±2.12 F=128.750 <0.001 乳酸脱氢酶( $ \bar x \pm s$ 191.50±55.17 186.50±45.68 154.44±24.40 F=7.825 0.008 CK-MB[M(Q1,Q3),ng/ml] 2.00(0.95,5.40) 2.40(1.05,4.65) 0.90(0.60,1.45) H=3.545 0.170 肌酸激酶[M(Q1,Q3),U/L] 107.00(61.00,283.50) 85.50(61.25,160.00) 56.00(35.50,74.00) H=4.384 0.012 肌红蛋白[M(Q1,Q3),g/ml] 39.80(23.95,89.00) 64.85(34.60,126.00) 20.40(13.30,30.50) H=3.667 0.160 注:CT为计算机体层摄影术;MACCE 为主要心脑血管不良事件;CK-MB为肌酸激酶同工酶  下载: 导出CSV
下载: 导出CSV
表 2 2组有心脑血管疾病易患因素患者间各指标的单因素分析
Table 2. Univariate analysis of each index between two groups of patients with cardiovascular and cerebrovascular disease susceptibility factors
变量 非易损斑块组
(n=300)易损斑块组
(n=200)检验值 P值 年龄( $ \bar x \pm s$ 56.2±10.5 61.9±10.3 t=5.989 <0.001 男性[例(%)] 140(46.7) 105(52.5) χ2=1.634 0.201 MACCE[例(%)] 51(17.0) 122(61.0) χ2=102.667 <0.001 体质指数( $ \bar x \pm s$ 24.97±3.51 25.70±3.58 t=2.267 0.024 心率( $ \bar x \pm s$ 77.45±26.66 74.61±13.84 t=1.389 0.166 高血压[例(%)] 113(37.7) 116(58.0) χ2=19.986 <0.001 糖尿病[例(%)] 35(11.7) 60(30.0) χ2=26.207 <0.001 高血脂[例(%)] 11(3.7) 6(3.0) χ2=0.162 0.687 冠心病[例(%)] 23(7.7) 34(17.0) χ2=10.349 <0.001 血糖( $ \bar x \pm s$ 6.52±2.03 7.47±2.41 t=4.738 <0.001 同型半胱氨酸( $ \bar x \pm s$ 12.32±4.11 14.14±4.15 t=4.848 <0.001 甘油三酯( $ \bar x \pm s$ 2.05±0.85 2.47±0.99 t=5.148 <0.001 总胆固醇( $ \bar x \pm s$ 4.41±0.98 4.32±1.05 t=0.772 0.441 高密度脂蛋白( $ \bar x \pm s$ 1.16±0.27 1.04±0.23 t=4.062 <0.001 低密度脂蛋白( $ \bar x \pm s$ 2.06±1.03 2.45±1.13 t=3.922 <0.001 载脂蛋白A1( $ \bar x \pm s$ 1.42±0.29 1.40±0.22 t=0.443 0.659 载脂蛋白B( $ \bar x \pm s$ 0.90±0.19 0.89±0.24 t=0.210 0.835 载脂蛋白E( $ \bar x \pm s$ 58.45±18.28 64.72±19.68 t=3.643 <0.001 脂蛋白( $ \bar x \pm s$ 247.81±66.02 261.96±71.08 t=2.278 0.023 胱抑素C( $ \bar x \pm s$ 0.86±0.35 1.02±0.34 t=5.016 <0.001 C反应蛋白( $ \bar x \pm s$ 5.20±1.41 13.20±5.26 t=16.376 <0.001 血沉( $ \bar x \pm s$ 6.94±3.34 17.23±5.86 t=24.930 <0.001 糖化血红蛋白c( $ \bar x \pm s$ 6.77±2.03 8.94±2.12 t=11.498 <0.001 乳酸脱氢酶( $ \bar x \pm s$ 188.64±47.97 154.44±24.40 t=2.965 0.005 CK-MB[M(Q1,Q3),ng/ml] 2.00(1.10,5.40) 0.90(0.60,1.45) Z=1.883 0.060 肌酸激酶[M(Q1,Q3),U/L] 88.00(61.00,173.50) 56.00(35.50,74.00) Z=−2.065 0.039 肌红蛋白[M(Q1,Q3),g/ml] 54.10(30.05,96.95) 20.40(13.30,30.50) Z=−1.742 0.082 注:MACCE 为主要心脑血管不良事件;CK-MB为肌酸激酶同工酶
下载: 导出CSV
表 3 有心脑血管疾病易患因素患者易损斑块发生的多因素Logistic回归分析
Table 3. Multivariate Logistic regression analysis of vulnerable plaque in patients with cardiovascular and cerebrovascular disease susceptibility factors
因素 B S.E Wald P值 OR 95%CI 下限 上限 年龄 0.027 0.012 5.085 0.024 1.027 1.004 1.052 糖尿病 0.911 0.304 8.974 0.003 2.488 1.370 4.517 高血糖 0.204 0.055 13.585 <0.001 1.227 1.100 1.368 C反应蛋白 0.699 0.345 4.091 0.043 2.011 1.022 3.958 高血压 0.503 0.244 4.259 0.039 1.654 1.026 2.667 同型半胱氨酸 0.075 0.029 6.978 0.008 1.078 1.020 1.140 脂蛋白 0.003 0.002 2.895 0.089 1.003 1.000 1.007 注:B为回归系数;S.E为回归系数的标准误;Wald为回归系数的Wald χ2检验;OR为优势比;CI为置信区间
下载: 导出CSV
表 4 发生与未发生MACCE患者的易损斑块征象情况比较[例(%)]
Table 4. Comparison of vulnerable plaque signs between patients with and without major adverse cardiovascular and cerebrovascular events (case (%))
组别 低CT衰减 血管正性重构指数 点状钙化 “餐巾环”征 无 有 无 有 无 有 无 有 发生MACCE的患者(n=122) 22(18.0) 100(82.0) 39(32.0) 83(68.0) 72(59.0) 50(41.0) 42(34.4) 80(65.6) 未发生MACCE的患者(n=78) 64(82.1) 14(17.9) 55(70.5) 23(29.5) 56(71.8) 22(28.2) 54(69.2) 24(30.8) χ2值 4.057 2.789 4.665 3.274 P值 0.025 0.033 0.021 0.044 注:MACCE为主要心脑血管不良事件;CT为计算机体层摄影术
下载: 导出CSV
表 5 有心脑血管疾病易患因素患者的易损斑块与MACCE的多因素Logistic分析
Table 5. Multivariate Logistic analysis of vulnerable plaques and major adverse cardiovascular and cerebrovascular events in patients with cardiovascular and cerebrovascular disease susceptibility factors
因素 B S.E. Wald P值 OR 95%CI 下限 上限 易损斑块 2.033 0.211 92.579 <0.001 7.637 5.047 11.554 注:MACCE为主要心脑血管不良事件;B为回归系数;S.E为回归系数的标准误;Wald为回归系数的Wald χ2检验;OR为优势比;CI为置信区间
下载: 导出CSV
表 6 2组有心脑血管疾病易患因素患者发生MACCE的类别统计[例(%)]
Table 6. Category statistics of major adverse cardiovascular and cerebrovascular events in two groups of patients with cardiovascular and cerebrovascular disease susceptibility factors (case (%))
组别 正常 稳定性心绞痛 恶性心律失常 心梗 支架或搭桥 心源性猝死 脑血管意外 非易损斑块组(n=300) 249(83.0) 23(7.7) 3(1.0) 6(2.0) 7(2.3) 0(0.0) 12(4.0) 易损斑块组(n=200) 78(39.0) 47(23.5) 8(4.0) 8(4.0) 20(10.0) 2(1.0) 37(18.5) 合计 327(65.4) 70(14.0) 11(2.2) 14(2.8) 27(5.4) 2(0.4) 49(9.8) 注:MACCE为主要心脑血管不良事件
下载: 导出CSV
表 7 2组发生心血管不良事件患者的斑块成分及钙化形态特征的比较
Table 7. Comparison of plaque composition and morphological characteristics of calcification between two groups of patients with cardiovascular adverse events
组别 点状钙化斑块
(%)大钙化斑块
(%)CT值( $ \bar x \pm s$ 斑块负荷( $ \bar x \pm s $ 有 无 有 无 ACS患者(n=38) 19(50.0) 19(50.0) 7(18.4) 31(81.6) 78±39 100.6±43.3 SAP患者(n=47) 8(17.0) 39(83.0) 18(38.3) 29(61.7) 114±55 90.3±42.6 χ2值 10.543 3.999 2.330 0.519 P值 0.002 0.046 0.025 0.084 注:ACS为急性冠状动脉综合征;SAP为稳定性心绞痛
下载: 导出CSV
-
[1] 陈伟伟, 高润霖, 刘力生, 等. 《中国心血管病报告2017》概要[J]. 中国循环杂志, 2018, 33(1): 1−8. DOI: 10.3969/j.issn.1000-3614.2018.01.001.
Chen WW, Gao RL, Liu LS, et al. Summary of China cardiovascular disease report 2017[J]. Chin Circ J, 2018, 33(1): 1−8. DOI: 10.3969/j.issn.1000-3614.2018.01.001.[2] Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the heart failure society of America[J]. J Card Fail, 2017, 23(8): 628−651. DOI: 10.1016/j.cardfail.2017.04.014. [3] 林豪, 肖波. 双源CTA对颈动脉与冠状动脉粥样硬化斑块相关性及临床价值研究[J]. 吉林医学, 2020, 41(5): 1108−1112. DOI: 10.3969/j.issn.1004-0412.2020.05.028.
Lin H, Xiao B. Study on the correlation and clinical value of dual-source CTA in carotid artery and coronary atherosclerotic plaque[J]. Jilin Med J, 2020, 41(5): 1108−1112. DOI: 10.3969/j.issn.1004-0412.2020.05.028.[4] Hoffmann U, Massaro JM, D'Agostino RB, et al. Cardiovascular event prediction and risk reclassification by coronary, aortic, and valvular calcification in the framingham heart study[J/OL]. J Am Heart Assoc, 2016, 5(2): e003144[2021-12-11]. https://www.ahajournals.org/doi/10.1161/JAHA.115.003144. DOI: 10.1161/JAHA.115.003144. [5] 葛强, 徐政昊, 袁蔚, 等. 易损斑块相关生物标志物的研究进展[J]. 中国现代医生, 2023, 61(5): 106−110. DOI: 10.3969/j.issn.1673-9701.2023.05.024.
Ge Q, Xu ZH, Yuan W, et al. Research progress of biomarkers related to vulnerable plaque[J]. China Mod Doctor, 2023, 61(5): 106−110. DOI: 10.3969/j.issn.1673-9701.2023.05.024.[6] 刘洋, 张舒媛, 司斌, 等. 冠状动脉CT血管成像检测对冠状动脉易损斑块和主要不良心血管事件风险预测的评估[J]. 中国循环杂志, 2020, 35(9): 894−899. DOI: 10.3969/j.issn.1000-3614.2020.09.008.
Liu Y, Zhang SY, Si B, et al. Atherosclerotic plaque features detected by coronary computed tomography angiography and their roles in predicting the occurrence of future cardiovascular events[J]. Chin Circ J, 2020, 35(9): 894−899. DOI: 10.3969/j.issn.1000-3614.2020.09.008.[7] 李婷婷, 徐香玖. 冠状动脉和颅脑动脉粥样硬化相关性及临床价值[J]. 实用放射学杂志, 2013, 29(7): 1083−1086. DOI: 10.3969/j.issn.1002-1671.2013.07.014.
Li TT, Xu XJ. Correlation of coronary and cerebral atherosclerosis and its clinical value by CT angiography and ultrasonography[J]. J Pract Radiol, 2013, 29(7): 1083−1086. DOI: 10.3969/j.issn.1002-1671.2013.07.014.[8] 郭建华, 沈婕. 正电子示踪剂在动脉粥样硬化易损斑块评价中的应用研究[J]. 国际医学放射学杂志, 2021, 44(6): 712−716. DOI: 10.19300/j.2021.Z18817.
Guo JH, Shen J. Application of positron tracer in the evaluation of atherosclerotic vulnerable plaques[J]. Int J Med Radiol, 2021, 44(6): 712−716. DOI: 10.19300/j.2021.Z18817.[9] 刘淑蓉, 陈国强, 郑亮, 等. CT心脑血管一体化成像的图像质量评价[J]. 国际放射医学核医学杂志, 2018, 42(5): 389−396. DOI: 10.3760/cma.j.issn.1673-4114.2018.05.001.
Liu SR, Chen GQ, Zheng L, et al. Evaluation of the image quality of integrated imaging in coronary combined with carotid and cerebrovascular computed tomography angiography[J]. Int J Radiat Med Nucl Med, 2018, 42(5): 389−396. DOI: 10.3760/cma.j.issn.1673-4114.2018.05.001.[10] 李苏豫, 唐春香, 张龙江. 冠状动脉CT血管成像评估易损斑块新进展[J]. 中华放射学杂志, 2022, 56(3): 330−334. DOI: 10.3760/cma.j.cn112149-20210315-00231.
Li SY, Tang CX, Zhang LJ. Coronary CT angiography of vulnerable plaque[J]. Chin J Radiol, 2022, 56(3): 330−334. DOI: 10.3760/cma.j.cn112149-20210315-00231.[11] 许伟坚, 葛虎, 李琳, 等. 冠状动脉易损斑块行第三代双源CT诊断的价值及相关因素[J]. 智慧健康, 2022, 8(8): 4−7. DOI: 10.19335/j.cnki.2096-1219.2022.08.002.
Xu WJ, Ge H, Li L, et al. The value of third-generation dual-source CT in the diagnosis of vulnerable coronary plaques and related factors[J]. Smart Health, 2022, 8(8): 4−7. DOI: 10.19335/j.cnki.2096-1219.2022.08.002.[12] 高艳, 顾慧, 杨世锋, 等. 基于冠状动脉CT血管成像的斑块定量分析及其与心肌缺血损伤的相关性研究[J]. 中华放射学杂志, 2020, 54(2): 129−135. DOI: 10.3760/cma.j.issn.1005-1201.2020.02.008.
Gao Y, Gu H, Yang SF, et al. Correlation study of coronary plaque quantitative analysis and myocardial ischemic injury based on coronary CT angiography[J]. Chin J Radiol, 2020, 54(2): 129−135. DOI: 10.3760/cma.j.issn.1005-1201.2020.02.008.[13] 王晶, 王全帮, 杨艳, 等. 冠脉CT血管造影对冠心病患者MACE的预测价值[J]. 心血管康复医学杂志, 2022, 31(4): 418−423. DOI: 10.3969/j.issn.1008-0074.2022.04.06.
Wang J, Wang QB, Yang Y, et al. Predictive value of coronary CT angiography for MACE in patients with coronary heart disease[J]. Chin J Cardiovasc Rehabil Med, 2022, 31(4): 418−423. DOI: 10.3969/j.issn.1008-0074.2022.04.06.[14] 王箬芃, 顾慧, 高艳, 等. 基于冠状动脉CT血管成像斑块定量分析探究甘油三酯葡萄糖指数与斑块负荷及斑块易损特征的相关性[J]. 中华放射学杂志, 2021, 55(11): 1153−1160. DOI: 10.3760/cma.j.cn112149-20210323-00263.
Wang RP, Gu H, Gao Y, et al. Correlation study of triglyceride-glucose index and plaque burden and characteristics of vulnerable plaque based on coronary CT angiography plaque quantitative analysis[J]. Chin J Radiol, 2021, 55(11): 1153−1160. DOI: 10.3760/cma.j.cn112149-20210323-00263. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 2208
- HTML全文浏览量: 1817
- PDF下载量: 19
