


-
原发灶不明的淋巴结转移癌主要包括转移性鳞癌和腺癌。Nakamura等[1]认为,在原发灶不明的淋巴结转移癌中鳞癌约占81.1%,其预后较好;腺癌约占7.6%,其中65%来自颈外(肺、胃肠道等),且预后较差。原发灶不明的淋巴结转移癌患者的原发灶通常比较隐匿,常缺乏典型的临床症状,虽采用多种影像学技术检测,往往也难以发现这些病灶,给临床诊断和治疗带来了较大的困难。PET/CT作为一种全身显像技术,兼具功能显像和解剖显像的优势,能够有效避免病灶的遗漏,对于恶性肿瘤的检出有着较高的灵敏度和特异度[2]。但是,18F-FDG PET/CT在原发灶不明的淋巴结转移性鳞癌患者原发灶检测中的具体价值、这类原发恶性肿瘤的相关临床表现及其他常规手段难以检出的原因仍鲜见报道,且无定论[3-4]。为了探讨18F-FDG PET/CT在淋巴结转移性鳞癌患者原发灶检测中的临床价值,本研究对淋巴结转移性鳞癌患者的18F-FDG PET/CT显像结果及临床相关资料进行了回顾性研究,现报道如下。
-
选取2018年3月至2020年11月因发现淋巴结转移性鳞癌(部分病灶病理分化程度明确)而原发灶不明于广东省佛山市禅城区中心医院PET/CT中心行18F-FDG PET/CT检查的56例患者进行回顾性研究,其中男性44例、女性12例,年龄19~81岁,中位年龄51岁。纳入标准:经组织病理学检查确诊为淋巴结转移性鳞癌,检查前未发现可疑原发灶,原发灶经组织病理学检查或临床随访确诊。排除标准:(1)既往有恶性肿瘤病史;(2)不接受长期随访;(3)临床资料不完整。所有患者的淋巴结转移性鳞癌均于18F-FDG PET/CT显像前经过组织病理学检查确诊,原发灶经组织病理学检查或临床随访确诊。所有患者或家属均于检查前签署了知情同意书。本研究符合《赫尔辛基宣言》的原则。
-
显像仪器为德国西门子公司Biograph mCT128型PET/CT。18F-FDG由广东回旋医药科技股份公司的回旋加速器中的模块自动合成,放射化学纯度>95%。
-
患者空腹6 h以上,于平静状态下经手背静脉注射18F-FDG,注射剂量3.70~5.55 MBq/kg。患者于暗室内静卧休息约1 h,排空膀胱后行全身PET/CT显像。先进行CT平扫,参数:管电压120 kV、管电流110 mA、层厚5 mm、间隔5 mm。随后进行PET扫描,采用三维数据采集模式,2 min/床位,扫描范围从股骨中段至颅顶,根据患者身高采集6~8个床位,必要时增加双下肢扫描、局部延迟显像及局部CT薄层扫描。采用CT平扫数据对PET图像进行衰减校正,PET图像采用有序子集最大期望值迭代法重建;CT重建采用标准重建法,矩阵512×512,层厚2 mm。获得PET、CT及PET/CT融合图像后,均通过西门子后处理工作站Syngo.Via进行显示。
-
所有PET/CT融合图像、PET图像和CT图像均进行帧对帧对比分析。PET/CT图像中病灶的18F-FDG摄取明显高于周围组织,且呈结节状、块状或条块状,则诊断为阳性病灶。阳性病灶由2位有多年PET/CT诊断经验的核医学科医师(1位主治医师、1位副主任医师)目测确认,意见不一致时以副主任医师的意见为准。沿异常浓聚病灶周边勾画ROI,由计算机计算SUV,取其SUVmax,结合SUV及相应部位的CT断层图像作出阳性判断。依据组织病理学检查、PET/CT复查、CT、MRI及超声等多项检查及临床随访的综合结果进行最终确诊,随访时间为3~25个月。
-
应用IBM SPSS 20.0软件进行统计学分析。采用双变量相关分析法分析原发灶与淋巴结转移灶的SUVmax的相关性,计算Pearson积差相关系数r。P<0.05为差异有统计学意义。
-
56例淋巴结转移灶鳞癌患者中,18F-FDG PET/CT检测原发灶阳性44例,其中真阳性42例、假阳性2例,检出率为75.0%(42/56)。42例真阳性分别为鼻咽癌26例、喉癌4例、扁桃腺癌3例、颌下腺癌1例、食管癌3例、肺癌3例、宫颈癌2例;2例假阳性均为鼻咽部炎症误诊为鼻咽癌。PET/CT检测原发灶假阴性1例,为鼻咽癌误诊为鼻咽部炎症。另外11例患者18F-FDG PET/CT未发现原发灶,其中1例在1年后的PET/CT随访中确诊为肺癌;其余10例至随访结束仍未找到原发灶(其中5例死亡)。
-
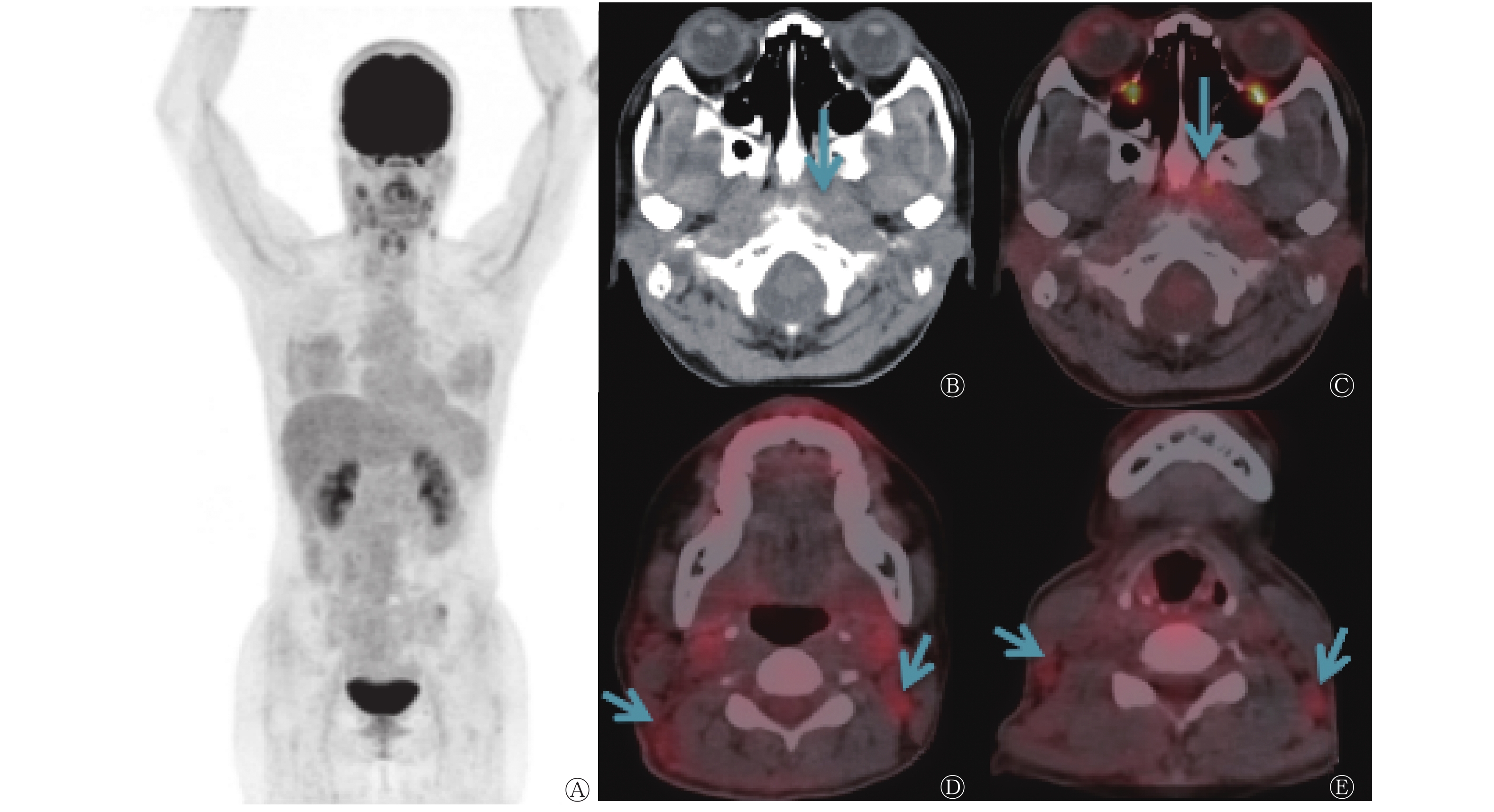
56例淋巴结转移性鳞癌患者中,中上颈部淋巴结转移性鳞癌患者49例,PET/CT检出37例(表1),检出率为75.5%(37/49),其中头颈部肿瘤33例[占89.2%(33/37),分别为鼻咽癌(图1)25例、扁桃体癌3例、颌下腺癌1例、喉癌4例],非头颈部肿瘤4例[占10.8%(4/37),分别为肺癌2例、食管癌1例、宫颈癌1例];锁骨上淋巴结转移性鳞癌患者5例,PET/CT检出4例,检出率为80.0%(4/5),其中头颈部肿瘤1例(鼻咽癌),非头颈部肿瘤3例(食管癌2例、宫颈癌1例);腋下淋巴结转移性鳞癌患者1例,原发灶未检出;腹膜后淋巴结转移性鳞癌患者1例,原发灶为肺癌(PET/CT检出)。
肿瘤原发灶 淋巴结转移灶部位 中上颈部 锁骨上 腹膜后 鼻咽癌 25 1 − 扁桃体癌 3 − − 颌下腺癌 1 − − 喉癌 4 − − 肺癌 2 − 1 食管癌 1 2 − 宫颈癌 1 1 − 总计 37 4 1 注:FDG为氟脱氧葡萄糖;PET/CT为正电子发射断层显像计算机体层摄影术。−表示无此项数据 表 1 18F-FDG PET/CT检出的42例淋巴结转移性鳞癌真阳 性患者淋巴结转移灶部位和肿瘤原发灶的情况(例)
Table 1. Relationship between lymph node metastasis and primary tumor in 42 patients with lymph node metastatic squamous cell carcinoma detected by 18F-FDG PET/CT (case)
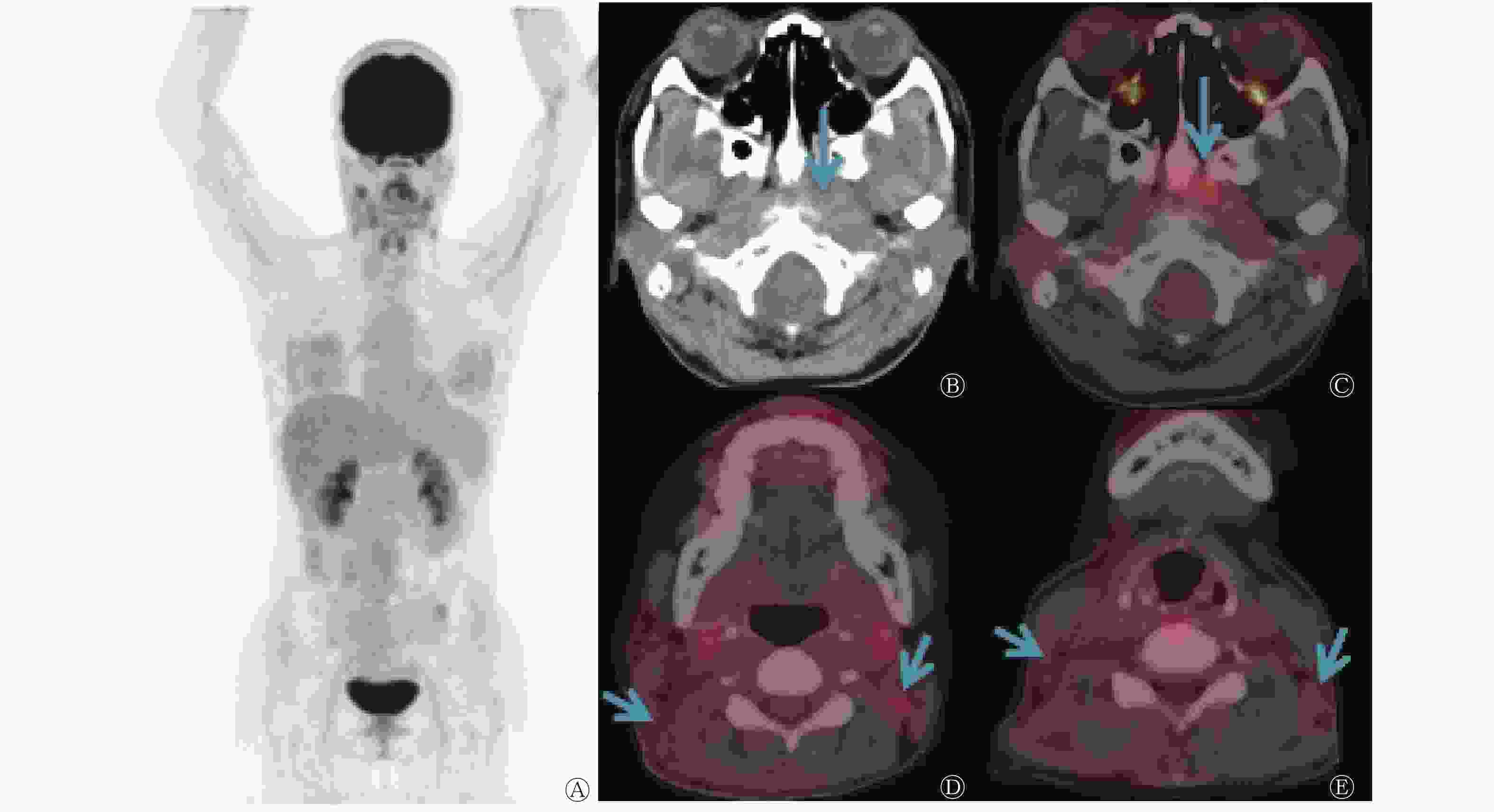
图 1 右颈部淋巴结转移性鳞癌患者(女性,38岁)的18F-FDG PET/CT显像图
Figure 1. 18F-FDG PET/CT images of a patient(female, 38 years old) with right neck lymph node metastatic squamous cell carcinoma
-
56例淋巴结转移性鳞癌患者中,18F-FDG PET/CT检出原发灶44例,其中5例淋巴结转移灶检查时已被局部切除,2例为误诊(假阳性),故最终纳入双变量相关分析的共37例,分析结果表明,原发灶与淋巴结转移灶的SUVmax在一定程度上具有一致性(r=0.320,P=0.027)。
-
56例淋巴结转移性鳞癌患者中,分化程度明确者30例,其中低分化癌25例,18F-FDG PET/CT显像检出原发灶19例(检出率76.0%);中、高分化癌5例,18F-FDG PET/CT显像检出全部原发灶(检出率100%)。
-
近十年来,我国恶性肿瘤的发病率和病死率分别以每年约3.9%和2.5%的速度增长[5-8]。目前,因发现淋巴结肿大且经组织病理学检查诊断为恶性肿瘤,却不伴有其他特定脏器和组织病变的明显临床症状,行多种辅助检查仍未能找到原发灶的患者很多,该问题一直困扰着临床医师、患者及其家属。在原发灶检测方面,常用的方法包括肿瘤标志物检测、影像学检查(超声、CT、MRI、PET、PET/CT)和内镜检查[9]等。鳞癌常发生在鳞状上皮覆盖的部位,如喉、食管、支气管、子宫颈和阴道等部位。淋巴道转移是恶性肿瘤常见的生物学行为,Kazmierczak等[10]发现,影像学检查在颈部淋巴结转移性鳞癌的原发灶检测中具有重要作用,其中全身CT扫描对原发灶的检出率为22%、全身MRI为36%、全身PET/CT为28%~57%,这提示PET/CT在淋巴结转移性鳞癌患者原发灶的检测中具有重要作用。尤其是对转移灶及原发灶的影像学表现不典型的患者,尽管临床上采用范围不断扩大的CT和MRI检查,仍有大部分患者不能确定原发灶。这种情况下,由于原发灶不明确,导致治疗无明确目标、不良反应多,故疗效及预后差。在无典型症状的恶性肿瘤患者原发灶检测中,18F-FDG PET/CT一次检查便可在全身范围探查可疑原发灶和转移灶,明确淋巴结的全身分布和其他组织转移的分期,对原发灶不明转移癌治疗方案的制定有重要价值,尤其是对于头颈部原发灶的检出,为临床决定先手术还是先放化疗提供了重要依据[11] ,也在一定程度上避免了精力和财力的浪费。在指导组织病理学取样方面,18F-FDG PET/CT检查可提供较为准确和有价值的定位,从而提高了活检的阳性率[10]。
本研究56例淋巴结转移性鳞癌患者中, 18F-FDG PET/CT检出原发灶44例,其中28例为鼻咽癌(含误诊2例),这与广东省为鼻咽癌高发省份有一定关系[12]。本研究中原发灶的检出率明显高于以往类似研究得出的结果[13],这可能与本研究中研究对象仅为淋巴结转移性鳞癌患者,以及一部分患者临床症状不典型而导致常规检查手段针对性不强,故原发灶未能及时检出有关。本研究中PET/CT诊断为鼻咽癌的2例患者,组织病理学检查结果证实为鼻咽部炎症;而PET/CT诊断为鼻咽部炎症的1例患者,组织病理学检查结果证实为鼻咽癌。对于鼻咽部PET/CT诊断为阳性的病灶,炎症与肿瘤的鉴别仍然是诊断的难点,需结合病史及病灶形态进行综合判断,而鼻咽部代谢增高病灶的组织病理学检查仍然是治疗前的必要步骤。本研究11例原发灶未检出的患者中,1例PET/CT显像全阴性患者1年后复查PET/CT发现右肺癌且伴全身广泛转移;另10例至随访结束,原发灶仍未明确,可能的原因如下:(1)原发灶微小,在目前的显像分辨率下无法被显示出;(2)转移灶太多太大,原发灶隐藏于其中;(3)原发灶可能已经消失。
肿瘤转移不是随机的,而是具有转移途径的倾向性[14],也有转移概率及发生转移时间的差别。掌握肿瘤转移的特点和规律,对临床诊治有重要意义。王成锋和赵平[15]对1273例原发灶不明的肿瘤患者进行的回顾性研究结果显示,肿瘤好发转移部位中67%为淋巴结,以颈部淋巴结为主。本研究中淋巴结转移灶首发部位为颈部的患者占87.5%(49/56),这可能与本研究的病例数较少有关。本研究中绝大多数患者的淋巴结转移情况符合恶性肿瘤的常规转移规律,但在研究中意外发现了国内外鲜见报道的淋巴结转移情况2例:1例锁骨上淋巴结转移性鳞癌原发灶为宫颈癌,另1例腹膜后淋巴结转移性鳞癌原发灶为肺癌。这2例患者在未行PET/CT检查前无原发灶肿瘤的相关症状。按照淋巴结的常规转移规律,腹膜后区域以及腹腔脏器的繁多使得腹膜后区域的肿瘤转移情况往往很难得到清晰显示,进行针对性的传统局部影像学检查很难发现以上2例患者的原发灶,18F-FDG PET/CT全身显像不仅为这类患者提供了原发灶的诊断,而且明确了周围组织和脏器受侵犯的具体情况。
刘方颖等[16]的研究结果显示,非小细胞肺癌增殖细胞核抗原高表达者具有18F-FDG高摄取的趋势。增殖细胞核抗原是一种仅在增殖细胞中合成或表达的核内多肽,其含量变化与DNA合成具有一致性,其高表达提示细胞内DNA合成活跃,是临床判断肿瘤细胞增殖和恶性程度的常用指标之一。本研究结果显示,37例患者原发灶SUVmax与淋巴结转移灶SUVmax具有一致性,提示肿瘤的转移灶与原发灶的肿瘤细胞增殖能力可能具有一致性。基于这一特性,在肿瘤的临床分期、疗效评价、复发及转移监测方面,18F-FDG PET/CT显像能够根据病灶代谢程度提示恶性肿瘤的边界、区别坏死与复发或残留组织。但由于本研究的病例数有限,此结论尚需扩大样本量进一步探讨。
肿瘤分化程度越低,说明恶性程度越高,对放化疗越敏感,这些低分化肿瘤患者的原发灶若能被及早诊断,患者的生存质量无疑将得到很大的提高。殷玉林等[17]对颈部原发灶不明转移癌的研究结果显示,中上颈淋巴结低分化转移癌的原发灶多数来自头颈部肿瘤,特别是鼻咽部,其分化程度低,恶性程度高,对放化疗敏感。本研究56例淋巴结转移性鳞癌患者中,分化程度明确者30例,18F-FDG PET/CT检查对低分化鳞癌患者具有较高的检出率,为其治疗争取了时间。本研究中,中高分化癌患者较少,故18F-FDG PET/CT在这类患者原发灶检测中的价值仍有待进一步扩大样本量进行研究证实。
PET/CT的出现是影像医学发展中的一个里程碑,其提供了一种全新的检测原发灶的方法。但是,由于炎症同样可以引起18F-FDG高代谢,部分特定组织类型的恶性肿瘤[18](如肾透明细胞癌、卵巢囊腺癌、胰腺癌、肝癌等)对18F-FDG的摄取不敏感,这些问题的解决还有待于新型药物的研发、临床的合理使用以及临床诊断经验的不断总结。近年来,68Ga-成纤维细胞激活蛋白抑制剂在多种上皮恶性肿瘤显像方面的研究陆续展开,有学者发现68Ga-成纤维细胞激活蛋白抑制剂 PET/CT在食管癌中显示了明显的肿瘤部位显像剂浓聚,可为靶区容积的确定提供额外的信息,有助于避免肿瘤的漏诊[19];另外,还有学者发现68Ga-成纤维细胞激活蛋白抑制剂 PET/CT在一定程度上发现了更多的原发灶和转移灶[20]。但由于经验有限,仍需要进一步的研究探讨。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 张冬萍负责现场的试验、数据的获取与分析、论文的撰写与修改;李莹负责现场的试验;刘雨琪负责数据的获取与分析;周智洋负责论文的审阅。
18F-FDG PET/CT检测淋巴结转移性鳞癌原发灶的价值
The value of 18F-FDG PET/CT imaging in detecting the primary foci of lymph node metastatic squamous cell carcinoma
-
摘要:
目的 探讨18F-氟脱氧葡萄糖(FDG) PET/CT在淋巴结转移性鳞癌原发灶检测中的临床应用价值。 方法 选取2018年3月至2020年11月于广东省佛山市禅城区中心医院因发现淋巴结转移性鳞癌而原发灶不明行全身18F-FDG PET/CT检查的56例患者进行回顾性研究,其中男性44例、女性12例,年龄19~81岁,中位年龄51岁。所有患者的淋巴结转移性鳞癌均于18F-FDG PET/CT显像前经组织病理学检查确诊,原发灶经组织病理学检查或临床随访确诊。分析并计算18F-FDG PET/CT检测原发灶的检出率;原发灶与淋巴结转移部位、最大标准化摄取值(SUVmax)的关系。采用双变量相关分析法分析原发灶与淋巴结转移灶的SUVmax的相关性。 结果 56例患者中,18F-FDG PET/CT检测原发灶阳性44例(真阳性42例、假阳性2例),检出率为75.0%;假阴性1例(鼻咽癌);11例患者18F-FDG PET/CT未发现原发灶。双变量相关分析结果显示,原发灶与淋巴结转移灶的SUVmax在一定程度上具有一致性(r=0.320,P<0.05)。 结论 18F-FDG PET/CT显像对淋巴结转移性鳞癌的不明原发灶检测具有较好的临床应用价值,淋巴结转移灶与原发灶的18F-FDG代谢强度存在良好的相关性。 -
关键词:
- 肿瘤,未知原发灶 /
- 淋巴结转移 /
- 癌,鳞状细胞 /
- 氟脱氧葡萄糖F18 /
- 正电子发射断层显像术 /
- 体层摄影术,X线计算机 /
- 最大标准化摄取值
Abstract:Objective To investigate the clinical value of 18F-FDG PET/CT imaging in detecting primary foci by analyzing images of squamous carcinoma patients with lymph node metastatic. Methods A retrospective analysis was performed on 56 patients (44 males and 12 females, aged 19−81, with a median age of 51), who underwent whole-body 18F-FDG PET/CT for the diagnosis of metastatic squamous carcinoma with unknown primary foci during March 2018 to November 2020 at the Central Hospital of Chancheng District of Foshan City in Guangdong Province. Prior to imaging, the diagnosis of metastatic squamous cell carcinoma was confirmed by pathological examination in all patients, and the primary foci were confirmed by pathological examination or clinical follow-up. To analyze and calculate the detection rate of 18F-FDG PET/CT in the diagnosis of primary lesion and the relationship between primary lesion and lymph node metastasis and maximum standardized uptake value (SUVmax). SUVmax of primary tumor and lymph node metastasis were analyzed by bivariable correlation analysis. Results Among 56 patients, 44 positive cases (42 true positive cases and 2 false positive cases) were detected by 18F-FDG PET/CT, with a detection rate of 75.0% and 1 false negative (nasopharyngeal carcinoma). Primary foci in 11 patients remained unfound by 18F-FDG PET/CT. The SUVmax of primary and metastatic foci were consistent to some extent (r=0.320, P<0.05). Conclusion 18F-FDG PET/CT imaging has good clinical value for the detection of unspecified primary foci in metastatic squamous cell carcinoma, and there is a good correlation between the intensity of glucose metabolism in the primary foci and metastatic foci. -
图 1 右颈部淋巴结转移性鳞癌患者(女性,38岁)的18F-FDG PET/CT显像图
Figure 1. 18F-FDG PET/CT images of a patient(female, 38 years old) with right neck lymph node metastatic squamous cell carcinoma
表 1 18F-FDG PET/CT检出的42例淋巴结转移性鳞癌真阳 性患者淋巴结转移灶部位和肿瘤原发灶的情况(例)
Table 1. Relationship between lymph node metastasis and primary tumor in 42 patients with lymph node metastatic squamous cell carcinoma detected by 18F-FDG PET/CT (case)
肿瘤原发灶 淋巴结转移灶部位 中上颈部 锁骨上 腹膜后 鼻咽癌 25 1 − 扁桃体癌 3 − − 颌下腺癌 1 − − 喉癌 4 − − 肺癌 2 − 1 食管癌 1 2 − 宫颈癌 1 1 − 总计 37 4 1 注:FDG为氟脱氧葡萄糖;PET/CT为正电子发射断层显像计算机体层摄影术。−表示无此项数据  下载: 导出CSV
下载: 导出CSV
-
[1] Nakamura A, Iguchi H, Takayama M, et al. Metastatic carcinoma of the neck from unknown primary sites[J]. Nihon Jibiinkoka Gakkai Kaiho, 2003, 106(6): 671−677. DOI: 10.3950/jibiinkoka.106.671. [2] 李嘉旭, 许璐, 李梦丹, 等. 18F-FDG PET/CT全身显像对原发不明转移瘤患者原发灶检出价值的Meta分析[J]. 第三军医大学学报, 2020, 42(13): 1360−1369. DOI: 10.16016/j.1000-5404.202002104.
Li JX, Xu L, Li MD, et al. Diagnostic value of whole body 18F-FDG PET/CT imaging in metastatic cancer of unknown primary: a Meta-analysis[J]. J Third Mil Med Univ, 2020, 42(13): 1360−1369. DOI: 10.16016/j.1000-5404.202002104.[3] Rudmik L, Lau HY, Matthews TW, et al. Clinical utility of PET/CT in the evaluation of head and neck squamous cell carcinoma with an unknown primary: a prospective clinical trial[J]. Head Neck, 201l, 33(7): 935−940. DOI: 10.1002/hed.21566. [4] Deron PB, Bonte KM, Vermeersch HF, et al. Lymph node metastasis of squamous cell carcinoma from an unknown primary in the upper and middle neck: impact of 18F-fluorodeoxyglucose positron emission tomography/computed tomography[J]. Cancer Biother Radiopharm, 2011, 26(3): 331−334. DOI: 10.1089/cbr.2010.0918. [5] Chen WQ, Zheng RS, Zuo TT, et al. National cancer incidence and mortality in China, 2012[J]. Chin J Cancer Res, 2016, 28(1): 1−11. DOI: 10.3978/j.issn.1000-9604.2016.02.08. [6] Chen WQ, Zheng RS, Zhang SW, et al. Cancer incidence and mortality in China, 2013[J]. Cancer Lett, 2017, 401: 63−71. DOI: 10.1016/j.canlet.2017.04.024. [7] Chen WQ, Sun KX, Zheng RS, et al. Cancer incidence and mortality in China, 2014[J]. Chin J Cancer Res, 2018, 30(1): 1−12. DOI: 10.21147/j.issn.1000-9604.2018.01.01. [8] 郑荣寿, 顾秀瑛, 李雪婷, 等. 2000−2014年中国肿瘤登记地区癌症发病趋势及年龄变化分析[J]. 中华预防医学杂志, 2018, 52(6): 593−600. DOI: 10.3760/cma.j.issn.0253-9624.2018.06.007.
Zheng RS, Gu XY, Li XT, et al. Analysis on the trend of cancer incidence and age change in cancer registry areas of China, 2000 to 2014[J]. Chin J Prev Med, 2018, 52(6): 593−600. DOI: 10.3760/cma.j.issn.0253-9624.2018.06.007.[9] 温树信, 张庆丰, 王鑫, 等. 原发灶不明的颈部淋巴结转移癌诊治策略[J]. 临床耳鼻咽喉头颈外科杂志, 2019, 33(11): 1014−1016. DOI: 10.13201/j.issn.1001-1781.2019.11.002.
Wen SX, Zhang QF, Wang X, et al. The scheme of diagnosis and treatment on metastatic cervical carcinomas from an unknown primary[J]. J Clin Otorhinolaryngol Head Neck Surg (China), 2019, 33(11): 1014−1016. DOI: 10.13201/j.issn.1001-1781.2019.11.002.[10] Kazmierczak PM, Nikolaou K, Rominger A, et al. Radiological diagnostics in CUP syndrome[J]. Radiologe, 2014, 54(2): 117−123. DOI: 10.1007/s00117-013-2547-9. [11] AAssar OS, Fischbein NJ, Caputo GR, et al. Metastatic head and neck cancer: role and usefulness of FDG PET in locating occult primary tumors[J]. Radiology, 1999, 210(1): 177−181. DOI: 10.1148/radiology.210.1.r99ja48177. [12] Wei KR, Zheng RS, Zhang SW, et al. Nasopharyngeal carcinoma incidence and mortality in China, 2013[J]. Chin J Cancer, 2017, 36(1): 90. DOI: 10.1186/s40880-017-0257-9. [13] Al-Brahim N, Ross C, Carter B, et al. The value of postmortem examination in cases of metastasis of unknown origin-20-year retrospective data from a tertiary care center[J]. Ann Diagn Pathol, 2005, 9(2): 77−80. DOI: 10.1016/j.anndiagpath.2004.12.003. [14] 王文萍. 实用肿瘤转移学[M]. 沈阳: 辽宁科学技术出版社, 2003: 20.
Wang WP. Practical oncology metastasis[M]. Shenyang: Liaoning Science and Technology Publishing House, 2003: 20.[15] 王成锋, 赵平. 应重视不明原发灶肿瘤的临床研究[J]. 中华医学杂志, 2006, 86(26): 1801−1803. DOI: 10.3760/j:issn:0376-2491.2006.26.001.
Wang CF, Zhao P. Clinical research of cancers of unknown primary deserves special emphasis[J]. Natl Med J China, 2006, 86(26): 1801−1803. DOI: 10.3760/j:issn:0376-2491.2006.26.001.[16] 刘方颖, 王全师, 裴著果. 非小细胞肺癌18F-FDG PET显像与增殖细胞核抗原表达的关系[J]. 中华核医学杂志, 2003, 23(1): 14−16. DOI: 10.3760/cma.j.issn.2095-2848.2003.01.004.
Liu FY, Wang QS, Pei ZG. 18F-FDG uptake in PET imaging correlates with the proliferating cell nuclear antigen in non-small cell lung cancer[J]. Chin J Uncl Med, 2003, 23(1): 14−16. DOI: 10.3760/cma.j.issn.2095-2848.2003.01.004.[17] 殷玉林, 唐平章, 徐国镇, 等. 颈部原发不明转移癌的治疗与转归[J]. 中华肿瘤杂志, 1999, 21(3): 230−232. DOI: 10.3760/j.issn:0253-3766.1999.03.021.
Yin YL, Tang PZ, Xu GZ, et al. Treatment and outcome of cervical lymph nodal metastases of unknown primary sites[J]. Chin J Oncol, 1999, 21(3): 230−232. DOI: 10.3760/j.issn:0253-3766.1999.03.021.[18] 徐晓辉, 何涛, 王欢. 18F-FDG PET/CT在胃癌术后复发及转移监测中的应用[J]. 中国CT和MRI杂志, 2021, 19(10): 152−154. DOI: 10.3969/j.issn.1672-5131.2021.10.049.
Xu XH, He T, Wang H. Application of 18F-FDG PET/CT in monitoring of recurrence and metastasis after gastric cancer surgery[J]. Chin J CT MRI, 2021, 19(10): 152−154. DOI: 10.3969/j.issn.1672-5131.2021.10.049.[19] Zhao L, Chen SY, Chen SJ, et al. 68Ga-fibroblast activation protein inhibitor PET/CT on gross tumour volume delineation for radiotherapy planning of oesophageal cancer[J]. Radiother Oncol, 2021, 158: 55−61. DOI: 10.1016/j.radonc.2021.02.015. [20] Hicks RJ, Roselt PJ, Kallur KG, et al. FAPI PET/CT: will it end the hegemony of 18F-FDG in oncology?[J]. J Nucl Med, 2021, 62(3): 296−302. DOI: 10.2967/jnumed.120.256271. -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 3386
- HTML全文浏览量: 1923
- PDF下载量: 13