















-
容积旋转调强放疗(volume-modulated arc therapy, VMAT)的图像引导技术能够有效监测治疗中靶区运动,防止等中心发生位移,从而保证输出剂量的准确性和保护周围正常组织[1-2]。在各种基于植入标志物校准的前列腺癌VMAT图像引导技术中,千伏级锥形束CT的应用较为广泛[3-4],但额外产生的辐射剂量相对较高,可能对患者造成影响[5-8]。而利用治疗射线进行成像的兆伏级电子射野影像装置(electronic portal imaging device, EPID)则不存在额外辐射剂量的问题,且能节省治疗时间[9-11]。但是,EPID的图像质量劣于锥形束CT,如何在现有基础上最大程度提高EPID的校准精度具有重要的研究意义[12]。
在现有基础上基于植入标志物的EPID校准精度关键取决于标志物质心准确性[12-13],质心准确性又取决于标志物的可探测性,而可探测性主要受标志物植入位置的影响。因此,标志物植入位置极大地影响了前列腺癌图像引导放疗(image-guided radiotherapy, IGRT)设备的校准精度,寻找标志物最佳植入位置具有重要临床意义,甚至关乎EPID的应用前景。本研究通过寻找多种情况下植入标志物最高可探测性分数位置,旨在提高前列腺癌IGRT的校准精度和疗效。
-
利用超声引导针和网格模板[14](美国CIVCO公司)将4枚线性金标志物(0.8 mm×0.8 mm×1.0 mm,比利时IBA公司)植入到Random仿真人体模型(比利时IBA公司)的盆腔部位。定义坐标轴:X轴为左右方向、Y轴为头脚方向、Z轴为腹背方向。标志物按照4种模式植入:X-Z平面植入(A模式)、X-Y平面植入(B模式)、斜植入(C模式)和分散植入(D模式)。其中,A模式下植入坐标为(−3a,0,0)、(−a,0,0)、(a,0,0)、(3a,0,0)和(a,0,a)、( −a,0,a)、( a,0,−a)、(−a,0,−a);B模式下植入坐标为(a,b,0)、(−a,b,0)、(a,−b,0)、(−a,−b,0);C模式下植入坐标为(a,b,a)、(−a,b,−a)、(a,−b,a)、(−a,−b,−a);D模式下植入坐标为(0,3b,0)、(a,b,a)、(−a,−b,−a)、(0,−3b,0)。每种植入模式下的组级坐标组合分别见表1~4。
参数值 b=0 a=5 A5-Ⅰc a=5 A5-Ⅱd a=10 A10-Ⅲd a=15 A15-Ⅳd 注:c表示植入坐标为(−3a,0,0)、(−a,0,0)、(a,0,0)、(3a,0,0)时的组级坐标组合;d表示植入坐标为(a,0,a)、(−a,0,a)、(a,0,−a)、(−a,0,−a)时的组级坐标组合。每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如A5-Ⅰ坐标组合代入参数a=5和b=0后,得到A5-Ⅰ组4枚标志物坐标:(−15,0,0)、(−5,0,0)、(5,0,0)、(15,0,0),a和b单位为mm 表 1 VMAT标志物植入的X-Z平面(Y=0)(模式A)下 4种组级坐标组合
Table 1. Four group-level coordinate combinations under marker implantation mode A on the X-Z plane (Y=0) in volume-modulated arc therapy
参数值 b=1.0 b=3.0 b=5.0 b=6.7 a=5 D5-Ⅰ D5-Ⅱ D5-Ⅲ D5-Ⅳ a=10 D10-Ⅰ D10-Ⅱ D10-Ⅲ D10-Ⅳ a=15 D15-Ⅰ D15-Ⅱ D15-Ⅲ D15-Ⅳ 注:每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如D5-Ⅰ坐标组合代入参数a=5和b=1后,得到D5-Ⅰ组4枚标志物坐标:(0,3,0)、(5,1,5)、(−5,−1,−5)、(0,−3,0),a和b单位为mm 表 4 VAMT标志物植入的分散植入(模式D)下12种组 级坐标组合(X,Y,Z≠0)
Table 4. Twelve group-level coordinate combinations under marker dispersed implantation mode D (X,Y,Z≠0) in volume- modulated arc therapy
参数值 b=3 b=9 b=15 b=20 a=5 B5-Ⅰ B5-Ⅱ B5-Ⅲ B5-Ⅳ a=10 B10-Ⅰ B10-Ⅱ B10-Ⅲ B10-Ⅳ a=15 B15-Ⅰ B15-Ⅱ B15-Ⅲ B15-Ⅳ 注:每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如B5-Ⅰ坐标组合代入参数a=5和b=3后,得到B5-Ⅰ组4枚标志物坐标:(5,3,0)、(−5,3,0)、(5,−3,0)、(−5,−3,0),a和b单位为mm 表 2 VMAT标志物植入的X-Y平面(Z=0)(模式B)下 12种组级坐标组合
Table 2. Twelve group-level coordinate combinations under marker implantation mode B on the X-Y plane (Z=0) in volume- modulated arc therapy
参数值 b=3 b=9 b=15 b=20 a=5 C5-Ⅰ C5-Ⅱ C5-Ⅲ C5-Ⅳ a=10 C10-Ⅰ C10-Ⅱ C10-Ⅲ C10-Ⅳ a=15 C15-Ⅰ C15-Ⅱ C15-Ⅲ C15-Ⅳ 注:每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如C5-Ⅰ坐标组合代入参数a=5和b=3后,得到C5-Ⅰ组4枚标志物坐标:(5,3,5)、(−5,3,−5)、(5,−3,5)、(−5,−3,−5),a和b单位为mm 表 3 VAMT标志物植入的斜植入(模式C)下12种组级 坐标组合(X,Y,Z≠0)
Table 3. Twelve group-level coordinate combinations under marker oblique implantation mode C (X,Y,Z≠0) in volume- modulated arc therapy
-
调取25例治疗已结束的前列腺癌患者的VMAT计划(每例2个对称弧,共50个弧),使用Synergy Platform加速器(瑞典医科达公司)分别对包含4枚标志物的40种坐标组合的盆腔假体进行基于EPID的IGRT标准照射,单次剂量约为60 Gy。在照射中,从弧上每个控制点获取EPID平片并用于下一步计算和分析。
-
定义在EPID平片上,若以标志物中心为圆心,半径r=3 mm的圆内区域未被多叶准直器或铅门全部遮挡,则该标志物是可探测的。计算每个控制点
$ j $'/> 处所获得的EPID平片上标志物$ i $ 的未遮挡区域u的面积$ {A}_{u}^{ij} $ 。控制点$ j $'/> 处可探测性分数为4枚标志物的未遮挡面积总和占总面积A的百分比,总面积A=$ 4 \times \pi {r^2}$ ,其中r=3 mm 。另外,本实验还引入了2种加权因子:标志物数量加权因子
$ {W}_{n} $ 和标志物重叠加权因子$ {W}_{o} $ ,分别惩罚每张EPID平片上可探测到的标志物数量n<3和每张EPID平片上发生标志物重叠的情况。(1)标志物数量加权因子
$ {W}_{n} $'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/> :首先,规定若任一枚标志物实际未遮挡或未重叠面积大于以标志物中心为圆心的圆面积(半径r=3 mm)的3/4,即总面积A的3/16时,则可探测标志物数量+1。然后,规定每张EPID平片上可探测到的标志物数量n≥3时,$ {W}_{n} $'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/> =1;n=2时,$ {W}_{n} $'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/> =2/3;n=1时,$ {W}_{n} $'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/> =1/3;n=0时,$ {W}_{n} $'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/>'/> =0。(2)标志物重叠加权因子
$ {W}_{o} $'/>'/>'/>'/>'/>'/>'/> :规定在每张EPID平片上,4枚标志物均未发生重叠时,$ {W}_{o} $'/>'/>'/>'/>'/>'/>'/> =1;2枚标志物发生重叠时,$ {W}_{o} $'/>'/>'/>'/>'/>'/>'/> =0.5;3枚及以上标志物发生重叠时,$ {W}_{o} $'/>'/>'/>'/>'/>'/>'/> =1/3。最终,完善后的可探测性分数D的计算公式如下:
$ D{\text{=}}{W}_{n}\times {W}_{o}\times \dfrac{{ \displaystyle \sum }_{1}^{4}{A}_{u}^{ij}}{A} $ 利用公式(1)计算每种植入模式中每种坐标组合在每次IGRT标准照射后全部控制点所获得的EPID平片的可探测性分数,最后计算每种坐标组合25次照射的可探测性分数的均值(
$\overline{D}$ )。 -
分析40种坐标组合的
$\overline{D}$'/> ,确定标志物最佳植入坐标组合与模式。另外,考虑到临床实践中由于患者前列腺体差异和操作条件的不同,并不是所有患者均适用于上述结果。因此,本研究应用SPSS 19.0软件的曲线拟合功能寻找标志物在所有模式下及坐标组合中的最佳植入位置参数a值和b值,从而使得某些不适用上述结果的患者仍可在其他模式下或坐标组合中获得相对较高的$\overline{D}$'/> ,计算方法如下。(1)a值:除A模式外(A模式下直接计算4个坐标组合的
$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 与a值的关系即可),分别计算每种模式下,每个a值组4个坐标组合(例如:B5-Ⅰ、B5-Ⅱ、B5-Ⅲ、B5-Ⅳ)的$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 。建立a值与$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 的函数关系,进行曲线拟合,寻找最大$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 时的a值。(2)b值:除A模式外(A模式下b值均为0,直接计算4个坐标组合的
$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 与b值的关系即可),分别计算每种模式下,每个b值组3个坐标组合(例如:B5-Ⅰ、B10-Ⅰ、B15-Ⅰ)的$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 。建立b值与$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 的函数关系,进行曲线拟合,寻找最大$\overline{D}$'/>'/>'/>'/>'/>'/>'/> 时的b值。 -
40个组级坐标组合25次照射的
$\overline{D}$ 按降序排列的结果见图1,按模式A~D排列的结果见图2。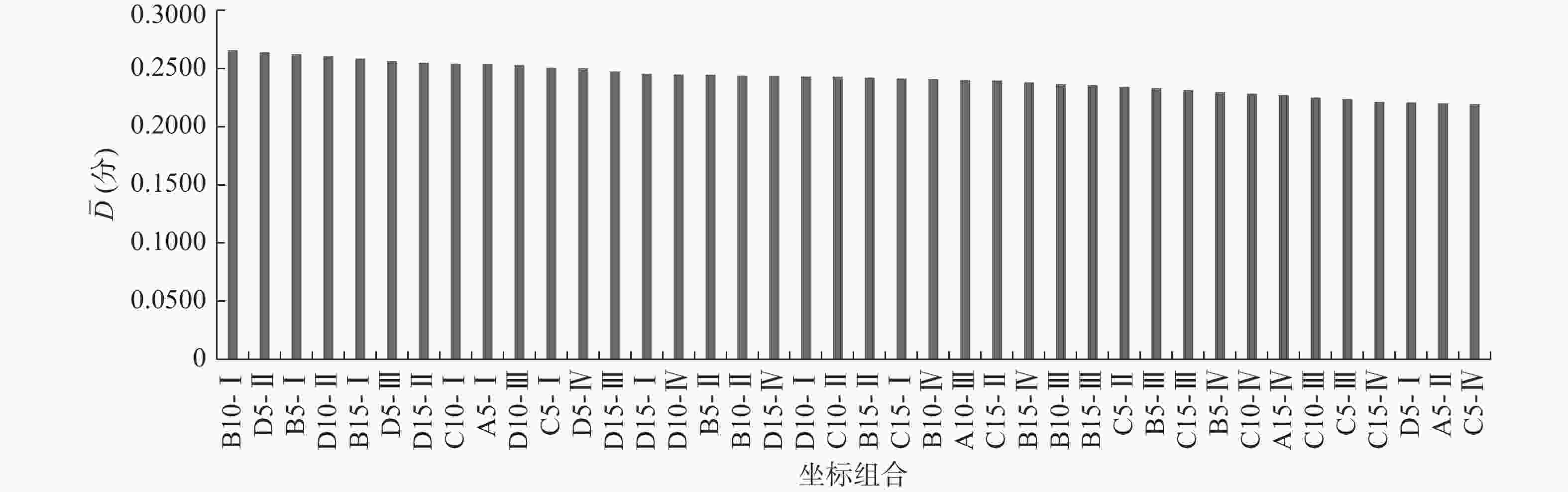
图 1 VMAT标志物植入中40个组级坐标组合25次照射的可探测性分数均值(
$ \overline{D} $ )按降序排列的结果Figure 1. The mean detectability score
$\overline{D} $ for 40 group-level coordinate combinations after 25 times of radiation in volume-modulated arc therapy marker implantation is arranged in descending order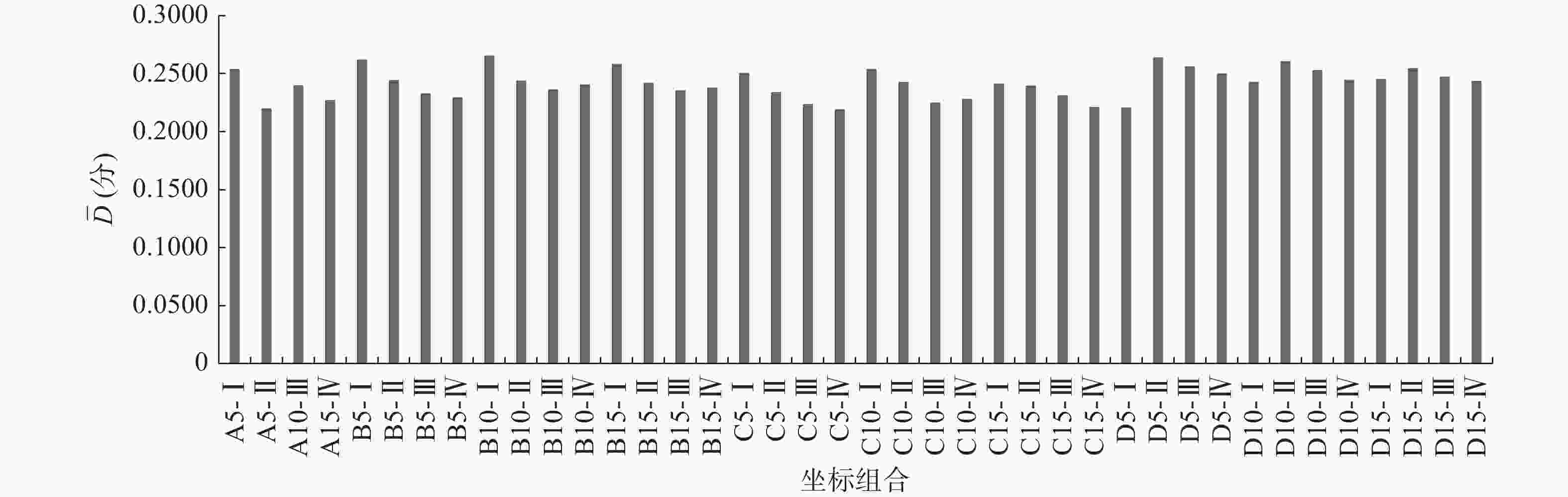
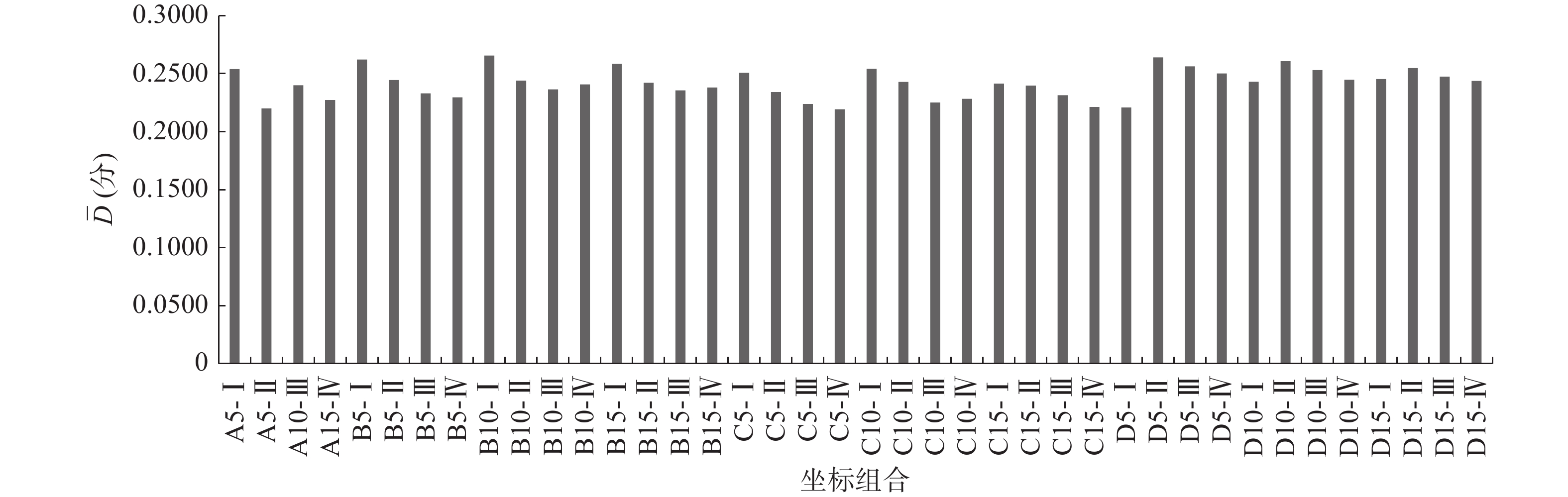
图 2 VMAT标志物植入中40个组级坐标组合25次照射的可探测性分数均值(
$\overline{D} $ )按模式A~D排列的结果Figure 2. The mean detectability score
$ \overline{D}$ for 40 group-level coordinate combinations after 25 times of radiation volume-modulated arc therapy marker implantation is arranged in mode A−D order -
由图1(组级结果)可见,B10-Ⅰ组
$\overline{D}$'/>'/>'/> 最高(0.2652分),C5-Ⅳ组最低(0.2191分)。由图2(模式级结果)可见,每种模式的相同a值组中,$\overline{D}$'/>'/>'/> 基本随着b值的增加而降低;4种模式中D模式的$\overline{D}$'/>'/>'/> 的均值最高(0.2489分),其余依次为B模式(0.2447分)、A模式(0.2357分)、C模式(0.2350分)。由此可见,本研究中最佳植入坐标组合为B10-Ⅰ组,即(10,3,0)、(−10,3,0)、(10,−3,0)、(−10,−3,0),最佳植入模式为D模式。 -
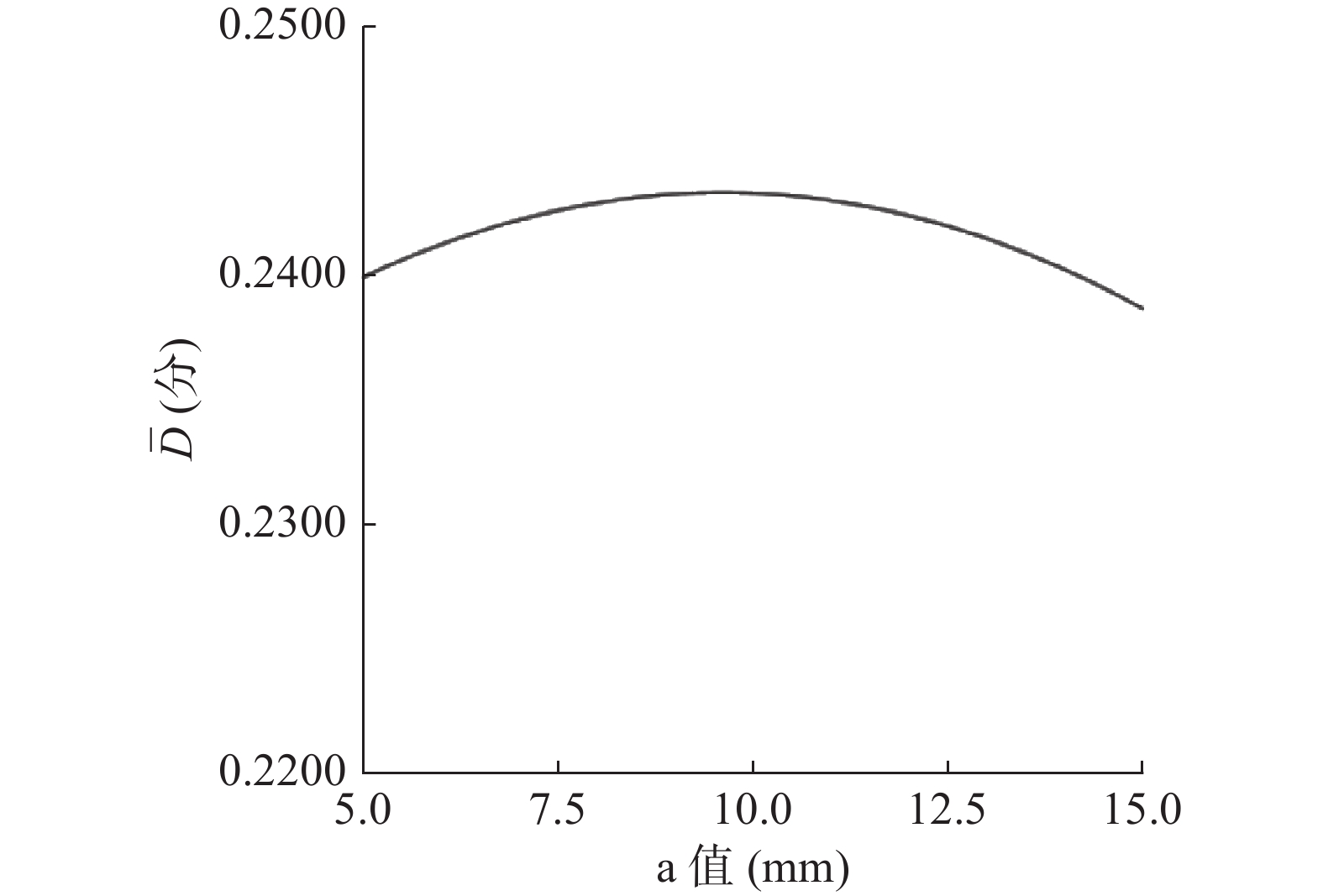
a、b值分别与
$\overline{D}$'/> 拟合的曲线见图3、4。其中,由图3可见,拟合曲线R2=0.237,拟合结果差,曲线峰值处横坐标a=9.6 mm;由图4可见,拟合曲线R2=0.721,拟合结果良好,曲线峰值处横坐标b=4.6 mm。综上,当a=9.6 mm、b=4.6 mm时,各种模式下均能获得较为理想的$\overline{D}$'/> 。
图 3 VMAT标志物植入中植入坐标参数a值同可探测性分数均值(
${ \overline{D}} $ )的拟合曲线Figure 3. Fitting curve of the implantation coordinate parameter a and the mean detectability score
$\overline{D} $ in volume-modulated arc therapy marker implatation
图 4 VMAT标志物植入中植入坐标参数b值同可探测性分数均值(
$\overline{D}$ )的拟合曲线Figure 4. Fitting curve of the implantation coordinate parameter b and the mean detectability score
$\overline{D}$ in volume-modulated arc therapy marker implatation -
本研究结果显示,对于常规患者(腺体完整,无残缺或畸形),组级最佳结果为B10-Ⅰ,模式级最佳结果为D模式。因此,在充分考虑了手术操作难易程度,是否会给患者带来不良影响等问题后,可参考上述结果进行标志物的植入。通过上述操作,可以最大程度地提高标志物的可探测性,进而提高其质心准确性,从而优化EPID的校准精度。
本研究中曲线拟合结果还显示,纵坐标(
$\overline{D}$ )随横坐标(a值或b值)变化的趋势均为先上升、后下降。对此,可能的原因如下。(1)曲线上升部分:当标志物距离中心原点位置过近时,由于缺乏外周标志物探测信息,无法准确反映前列腺靶区的旋转变化。随着a值和b值逐渐增大,标志物距离中心原点距离增加,外周标志物探测信息逐渐丰富,因此能够较准确地反映前列腺靶区旋转变化,总体探测分数逐渐增加。(2)曲线下降部分:在VMAT典型弧形野中,动态多叶准直器最有可能在前列腺靶区治疗等中心原点周围打开,距离中心较近的标志物被多叶准直器遮挡的概率不大。随着射野中心距离的增加,外周标志物被多叶准直器遮挡的概率大大增加,因此$\overline{D} $'/> 呈现快速下降的趋势。以上2种解释同样适用于所有组级坐标组合$\overline{D} $'/> 按模式排列结果中A、B、C模式的下降部分和D模式。Ma等[14]也利用相同的理论解释了相似的实验结果。总之,标志物在X、Y、Z 3个方向上相对中心原点的坐标是决定其可探测性分数的主要因素,过小或过大的直线距离分别会导致旋转信息量的减少和多叶准直器遮挡概率的增加[15],因此,将可探测性分数峰值处的a值和b值代入并应用到各种模式中,计算出的最佳坐标组合即为各种模式下标志物最理想的植入位置。对于一些前列腺靶区情况复杂、植入操作特殊的患者(如前列腺癌术后放疗患者、腺体残缺患者),或许不适合参考最佳组级,甚至模式级结果进行植入手术,上述结果为这类患者在其他坐标组合或模式下进行手术提供了重要临床参考。
综上,本研究获得了标志物最佳植入位置的组级和模式级结果,同时通过对该结果进行拟合曲线分析获得了所有情况下各种模式和坐标组合均较为理想的参数。本研究结果不仅充分考虑了常规和特殊患者的临床实践情况,具有普适性,同时也为基于EPID联合标志物的前列腺癌IGRT提供了重要临床参考数据和依据,从而提高了其校准精度和治疗效果,拓宽了EPID的应用前景。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 田龙负责研究过程的实施、实验的实施、论文的起草和最终版本的修订;闫洁诚、李丹、李慧超负责数据的获取与分析;胡逸民负责研究命题的提出和设计。
前列腺癌容积旋转调强放疗中标志物可探测性研究
Research on detectability of markers in volume-modulated arc therapy for prostate cancer
-
摘要:
目的 量化前列腺癌容积旋转调强放疗中植入标志物的可探测性,寻找最佳植入位置。 方法 (1)依次将标志物植入4种模式下盆腔假体内不同既定坐标组合处。(2)调取25例既往前列腺癌患者的容积旋转调强放疗计划,对每次按照实验设计植入了标志物的盆腔假体分别进行25次照射,单次剂量约为60 Gy,在每个控制点获取兆伏级电子射野影像平片。(3)利用兆伏级平片和自研算法计算每种坐标组合25次照射的可探测性分数的均值( $\overline{D}$ ),并寻找最佳植入位置。通过曲线拟合分析计算普适情况下最佳植入位置参数值a和b。结果 组级结果:在所有组级坐标组合中,B模式下B10-Ⅰ组[(10,3,0)、(−10,3,0)、(10,−3,0)、(−10,−3,0),单位:mm]的 $\overline{D}$ 最高(0.2652分)。模式级结果:在所有模式中,D模式[(0,3b,0)、(a,b,a)、(−a,−b,−a)、(0,−3b,0),a、b均为参数,单位:mm]下的$\overline{D}$ 的平均值最高(0.2489分)。系统化结果:当a=9.6 mm、b=4.6 mm时,4种模式下所有坐标组合的$\overline{D}$ 均较为理想。结论 成功量化了植入标志物的可探测性并获取了由组级到模式级再到系统化的最佳植入位置。 Abstract:Objective To quantify the detectability of implanted markers in volume-modulated arc therapy for prostate cancer and to identify the best implant location. Methods (1) Markers were implanted with different fixed coordinate combinations in pelvic prostheses in proper order under four modes. (2) Twenty-five past volume-modulated arc therapy plans for prostate cancer were selected. In accordance with the experimental design, the pelvic prostheses implanted with the markers were irradiated for 25 times with single dose of about 60 Gy, and MV-level electronic portal image device images were obtained at each control point. (3) The mean value of detectability score ( ${ \overline{D}}$ ) of the implanted markers in each coordinate combination after 25 times of irradiation was calculated for every time point by using MV-level images and a self-developed algorithm to identify the best implant location. The optimal implant location parameters a and b were calculated via curve-fitting analysis.Results Group-level results: Among all group-level coordinate combinations, the $ \overline{D}$ of group B10-Ⅰ ((10.0,3.0,0), (−10.0,3.0,0), (10.0,−3.0,0), (−10.0,−3.0,0); unit: mm) under mode B was the highest (0.2652). Mode-level results: Among all modes, the mean$\overline{D}$ of mode D ((0,3b,0), (a,b,a), (−a,b,−a), (0,−3b,0); a and b are parameters, unit: mm) was the highest (0.2489). System-level results: The$\overline{D}$ of all combinations under the four modes were ideal when a=9.6 mm and b=4.6 mm.Conclusion This study successfully quantified the detectability of implanted markers, and the best implant location from the group level to the model level and then to the system level was obtained. -
图 1 VMAT标志物植入中40个组级坐标组合25次照射的可探测性分数均值(
$ \overline{D} $ )按降序排列的结果Figure 1. The mean detectability score
$\overline{D} $ for 40 group-level coordinate combinations after 25 times of radiation in volume-modulated arc therapy marker implantation is arranged in descending order
图 2 VMAT标志物植入中40个组级坐标组合25次照射的可探测性分数均值(
$\overline{D} $ )按模式A~D排列的结果Figure 2. The mean detectability score
$ \overline{D}$ for 40 group-level coordinate combinations after 25 times of radiation volume-modulated arc therapy marker implantation is arranged in mode A−D order
图 3 VMAT标志物植入中植入坐标参数a值同可探测性分数均值(
${ \overline{D}} $ )的拟合曲线Figure 3. Fitting curve of the implantation coordinate parameter a and the mean detectability score
$\overline{D} $ in volume-modulated arc therapy marker implatation
图 4 VMAT标志物植入中植入坐标参数b值同可探测性分数均值(
$\overline{D}$ )的拟合曲线Figure 4. Fitting curve of the implantation coordinate parameter b and the mean detectability score
$\overline{D}$ in volume-modulated arc therapy marker implatation表 1 VMAT标志物植入的X-Z平面(Y=0)(模式A)下 4种组级坐标组合
Table 1. Four group-level coordinate combinations under marker implantation mode A on the X-Z plane (Y=0) in volume-modulated arc therapy
参数值 b=0 a=5 A5-Ⅰc a=5 A5-Ⅱd a=10 A10-Ⅲd a=15 A15-Ⅳd 注:c表示植入坐标为(−3a,0,0)、(−a,0,0)、(a,0,0)、(3a,0,0)时的组级坐标组合;d表示植入坐标为(a,0,a)、(−a,0,a)、(a,0,−a)、(−a,0,−a)时的组级坐标组合。每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如A5-Ⅰ坐标组合代入参数a=5和b=0后,得到A5-Ⅰ组4枚标志物坐标:(−15,0,0)、(−5,0,0)、(5,0,0)、(15,0,0),a和b单位为mm  下载: 导出CSV
下载: 导出CSV
表 4 VAMT标志物植入的分散植入(模式D)下12种组 级坐标组合(X,Y,Z≠0)
Table 4. Twelve group-level coordinate combinations under marker dispersed implantation mode D (X,Y,Z≠0) in volume- modulated arc therapy
参数值 b=1.0 b=3.0 b=5.0 b=6.7 a=5 D5-Ⅰ D5-Ⅱ D5-Ⅲ D5-Ⅳ a=10 D10-Ⅰ D10-Ⅱ D10-Ⅲ D10-Ⅳ a=15 D15-Ⅰ D15-Ⅱ D15-Ⅲ D15-Ⅳ 注:每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如D5-Ⅰ坐标组合代入参数a=5和b=1后,得到D5-Ⅰ组4枚标志物坐标:(0,3,0)、(5,1,5)、(−5,−1,−5)、(0,−3,0),a和b单位为mm
下载: 导出CSV
表 2 VMAT标志物植入的X-Y平面(Z=0)(模式B)下 12种组级坐标组合
Table 2. Twelve group-level coordinate combinations under marker implantation mode B on the X-Y plane (Z=0) in volume- modulated arc therapy
参数值 b=3 b=9 b=15 b=20 a=5 B5-Ⅰ B5-Ⅱ B5-Ⅲ B5-Ⅳ a=10 B10-Ⅰ B10-Ⅱ B10-Ⅲ B10-Ⅳ a=15 B15-Ⅰ B15-Ⅱ B15-Ⅲ B15-Ⅳ 注:每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如B5-Ⅰ坐标组合代入参数a=5和b=3后,得到B5-Ⅰ组4枚标志物坐标:(5,3,0)、(−5,3,0)、(5,−3,0)、(−5,−3,0),a和b单位为mm
下载: 导出CSV
表 3 VAMT标志物植入的斜植入(模式C)下12种组级 坐标组合(X,Y,Z≠0)
Table 3. Twelve group-level coordinate combinations under marker oblique implantation mode C (X,Y,Z≠0) in volume- modulated arc therapy
参数值 b=3 b=9 b=15 b=20 a=5 C5-Ⅰ C5-Ⅱ C5-Ⅲ C5-Ⅳ a=10 C10-Ⅰ C10-Ⅱ C10-Ⅲ C10-Ⅳ a=15 C15-Ⅰ C15-Ⅱ C15-Ⅲ C15-Ⅳ 注:每个坐标组合代入相应参数值a和b即为该组标志物坐标,例如C5-Ⅰ坐标组合代入参数a=5和b=3后,得到C5-Ⅰ组4枚标志物坐标:(5,3,5)、(−5,3,−5)、(5,−3,5)、(−5,−3,−5),a和b单位为mm
下载: 导出CSV
-
[1] 倪晓雷, 陈榕钦, 柏朋刚, 等. 图像引导下宫颈癌容积旋转调强放疗中膀胱和直肠实际受照剂量评估[J]. 中国医学物理学杂志, 2019, 36(2): 142−145. DOI: 10.3969/j.issn.1005-202X.2019.02.004.
Ni XL, Chen RQ, Bai PG, et al. Evaluation of actual doses to bladder and rectum during image-guided volumetric modulated arc therapy for cervical cancer[J]. Chin J Med Phys, 2019, 36(2): 142−145. DOI: 10.3969/j.issn.1005-202X.2019.02.004.[2] 邱健健, 吕博, 黄莹, 等. 基于容积旋转弧形调强放疗技术的肝癌立体定向放疗方案评估与位置误差分析[J]. 中华放射医学与防护杂志, 2017, 37(2): 143−148. DOI: 10.3760/cma.j.issn.0254-5098.2017.02.011.
Qiu JJ, Lyu B, Huang Y, et al. The feasibility of breath control management guided stereotactic ablation body radiotherapy of liver tumors by volumetric modulated arc therapy[J]. Chin J Radiol Med Prot, 2017, 37(2): 143−148. DOI: 10.3760/cma.j.issn.0254-5098.2017.02.011.[3] 田龙, 席强, 赵鑫, 等. 膀胱癌图像引导放疗中基于骨骼与基于内植标记物锥形束CT校准比较[J]. 中国医学物理学杂志, 2019, 36(6): 647−652. DOI: 10.3969/j.issn.1005-202X.2019.06.006.
Tian L, Xi Q, Zhao X, et al. Comparison between CBCT calibrations based on skeleton vs implanted markers in image-guided radiotherapy for bladder cancer[J]. Chin J Med Phys, 2019, 36(6): 647−652. DOI: 10.3969/j.issn.1005-202X.2019.06.006.[4] 田龙, 席强, 赵鑫, 等. 膀胱癌图像引导放疗中基于软组织灰度值与基于内植标记物的锥形束CT校准比较[J]. 中国医学物理学杂志, 2018, 35(1): 31−35. DOI: 10.3969/j.issn.1005-202X.2018.01.007.
Tian L, Xi Q, Zhao X, et al. Comparison of cone beam computed tomography calibrations based on soft tissue grey value and implanted markers in image-guided radiotherapy for bladder cancer[J]. Chin J Med Phys, 2018, 35(1): 31−35. DOI: 10.3969/j.issn.1005-202X.2018.01.007.[5] 杨荃荃, 李志勇, 王娇. 锥形束CT与MSCT平扫在口腔检查中图像质量及辐射剂量的对比[J]. 中国CT和MRI杂志, 2020, 18(11): 50−52. DOI: 10.3969/j.issn.1672-5131.2020.11.016.
Yang QQ, Li ZY, Wang J. Comparison on image quality and radiation dose of cone beam computed tomography and MSCT for oral examination[J]. Chin J CT MRI, 2020, 18(11): 50−52. DOI: 10.3969/j.issn.1672-5131.2020.11.016.[6] 付娟, 孟慧鹏, 王克强, 等. 放射治疗千伏级图像引导系统的辐射剂量研究[J]. 医疗卫生装备, 2020, 41(2): 52−56. DOI: 10.19745/j.1003-8868.2020037.
Fu J, Meng HP, Wang KQ, et al. Study on radiation dose of kV image-guided system in radiotherapy[J]. Chin Med Equip J, 2020, 41(2): 52−56. DOI: 10.19745/j.1003-8868.2020037.[7] 李俊禹, 吴昊, 杨敬贤, 等. 基于品质因素评价瓦里安锥束CT成像质量与辐射剂量风险收益比[J]. 中华放射医学与防护杂志, 2020, 40(8): 595−599. DOI: 10.3760/cma.j.issn.0254-5098.2020.08.004.
Li JY, Wu H, Yang JX, et al. Evaluation of cost-effective ratio (imaging quality vs. radiation dose) of Varian cone beam CT based on figure of merit (FOM)[J]. Chin J Radiol Med Prot, 2020, 40(8): 595−599. DOI: 10.3760/cma.j.issn.0254-5098.2020.08.004.[8] 谢晓艳, 张祖燕, 王争, 等. 锥形束CT与螺旋CT应用于颞骨显像的辐射剂量分析[J]. 中华医学杂志, 2018, 98(23): 1837−1840. DOI: 10.3760/cma.j.issn.0376-2491.2018.23.006.
Xie XY, Zhang ZY, Wang Z, et al. Dosimetry of cone-beam computed tomography and multi-slice computed tomography scanning for temporal bone[J]. Nat Med J China, 2018, 98(23): 1837−1840. DOI: 10.3760/cma.j.issn.0376-2491.2018.23.006.[9] Inui S, Ueda Y, Ono S, et al. Evaluation of two-dimensional electronic portal imaging device using integrated images during volumetric modulated arc therapy for prostate cancer[J]. Rep Pract Oncol Radiother, 2021, 26(2): 281−290. DOI: 10.5603/RPOR.a2021.0041. [10] Osman SOS, Russell E, King R B, et al. Fiducial markers visibility and artefacts in prostate cancer radiotherapy multi-modality imaging[J/OL]. Radiat Oncol, 2019, 14(1): 237[2021-02-22]. https://ro-journal.biomedcentral.com/articles/10.1186/s13014-019-1447-1. DOI: 10.1186/s13014-019-1447-1. [11] Ghaffari H, Navaser M, Mofid B, et al. Fiducial markers in prostate cancer image-guided radiotherapy[J]. Med J Islam Repub Iran, 2019, 33: 15. DOI: 10.34171/mjiri.33.15. [12] 田龙, 席强, 赵鑫, 等. 前列腺癌图像引导放疗中两种引导方法摆位误差的比较[J]. 癌症进展, 2019, 17(5): 552−554, 588. DOI: 10.11877/j.issn.1672-1535.2019.17.05.14.
Tian L, Xi Q, Zhao X, et al. Comparison of setup error between two image-guided radiotherapy methods for prostate cancer[J]. Oncol Prog, 2019, 17(5): 552−554, 588. DOI: 10.11877/j.issn.1672-1535.2019.17.05.14.[13] 田龙, 李明辉, 胡逸民. 利用EPID图像金球位置自动跟踪算法研究[J]. 中国医学物理学杂志, 2014, 31(4): 5038−5042. DOI: 10.3969/j.issn.1005-202X.2014.04.014.
Tian L, Li MH, Hu YM. Study on automatically detecting the golden marker's position by using EPID images[J]. Chin J Med Phys, 2014, 31(4): 5038−5042. DOI: 10.3969/j.issn.1005-202X.2014.04.014.[14] Ma TJ, Kilian-Meneghin J, Kumaraswamy LK. Recommendation of fiducial marker implantation for better target tracking using MV imager in prostate radiotherapy[J]. J Appl Clin Med Phys, 2018, 19(5): 389−397. DOI: 10.1002/acm2.12390. [15] McNiven AL, Sharpe MB, Purdie TG. A new metric for assessing IMRT modulation complexity and plan deliverability[J]. Med Phys, 2010, 37(2): 505−515. DOI: 10.1118/1.3276775. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 5890
- HTML全文浏览量: 3983
- PDF下载量: 14

 '/>
'/>





 '/>
'/>



 '/>
'/>



 '/>
'/>
 '/>
'/>


 '/>
'/>



 '/>
'/>

 '/>
'/>

 '/>
'/>