


 下载:
下载:
-
骨血管瘤(intraosseous hemangioma,IH)是一种原发于骨的良性肿瘤,约占所有原发性骨肿瘤的1%,通常累及脊柱和颅骨,发生于长骨和扁平骨者较为少见[1-2]。目前,IH的发病机制仍不明确,临床表现缺乏特异性。IH发生于脊柱和颅骨时,其影像学表现较为典型;发生于长骨或扁平骨时,其影像学可成侵袭性或恶性肿瘤表现[3],容易造成误诊。我们报道了1例位于扁平骨的多发性IH,查阅文献并分析其18F-FDG PET/CT显像特点,旨在为临床鉴别诊断提供参考。
-
患者女性,57岁,因“体检时发现双侧肋骨病变20余天”于2020年4月26日至四川省肿瘤医院就诊。胸部CT影像显示,左侧第二肋骨、右侧第六肋骨膨胀性骨质破坏伴软组织密度影,性质不明确。患者无发热、盗汗、胸痛和呼吸困难等不适症状。既往无结核、外伤及恶性肿瘤等病史。实验室检查结果显示,血常规无明显异常,尿本周蛋白(BJP)为阴性,未见β2微球蛋白(β2-MG)水平升高,免疫球蛋白(immune globulin,Ig)G、IgA 和IgM 水平均未升高,未见碱性磷酸酶(ALP)水平升高,骨髓穿刺涂片和流式细胞学检查结果未见浆细胞异常增多,未见相关肿瘤标志物明显异常。
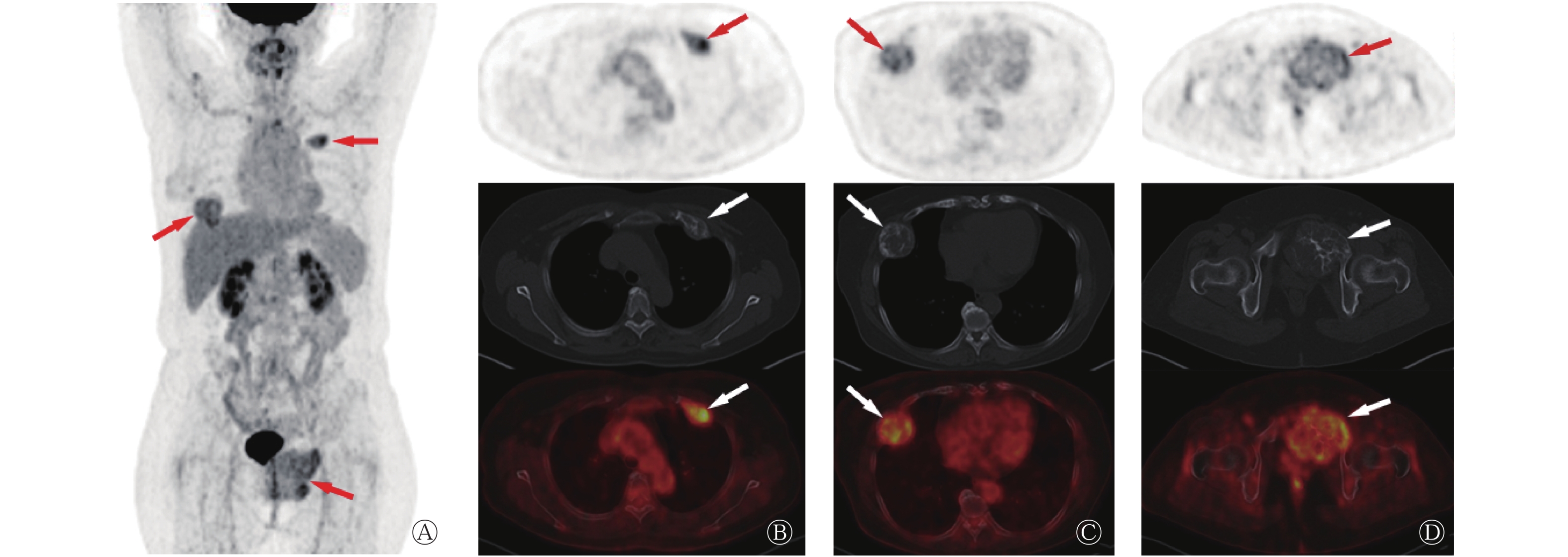
为明确骨病变的性质,对患者行全身18F-FDG PET/CT显像(图1A),结果显示,左侧第二肋骨前支、右侧第六肋骨前支和左侧耻骨膨胀性骨质破坏,边界清晰,内可见软组织密度影和粗细不一的骨样密度分隔影,边缘硬化,代谢不均匀升高(图1B~D);左侧第二肋骨前支病灶最大截面大小4.0 cm×2.4 cm,SUVmax=5.5;右侧第六肋骨前支病灶最大截面大小5.2 cm×4.6 cm,SUVmax=4.8;左侧耻骨病灶最大截面大小8.6 cm×7.2 cm,SUVmax=5.6。左侧耻骨病灶最大且位置表浅,遂行左侧耻骨病灶切开活检术。
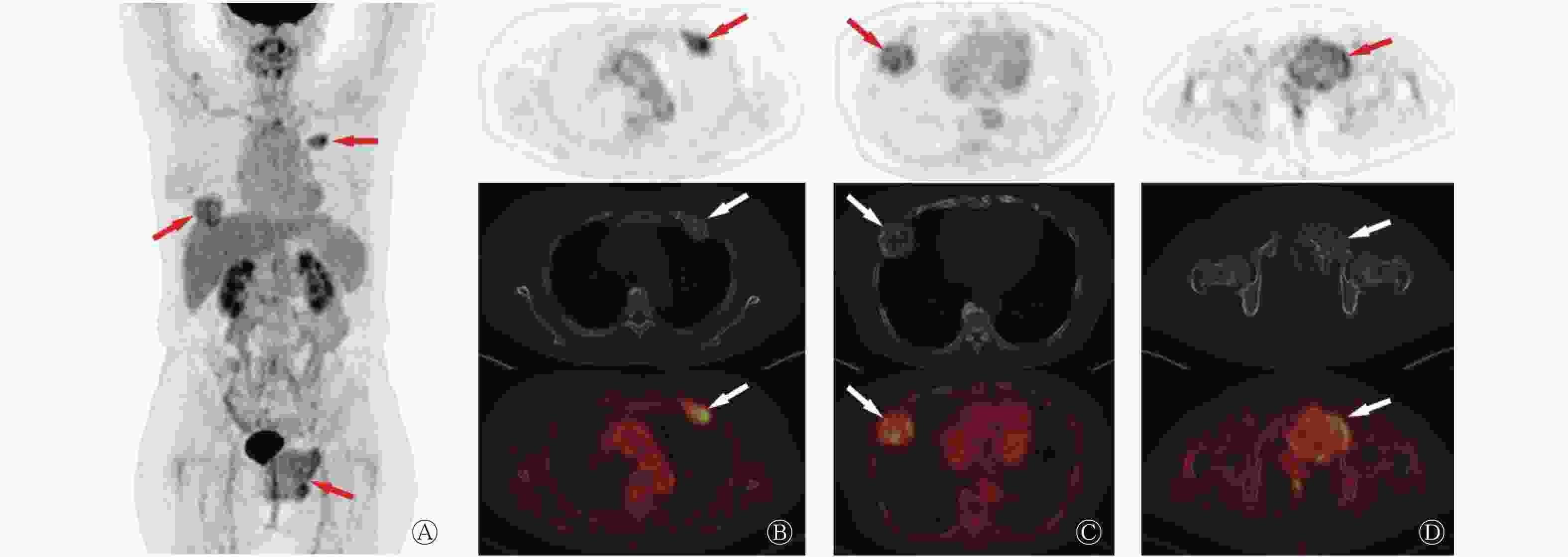
图 1 多发性骨血管瘤患者(女性,57岁)的18F-FDG PET/CT显像图
Figure 1. 18F-FDG PET/CT images of the patient (female, 57 years old) with multiple intraosseous hemangiomas
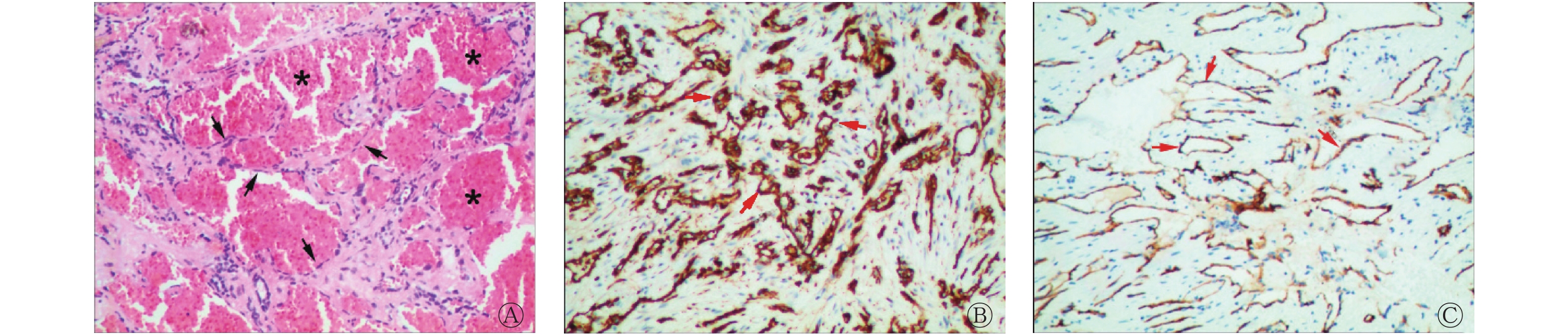
组织病理学检查结果显示,血管源性肿瘤以海绵状血管瘤为主,灶性区域为毛细血管瘤和动静脉瘤样结构,部分区域梭形细胞增生,肿瘤细胞异型性不大,未见复杂迷路或吻合(图2A)。免疫组织化学检查结果显示,细胞角蛋白19(CK19)(−)、细胞角蛋白(CK)(−)、甲状腺转录因子1(TTF-1)(−)、配对盒基因8抗原(PAX-8)(−)、E26转录因子相关基因(ERG)(+)、分化抗原簇31(CD31)(+)、分化抗原簇34(CD34)(+)、细胞增殖核抗原Ki-67(+,5%)(图2B~C)。结合患者的影像学表现,初步诊断为多发性IH,截至笔者投稿仍在随访中。
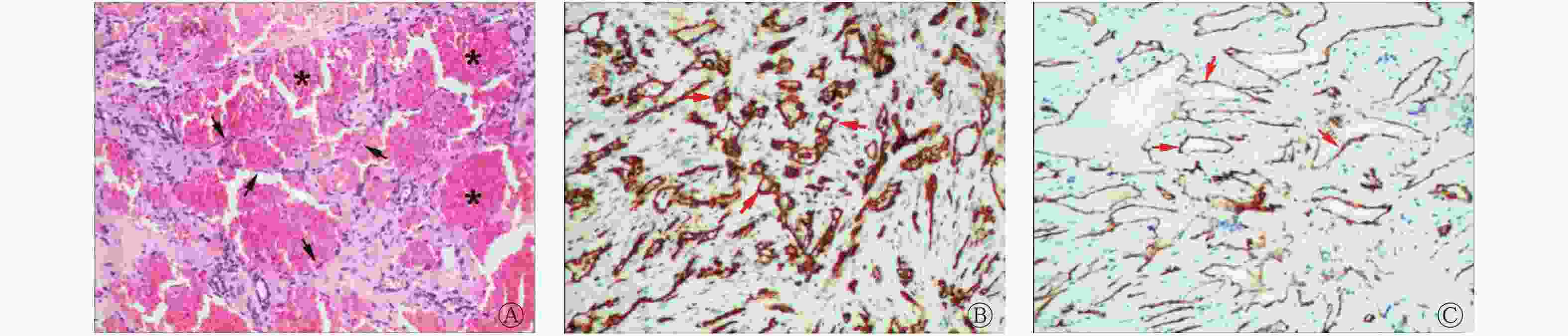
图 2 多发性骨血管瘤患者(女性,57岁)的组织病理学检查图(A,苏木精-伊红染色,×100)和免疫组织化学染色图(B、C,×100)
Figure 2. Histopathological and immunohistochemistry images of the patient (female, 57 years old) with multiple intraosseous hemangiomas
-
IH是一种良性的骨血管源性肿瘤,可在任何年龄段发生,最常见的累及部位是脊柱,其次是颅骨,常为单发,多发者少见[1,4-5]。IH在组织病理学上可分为海绵状型、毛细血管型、静脉血管型和混合型,临床上常无任何症状。发生于脊柱的患者,影像学表现较为典型,X射线图像常表现为“栅栏状”改变,CT横断面图像常表现为椎体网眼状或小蜂窝状改变,其内可见由残留的骨小梁形成的点状高密度影,由于肿瘤内存在脂肪,MRI的T1加权成像和T2加权成像均表现为较高信号,18F-FDG PET/CT常表现为无或低18F-FDG摄取[6];发生于扁平骨的患者,病灶可呈侵袭性或恶性肿瘤表现,为膨胀性或溶骨性骨质破坏,伴或不伴软组织形成,病灶内可见由骨小梁形成的粗细不均的分隔影,偶有钙化,边缘可有硬化,18F-FDG PET/CT表现为高18F-FDG摄取[3]。
IH因病变部位不同,可有多种影像学表现,导致手术前诊断困难。IH需要与以下疾病相鉴别:(1)骨转移瘤。骨转移瘤是骨骼系统发病率最高的恶性肿瘤,多见于中老年患者,男性常继发于前列腺癌,女性常继发于乳腺癌[7],常通过血行转移至脊柱,以胸、腰椎多见。临床症状主要表现为骨痛,部分患者可伴有病理性骨折、脊髓压迫等症状。实验室检查结果常显示血钙水平升高。影像学表现为成骨性、溶骨性和混合性骨质破坏,以溶骨性骨质破坏多见,伴或不伴软组织形成。18F-FDG PET/CT检查结合解剖和代谢信息,不仅能观察到病灶的形态学特点,还能反映其代谢情况,骨转移瘤在18F-FDG PET/CT上多表现为高代谢灶[8]。此外,部分患者可能为不明原发灶的骨转移瘤。因此,当患者的18F-FDG PET/CT显示全身多处骨质破坏,而未发现原发灶时,应警惕骨转移瘤的可能。(2)多发性骨髓瘤(multiple myeloma,MM)。MM好发于颅骨、脊柱、肋骨和骨盆等富含红骨髓的部位,临床表现多样,实验室检查结果常见血清单链IgG水平升高,确诊需要依据组织病理学检查结果。MM的CT表现为多发穿凿样或鼠咬状溶骨性骨质破坏,相互融合,累及肋骨时可表现为皂泡状或膨胀性骨质破坏,常见骨质疏松改变和并发病理性骨折,MRI图像呈典型“胡椒盐征”改变。18F-FDG PET/CT检查对MM具有较高的诊断价值,表现为局限于骨骼系统的多发溶骨性骨质破坏,骨质破坏累及范围广、数量多,其18F-FDG PET影像学表现具有一定的特异性,18F-FDG的代谢水平高低不等[9]。以上这些特点有助于MM的诊断和鉴别诊断。(3)骨纤维异常增殖症。该病好发于青少年,发生部位常见于四肢长骨、颅面骨和肋骨等。其典型CT表现为磨玻璃样改变,骨内膜呈“贝壳征”,周围有硬化边。18F-FDG PET/CT显示,不同患者的病灶的SUVmax具有较大的异质性,SUVmax为1.23~9.64[10],其原因可能是在骨组织重塑过程中,骨转换和成纤维细胞增殖的程度不同[11]。
多发性IH为少见肿瘤,本例患者影像学表现不同于常见的脊柱血管瘤,需要与上述相似疾病相鉴别。此外,由于骨良性血管源性肿瘤与骨恶性血管源性肿瘤在影像学和组织病理学表现上存在相似之处[12-13] ,本病例尚不能完全排除交界性或低度恶性血管源性肿瘤,治疗后需密切随访。18F-FDG PET/CT作为鉴别肿瘤良恶性的重要方法之一,在鉴别骨良、恶性血管源性肿瘤中的价值仍需要进一步研究探讨。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 李川负责论文的撰写、病例图片的整理与解析;姚玉唐负责诊断报告的终审、论文的修订;周星、彭小娟、江雪梅负责病例图片的获取、文献的收集与整理;游金辉负责研究命题的提出与理论指导;程祝忠负责研究命题的提出、论文的审核与最终版本的修订。
多发性骨血管瘤18F-FDG PET/CT显像一例
18F-FDG PET/CT imaging of multiple intraosseous hemangiomas : a case report
-
摘要: 笔者报道了1例多发性骨血管瘤(IH)18F-氟脱氧葡萄糖(FDG)PET/CT显像的病例,从临床症状、实验室检查和影像学表现等方面进行鉴别诊断。不同部位的IH的影像学表现各异,而18F-FDG PET/CT能为临床鉴别肿瘤的良恶性提供参考。由于发生于扁平骨的IH非常少见,且其影像学表现缺乏特异性,笔者通过对该病例的18F-FDG PET/CT显像特点进行分析,以期提高影像科医师对该病的认识。Abstract: A case of multiple intraosseous hemangioma (IH) with 18F-fluorodeoxyglucose (FDG) PET/CT imaging was reported, which was differentiated from the aspects of clinical symptoms, laboratory examinations and imaging findings. IH in different location have different imaging findings, and 18F-FDG PET/CT can provide a reference for clinical differentiation of benign and malignant tumors. As it was rare to find IH in flat bones, whose imaging findings were lack of specificity, the authors analyzed the 18F-FDG PET/CT imaging characteristics in order to improve the understanding of imaging physicians about the disease.
-
Key words:
-
图 1 多发性骨血管瘤患者(女性,57岁)的18F-FDG PET/CT显像图
Figure 1. 18F-FDG PET/CT images of the patient (female, 57 years old) with multiple intraosseous hemangiomas
-
[1] Leong S, Kok HK, Delaney H, et al. The radiologic diagnosis and treatment of typical and atypical bone hemangiomas: current status[J]. Can Assoc Radiol J, 2016, 67(1): 2−11. DOI: 10.1016/j.carj.2014.07.002. [2] Morkan DB, Gauthier JM, Kreisel D, et al. Incidentally found rib hemangioma: case report and discussion of management[J/OL]. AME Case Rep, 2021, 5: 13[2020-12-07]. https://acr.amegroups.com/article/view/6325/html. DOI: 10.21037/acr-20-144. [3] Matsumoto Y, Takahashi Y, Haraguchi A, et al. Intraosseous hemangioma arising in the clavicle[J]. Skeletal Radiol, 2014, 43(1): 89−93. DOI: 10.1007/s00256-013-1715-3. [4] Yao K, Tang F, Min L, et al. Multifocal intraosseous hemangioma: a case report[J]. Medicine (Baltimore), 2019, 98(2): e14001. DOI: 10.1097/MD.0000000000014001. [5] Akiyama R, Suzuki J, Ito K, et al. Multiple intraosseous hemangiomas: uncommon location[J]. Intern Med, 2018, 57(2): 293−294. DOI: 10.2169/internalmedicine.9137-17. [6] Tian R, Su MG, Tian Y, et al. Dual-time point PET/CT with F-18 FDG for the differentiation of malignant and benign bone lesions[J]. Skeletal Radiol, 2009, 38(5): 451−458. DOI: 10.1007/s00256-008-0643-0. [7] Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity[J]. Clin Cancer Res, 2006, 12(Suppl 20): S6243−6249. DOI: 10.1158/1078-0432.CCR-06-0931. [8] 郑庆中, 苏洁敏, 李小玲, 等. 18F-FDG PET/CT显像对多发性骨髓瘤与骨转移瘤的鉴别诊断价值[J]. 中国实验血液学杂志, 2020, 28(4): 1267−1271. DOI: 10.19746/j.cnki.issn1009-2137.2020.04.031.
Zheng QZ, Su JM, Li XL, et al. Differential diagnostic value of 18F-FDG PET/CT imaging in multiple myeloma and bone metastases[J]. J Exp Hematol, 2020, 28(4): 1267−1271. DOI: 10.19746/j.cnki.issn1009-2137.2020.04.031.[9] 李现军, 李凤岐, 李桂芝, 等. 多发性骨髓瘤患者18F-FDG PET/CT显像分析[J]. 中华核医学与分子影像杂志, 2018, 38(12): 790−792. DOI: 10.3760/cma.j.issn.2095-2848.2018.12.004.
Li XJ, Li FQ, Li GZ, et al. Imaging analysis of 18F-FDG PET/CT in patients with multiple myeloma[J]. Chin J Nucl Med Mol Imaging, 2018, 38(12): 790−792. DOI: 10.3760/cma.j.issn.2095-2848.2018.12.004.[10] Su MG, Tian R, Fan QP, et al. Recognition of fibrous dysplasia of bone mimicking skeletal metastasis on 18F-FDG PET/CT imaging[J]. Skeletal Radiol, 2011, 40(3): 295−302. DOI: 10.1007/s00256-010-0999-9. [11] Strobel K, Bode B, Lardinois D, et al. PET-positive fibrous dysplasia-a potentially misleading incidental finding in a patient with intimal sarcoma of the pulmonary artery[J]. Skeletal Radiol, 2007, 36 (Suppl 1): S24−28. DOI: 10.1007/s00256-006-0152-y. [12] Errani C, Vanel D, Gambarotti M, et al. Vascular bone tumors: a proposal of a classification based on clinicopathological, radiographic and genetic features[J]. Skeletal Radiol, 2012, 41(12): 1495−1507. DOI: 10.1007/s00256-012-1510-6. [13] van IJzendoorn DGP, Bovée JVMG. Vascular tumors of bone: the evolvement of a classification based on molecular developments[J]. Surg Pathol Clin, 2017, 10(3): 621−635. DOI: 10.1016/j.path.2017.04.003. -

 点击查看大图
点击查看大图
图(2)
计量
- 文章访问数: 5806
- HTML全文浏览量: 4061
- PDF下载量: 27