


-
尽管DTC预后良好,然而一旦患者出现远处转移,其5年总生存率将降至50%[1]。DTC常见的远处转移部位为肺和骨,其中,骨转移对预后影响更显著。因此,早期发现DTC患者的骨转移有助于更好地对患者进行分期和预后评估,并指导临床选择合适的综合治疗方案。笔者报道了1例DTC切除术后多发骨转移的病例,其99Tcm-MDP全身骨显像(whole-body bone scan,WBS)结果呈阴性,而经131I治疗后全身显像(post-treatment whole body scan,Rx-WBS)结果呈阳性,现将其实验室检查结果、影像学特点及治疗经过报道如下。
-
患者女性,46岁,2015年9月因“发现颈部肿块3月余”于湖北省恩施市建始县人民医院行双侧甲状腺次全切除术,组织病理学检查结果为双侧甲状腺腺瘤伴左侧甲状腺囊性变;2018年6月行颈部CT,结果显示甲状腺内低密度结节伴钙化,随后行双侧残余甲状腺全切除术+右侧中央组淋巴结清扫术。组织病理学检查结果为右侧甲状腺乳头状癌Ⅱ级,淋巴管有浸润,切缘未见癌细胞;左侧甲状腺腺瘤,局部边缘组织见上皮细胞非典型增生。
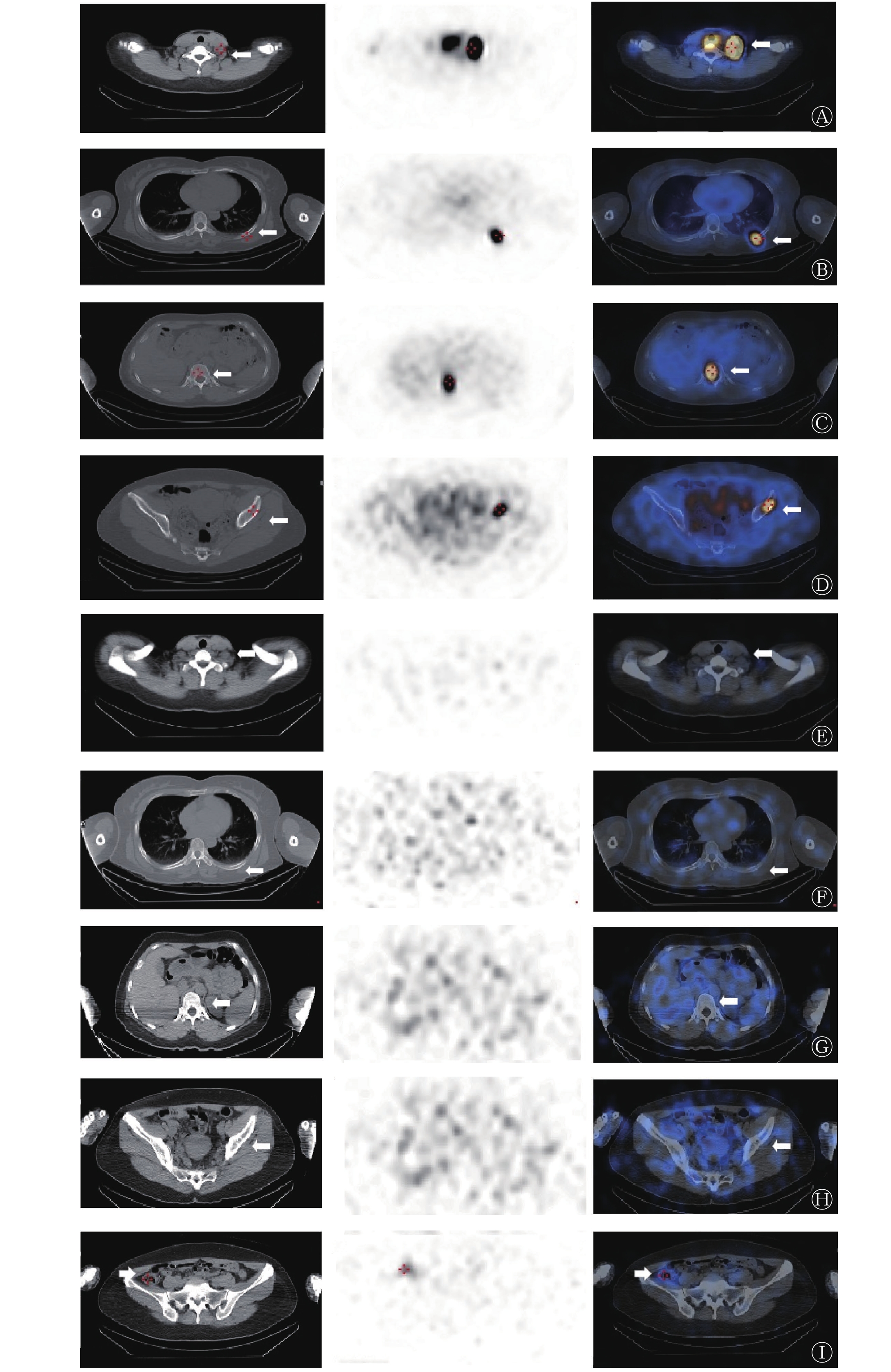
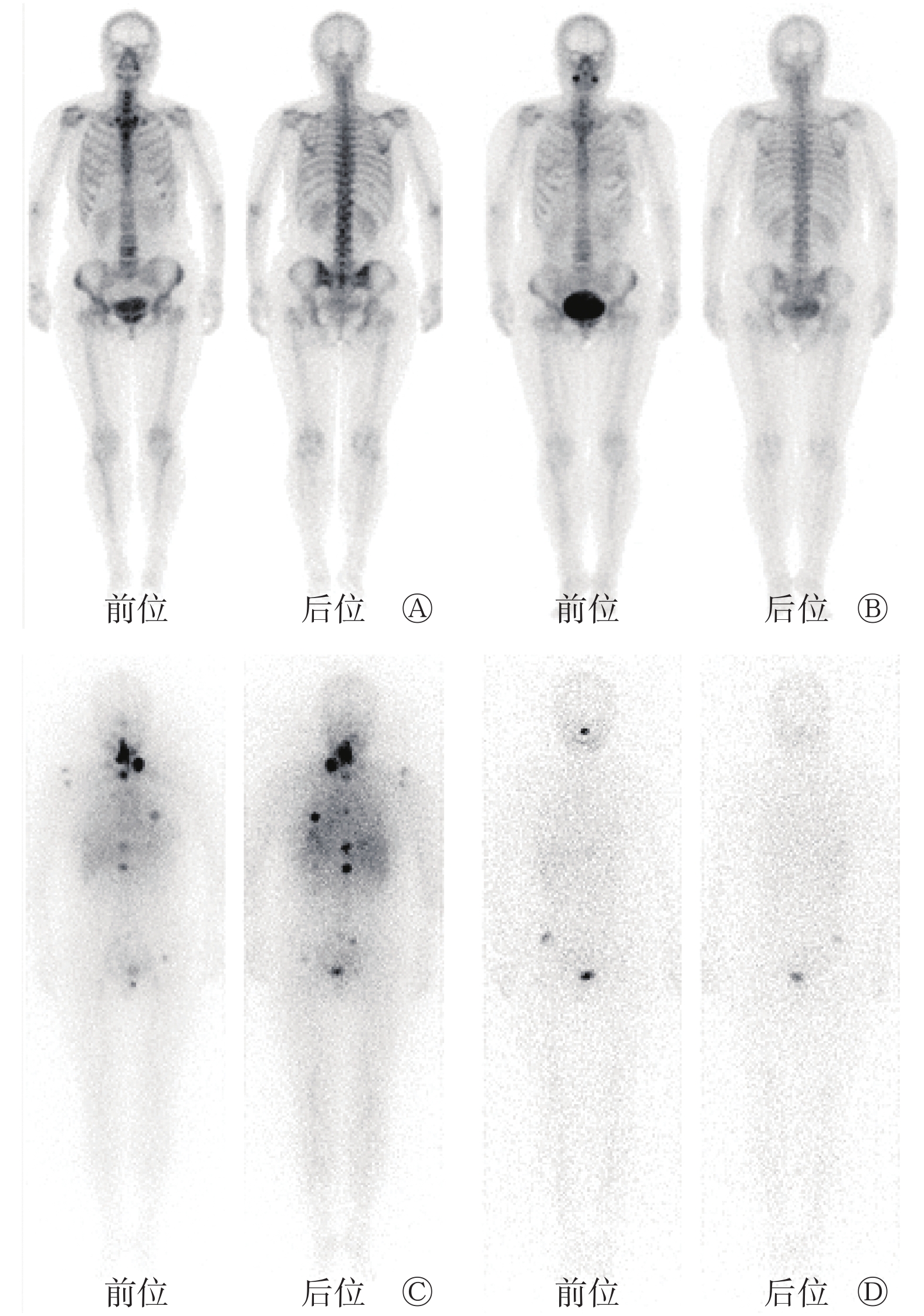
2018年7月,患者于华中科技大学同济医学院附属同济医院复查,其甲状腺球蛋白(thyroglobulin,Tg)水平为2.70 ng/mL,甲状腺球蛋白抗体(thyroglobulin antibody,TgAb)水平为36.50 U/mL(表1)。2019年1月于核医学科住院,拟行131I治疗,其血清游离T3(free T3,FT3)水平为1.75 pg/mL,血清游离T4(free T4,FT4)水平为0.37 ng/dL,促甲状腺激素(thyroid stimulating hormone,TSH)水平为72.58 μIU/mL,Tg水平为64.95 ng/mL,TgAb水平为66.80 U/mL(表1)。颈部超声结果显示,双侧甲状腺区异常低回声,考虑可能是术后导致的改变;可见左侧颈部淋巴结,考虑可能为异常淋巴结。行99Tcm-MDP WBS,结果未见明显异常(图1A)。综合患者的甲状腺功能、Tg和TgAb水平、颈部超声以及组织病理学检查结果,给予5.5×103 MBq的131I以在清甲的同时兼顾清灶治疗。5 d后行131I Rx-WBS(图1C)及局部SPECT/CT显像(图2A~D),结果显示左侧颈部V区淋巴结及全身多处骨组织多发摄碘灶;而CT结果显示,相应骨密度未见明显异常(图2),考虑为甲状腺癌术后伴左侧颈部V区淋巴结及多发骨转移。131I治疗后6周(2019年2月),患者的Tg水平为0.09 ng/mL、TgAb水平为155.60 U/mL;治疗后3个月(2019年4月),患者的Tg水平<0.04 ng/mL、TgAb水平为61.50 U/mL(表1)。2019年7月住院行第2次131I治疗,其TSH水平为73.95 μIU/mL,Tg水平为0.14 ng/mL,TgAb水平为21.97 U/mL(表1)。颈部超声结果未见明显异常。99Tcm-MDP WBS结果未见明显异常(图1B)。患者首次131I Rx-WBS结果提示淋巴结及多发骨转移,故第2次给予7.4×103 MBq的131I。5 d后行131I Rx-WBS(图1D)及局部SPECT/CT显像(图2E~I),131I Rx-WBS结果显示,原颈部及骨摄碘灶消失,肠道见生理性放射性浓聚,局部SPECT/CT显像结果与131I Rx-WBS结果一致。2019年9月和11月分别进行复查,Tg水平均<0.04 ng/mL,TgAb水平均<16.50 U/mL(表1),颈部超声结果均未见明显异常。
时间 血清游离T3
(pg/mL)血清游离T4
(ng/dL)促甲状腺激素(μIU/mL) 甲状腺球蛋白
(ng/mL)甲状腺球蛋白抗体(U/mL) 2018年7月 4.55 2.14 0.02 2.70 36.50 2019年1月 1.75 0.37 72.58 64.95 66.80 2019年2月 3.62 1.67 0.02 0.09 155.60 2019年4月 5.06 1.78 0.01 <0.04 61.50 2019年7月 <1.00 <0.40 73.95 0.14 21.97 2019年9月 3.37 1.31 0.63 <0.04 <16.50 2019年11月 4.07 1.67 0.01 <0.04 <16.50 正常参考值 2.00~4.10 0.80~2.00 0.55~4.78 1.40~78.00 0~60.00 注:T3为三碘甲腺原氨酸;T4为甲状腺素 表 1 分化型甲状腺癌切除术后多发骨转移患者(女性,46岁)2次行131I治疗前后的甲状腺功能结果
Table 1. Results of thyroid function of the patient with differentiated thyroid cancer with multiple bone metastases after resection (female, 46 years old) before and after 2 131I treatments
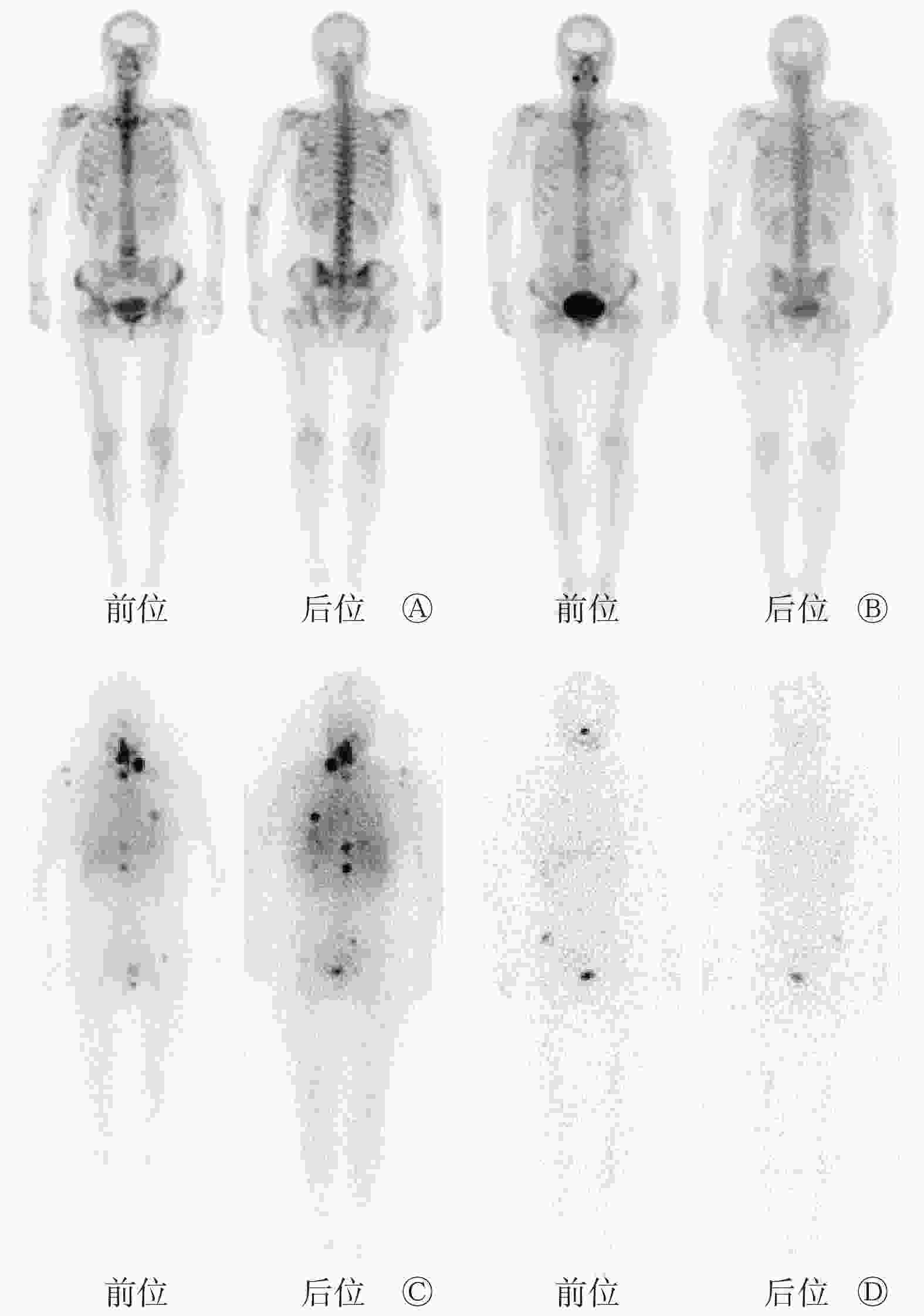
图 1 分化型甲状腺癌切除术后多发骨转移患者(女性,46岁)2次131I治疗前的99Tcm-MDP全身骨显像图和2次131I Rx-WBS图
Figure 1. 99Tcm-MDP whole-body bone scan images before twice 131I treatments and post-treatment whole body scan images after twice 131I treatments in patient with multiple bone metastases after resection of differentiated thyroid cancer (female, 46 years old)

图 2 分化型甲状腺癌切除术后多发骨转移患者(女性,46岁)2次131I治疗后的SPECT/CT显像图
Figure 2. SPECT/CT images after twice 131I treatment in the patient with multiple bone metastases after resection of differentiated thyroid cancer(female, 46 years old)
-
近年来的调查结果显示,DTC是发病率增长最快的恶性肿瘤之一,必须及时给予综合治疗[1]。尽管DTC预后良好,患者的10年总生存率为85%~93%,然而一旦患者出现远处转移,其5年总生存率将降至50%[1]。DTC常见的远处转移部位为肺和骨,其中肺转移占85%~93%,骨转移占20%~30%,两处皆有转移者占20%[2]。骨转移对DTC预后的影响更为显著,患者的10年总生存率进一步下降至13%~21%[3]。因此,早期发现DTC患者的骨转移有助于更好地对患者进行分期和预后评估,并指导临床医师选择合适的综合治疗方案。
DTC骨转移以溶骨性为主,少数为成骨性[4]。99Tcm-MDP WBS可显示局部骨血流灌注和骨盐代谢的情况,对诊断骨转移癌具有较高的灵敏度,且能比X射线和CT早3~6个月检出病灶,但体积小的溶骨性转移灶的99Tcm-MDP WBS结果可呈阴性,这是造成假阴性的原因之一。此外,受骨折和退行性病变的影响,99Tcm-MDP WBS诊断骨转移的假阳性率高、特异度低。由于大部分DTC转移灶均具有特异性摄取131I的特征,因此,131I WBS在诊断DTC骨转移方面具有重要意义,联合局部SPECT/CT显像可明显提高诊断的特异度和准确率,并有利于发现体积小、隐匿性的转移灶[5-6]。但是,131I WBS可显示不摄取131I的骨转移灶。有文献报道10%~15%的DTC患者会出现Tg阳性而131I WBS结果阴性的情况,主要原因可能是复发或转移的肿瘤细胞失分化、残留的肿瘤组织太少或病灶的体积太小而受仪器分辨率的限制无法探测到[7]。尽管DTC病灶具有分泌Tg的能力,然而其摄碘能力降低或丧失,导致131I WBS出现假阴性结果[7]。因此,99Tcm-MDP WBS、131I WBS及局部SPECT/CT联合应用可提高诊断的特异度和灵敏度。本病例第1次行131I Rx-WBS时探测到多发摄碘的骨转移灶,CT结果未见明显的骨密度异常,99Tcm-MDP WBS结果为阴性,可能是骨转移灶具备摄碘能力,但仍处于溶骨性病变的早期,尚未出现结构的改变,而99Tcm-MDP WBS探测溶骨性病变的灵敏度较低。
治疗后血清Tg水平是反映甲状腺癌转移程度的关键指标[8],但TgAb的存在会干扰Tg水平检测的准确率[9]。本病例在第1次131I治疗前TgAb水平升高,这提示存在分泌Tg的组织或病灶,即疾病处于持续或复发状态。第1次131I治疗后,患者的TgAb水平持续升高,这可能是因为131I的辐射生物学效应破坏了残留的甲状腺组织或肿瘤细胞,导致Tg释放入血,机体针对抗原Tg产生自身免疫性抗体[7]。第1次131I治疗前,患者的刺激性Tg水平为64.95 ng/mL,这提示有残余的DTC病灶或转移灶,通过2次131I治疗(总剂量为12.9×103 MBq)后,在接受甲状腺激素治疗的情况下,复查血清Tg及TgAb水平,二者分别降至<0.04 ng/mL、<16.50 U/mL,提示病情缓解,影像学检查结果显示转移灶消失。
一项针对131I治疗DTC患者的术后生存率分析的研究结果表明,经过131I治疗的DTC患者的10年总生存率为92.38%,其中,骨转移的DTC患者的10年总生存率为80.41%[10]。131I治疗可明显提高DTC患者术后的无复发生存率、无进展生存率和无疾病生存率[11]。对于骨转移灶的治疗,2014版《131I治疗分化型甲状腺癌指南》[12]指出,大部分患者经131I清灶治疗后病情稳定,部分患者的骨转移灶可减少或消失,虽然131I治疗很难治愈骨转移灶,但其可以缓解症状,提高患者的生活质量,并延长生存期,因此,摄碘骨转移灶应考虑行131I清灶治疗。本病例共经过2次131I治疗,第2次131I Rx-WBS结果为阴性,治疗后监测血清Tg水平持续<0.04 ng/mL,TgAb水平持续<16.50 U/mL,颈部超声结果无异常,提示转移灶消失,131I治疗效果显著。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 李丹负责病例资料的收集与整理、论文的撰写与修订;张冬灵负责病例资料的协助收集与整理;朱小华负责数据的分析、论文的审阅与最终版本的修订。
分化型甲状腺癌切除术后多发骨转移一例
Differentiated thyroid cancer with multiple bone metastases after resection: a case report
-
摘要: 笔者报道了1例分化型甲状腺癌(DTC)切除术后多发骨转移的病例,其99Tcm-亚甲基二膦酸盐全身骨显像结果呈阴性,而经131I治疗后全身显像(Rx-WBS)结果呈阳性,通过实验室检查、组织病理学检查及影像学检查结果综合分析了该病的特点。综合分析结果提示131I Rx-WBS有利于发现DTC骨转移灶,且131I治疗对其效果显著。Abstract: The authors reported a case of differentiated thyroid cancer (DTC) with multiple bone metastases after resection, whose 99Tcm-methylenediphosphonate whole-body bone scan was negative while 131I post-treatment whole body scan (Rx-WBS) was positive. This article clarified the characteristics of the disease from laboratory examinations, histopathological examinations and imaging examinations results. This case illustrated that 131I Rx-WBS was conducive to the discovery of DTC bone metastases, and 131I therapy has a significant effect.
-
Key words:
-
图 1 分化型甲状腺癌切除术后多发骨转移患者(女性,46岁)2次131I治疗前的99Tcm-MDP全身骨显像图和2次131I Rx-WBS图
Figure 1. 99Tcm-MDP whole-body bone scan images before twice 131I treatments and post-treatment whole body scan images after twice 131I treatments in patient with multiple bone metastases after resection of differentiated thyroid cancer (female, 46 years old)
图 2 分化型甲状腺癌切除术后多发骨转移患者(女性,46岁)2次131I治疗后的SPECT/CT显像图
Figure 2. SPECT/CT images after twice 131I treatment in the patient with multiple bone metastases after resection of differentiated thyroid cancer(female, 46 years old)
表 1 分化型甲状腺癌切除术后多发骨转移患者(女性,46岁)2次行131I治疗前后的甲状腺功能结果
Table 1. Results of thyroid function of the patient with differentiated thyroid cancer with multiple bone metastases after resection (female, 46 years old) before and after 2 131I treatments
时间 血清游离T3
(pg/mL)血清游离T4
(ng/dL)促甲状腺激素(μIU/mL) 甲状腺球蛋白
(ng/mL)甲状腺球蛋白抗体(U/mL) 2018年7月 4.55 2.14 0.02 2.70 36.50 2019年1月 1.75 0.37 72.58 64.95 66.80 2019年2月 3.62 1.67 0.02 0.09 155.60 2019年4月 5.06 1.78 0.01 <0.04 61.50 2019年7月 <1.00 <0.40 73.95 0.14 21.97 2019年9月 3.37 1.31 0.63 <0.04 <16.50 2019年11月 4.07 1.67 0.01 <0.04 <16.50 正常参考值 2.00~4.10 0.80~2.00 0.55~4.78 1.40~78.00 0~60.00 注:T3为三碘甲腺原氨酸;T4为甲状腺素  下载: 导出CSV
下载: 导出CSV
-
[1] Wen XZ, Wang B, Jin QM, et al. Thyroid antibody status is associated with central lymph node metastases in papillary thyroid carcinoma patients with Hashimoto's thyroiditis[J]. Ann Surg Oncol, 2019, 26(6): 1751−1758. DOI: 10.1245/s10434-019-07256-4. [2] Califano I, Deutsch S, Löwenstein A, et al. Outcomes of patients with bone metastases from differentiated thyroid cancer[J]. Arch Endocrinol Metab, 2018, 62(1): 14−20. DOI: 10.20945/2359-3997000000004. [3] Pal P, Singh B, Kane S, et al. Bone metastases in follicular carcinoma of thyroid[J]. Indian J Otolaryngol Head Neck Surg, 2018, 70(1): 10−14. DOI: 10.1007/s12070-017-1170-x. [4] Orita Y, Sugitani I, Toda K, et al. Zoledronic acid in the treatment of bone metastases from differentiated thyroid carcinoma[J]. Thyroid, 2011, 21(1): 31−35. DOI: 10.1089/thy.2010.0169. [5] Higashino M, Ayani Y, Terada T, et al. Clinical features of poorly differentiated thyroid papillary carcinoma[J]. Auris Nasus Larynx, 2019, 46(3): 437−442. DOI: 10.1016/j.anl.2018.10.001. [6] Lamartina L, Grani G, Durante C, et al. Recent advances in managing differentiated thyroid cancer[J/OL]. F1000Res, 2018, 7: 86[2020-09-26]. https://f1000research.com/articles/7-86/v1. DOI: 10.12688/f1000research.12811.1. [7] Maruoka Y, Abe K, Baba S, et al. Incremental diagnostic value of SPECT/CT with 131I scintigraphy after radioiodine therapy in patients with well-differentiated thyroid carcinoma[J]. Radiology, 2012, 265(3): 902−909. DOI: 10.1148/radiol.12112108. [8] Lin YS, Li TJ, Liang J, et al. Predictive value of preablation stimulated thyroglobulin and thyoglobulin/thyoid-stimulating hormone ratio in differetiated thyroid cancer[J]. Clin Nucl Med, 2011, 36(12): 1102−1105. DOI: 10.1097/RLU.0b013e3182291c65. [9] Spencer CA. Challenges of serum thyroglobulin (Tg) measurement in the presence of Tg autoantibodies[J]. J Clin Endocrinol Metab, 2004, 89(8): 3702−3704. DOI: 10.1210/jc.2004-0986. [10] 余永利, 罗全勇, 陈立波, 等. 分化型甲状腺癌术后131I治疗生存率分析[J]. 中华核医学杂志, 2006, 26(5): 261−263. DOI: 10.3760/cma.j.issn.2095-2848.2006.05.001.
Yu YL, Luo QY, Chen LB, et al. Survival of patients with differentiated thyroid carcinoma after thyroidectomy and 131I therapy[J]. Chin J Nucl Med, 2006, 26(5): 261−263. DOI: 10.3760/cma.j.issn.2095-2848.2006.05.001.[11] 慕转转, 刘杰蕊, 鲁涛, 等. 血清Tg用于远处转移性分化型甲状腺癌131I治疗的疗效评估[J]. 中华核医学与分子影像杂志, 2020, 40(6): 329−333. DOI: 10.3760/cma.j.cn321828-20200220-00055.
Mu ZZ, Liu JR, Lu T, et al. Serum thyroglobulin in evaluating the response to 131I treatment in patients with distant metastatic differentiated thyroid cancer[J]. Chin J Nucl Med Mol Imag, 2020, 40(6): 329−333. DOI: 10.3760/cma.j.cn321828-20200220-00055.[12] 中华医学会核医学分会. 131I治疗分化型甲状腺癌指南(2014版)[J]. 中华核医学与分子影像杂志, 2014, 34(4): 264−278. DOI: 10.3760/cma.j.issn.2095-2848.2014.04.002.
Chinese Society of Nuclear Medicine. Clinical guidelines for 131I therapy of differentiated thyroid cancer (2014 version)[J]. Chin J Nucl Med Mol Imaging, 2014, 34(4): 264−278. DOI: 10.3760/cma.j.issn.2095-2848.2014.04.002. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 4052
- HTML全文浏览量: 2868
- PDF下载量: 25