



-
胰腺和胆道结石是一种临床常见疾病,该疾病的致病因素较多,其中饮食习惯、长期炎症是最常见的病因,约占胰腺和胆道结石病的70% [1]。胰腺和胆道结石发病率较高,可引起腹部剧烈疼痛、黄疸和腹部感染等临床症状的发生,具有反复发作的特征,尽早诊断和及时治疗才可减轻其对患者生活质量的影响[2]。现阶段,胰腺和胆道结石常用的影像学诊断手段为胰胆管CT及磁共振胰胆管成像(magnetic resonance cholangiopancreatography,MRCP)等,但因成像特点不同,各种影像学诊断结果存在一定的差异,而目前临床上通常认为,与胰胆管CT比较,MRCP的诊断价值相对较高[3]。MRCP技术应用于胰腺和胆道结石的诊断,主要包括三维快速恢复快速自旋回波(three dimensional turbo spin echo retore,3D-TSERT)序列和可变翻转角的三维快速自旋回波(three dimensional sampling perfertion with application optimized contrasts using deifferent flip angle evolutions,3D-SPACE )序列扫描技术,其价值均在于MRCP对胆道结石的诊断得到了研究者的普遍认同[4-5]。但不同扫描序列的MRCP具有一定的差异,3D-TSERT和3D-SPACE序列这两种扫描技术是否存在互补性尚未见文献报道。鉴于此,本研究以确诊的胰腺和胆道结石患者为回顾性研究对象,评估3D-SPACE 联合3D-TSERT序列扫描技术在MRCP诊断结石中的价值。
-
选取2019年1月至9月于徐州市中心医院收治的胰腺和胆道结石患者进行回顾性研究。纳入标准[6]:(1)右上腹部绞痛伴发热、冷汗等临床症状,初步诊断为胰腺和胆道结石,但仍需进一步行影像学检查确诊; (2)未患有合并心肺等重要脏器功能障碍类疾病;(3)行外科取石手术,取出沙粒性结石;(4)对本研究知情并签署了知情同意书。排除标准:(1)依从性较差,临床资料不全;(2)妊娠期、哺乳期的女性。最终收集胰腺和胆道结石患者168例,其中男性93例、女性75例,年龄24~70(42.91±3.20)岁。本研究符合《赫尔辛基宣言》的原则。
-
采用德国西门子公司MRI扫描仪(型号:MAGNETOM Skyra 3.0T,配备6通道体线圈和6通道脊柱线阵列连接接收器)行腹部常规横断面T2压脂、T1加权扫描,定位胰腺和胆道,患者分别于自由呼吸状态下行3D-TSERT和3D-SPACE 序列的胰腺、胆道部位扫描,扫描位置以胆总管和胰管汇合处为中心,共旋转8次(每次约45°)投影模拟三维成像。3D-SPACE 序列扫描参数:视野 38 cm×38 cm、重复时间/回波时间(echo time,TE) 2 000 ms/629 ms、翻转角160°、层厚1.2 cm、层数80;回波数 106、矩阵279×384;体素1.0 mm×1.0 mm×1.1 mm;信噪比1.25;平均时长 133 s;加快因子2。3D-TSERT序列扫描参数:视野38 cm×38 cm、重复时间/TE 2 000 ms/622 ms;翻转角150°、层厚1.2 cm、层数 80;回波数 75;矩阵 275×320;体素 1.4 mm×1.2 mm×1.3 mm;信噪比 1.07;平均时长 284 s;加快因子 2。应用Syngo软件去除干扰影像,采用最大密度投影(MIP)技术处理原始图像,得到3D-SPACE和3D-TSERT序列胰胆管系统的磁共振图像。所有图像均由2名影像科副主任医师共同阅片,得出胰腺和胆道结石统一诊断,意见不统一时由主任医师进行最终判定。
-
以手术结果为诊断标准,计算3D-SPACE、3D-TSERT序列及其二者联合诊断结石的检出率,以及不同大小胰腺和胆道结石(≤0.8 cm结石,>0.8 cm结石)[7]、不同部位胰腺和胆道结石(胆囊结石、肝内胆管结石、胆总管结石、胆总管下端壶腹部结石、胰管结石)的检出率。分析3种扫描方法在MRCP诊断结石中的灵敏度、特异度和准确率,以ROC曲线最优临界值(最接近左上角点)的坐标值分别作为灵敏度、特异度,以ROC曲线的AUC作为准确率。
-
应用SPSS 22.0软件对数据进行统计学分析。胰腺和胆道结石的检出率及不同大小、不同部位胰腺和胆道结石的检出率等以百分比表示,2组间的比较采用χ2检验。差异标准α=0.05,P<0.05为差异有统计学意义。
-
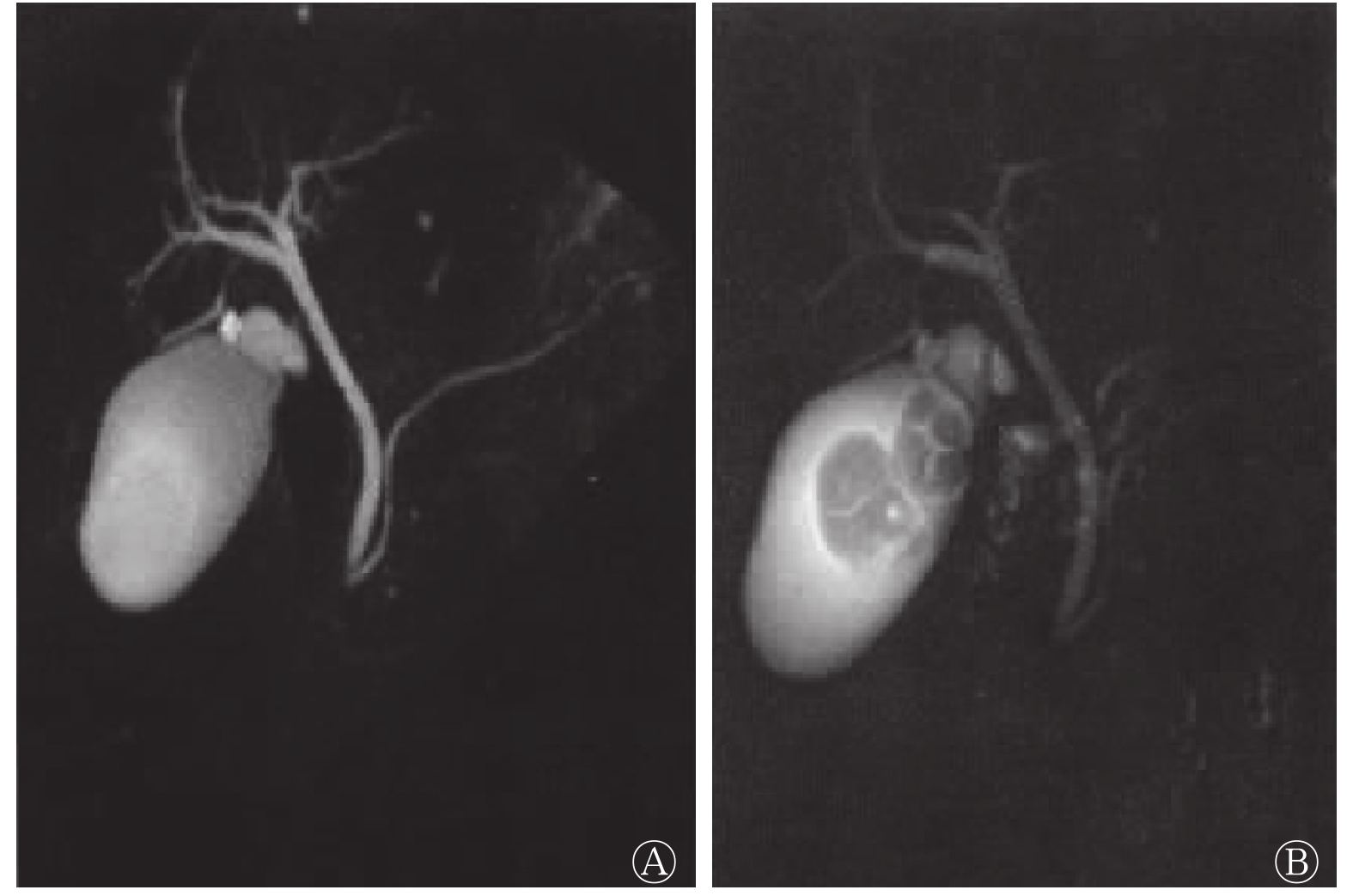
对全部患者行3D-SPACE联合3D-TSERT序列扫描结果发现,个别患者胆囊体积不同程度增大或缩小,胆囊壁增厚或无增厚,胆囊周围可见T2信号包绕或结节状T2信号(图1)。
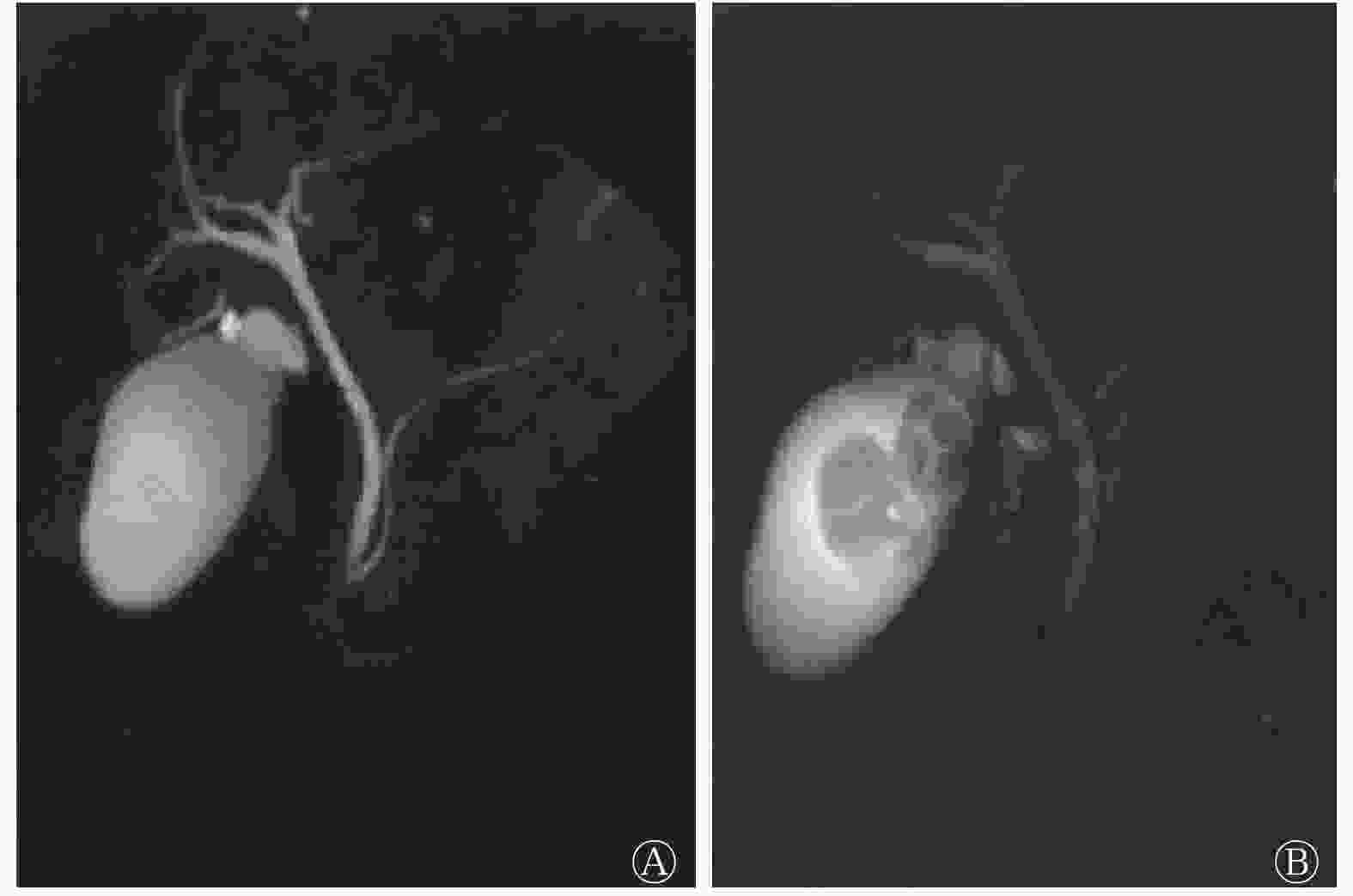
图 1 胆囊结石患者(女性,44岁)的磁共振胰胆管成像图 A为三维快速恢复快速自旋回波序列,未见胆囊结石;B为可变翻转角的三维快速自旋回波序列,清晰可见胆囊结石2颗,最大径分别为0.6 cm和0.7 cm
Figure 1. Magnetic resonance cholangiopancreatography of a patient with gallbladder calculi (female, 44 years old)
-
168例患者在手术中检出胰腺和胆道单发结石148例、双发或多发结石20例。手术中共检出结石194颗,以其为诊断标准,3D-SPACE序列检查共检出结石158颗,检出率为81.44%; 3D-TSERT序列检查共检出结石153颗,检出率为78.87% ;3D-SPACE联合3D-TSERT序列检查共检出结石191颗,检出率为98.45%。3D-SPACE 联合3D-TSERT序列的胰腺和胆道结石检出率高于3D-SPACE 、3D-TSERT序列(χ2=12.738、13.461,均P<0.01)。
-
手术中共检出胰腺和胆道结石194颗,其中最大径≤0.8 cm结石105颗、>0.8 cm结石89颗。3D-SPACE、3D-TSERT序列及其二者联合检查对最大径≤0.8 cm结石的检出率分别为69.52%(73/105)、66.67%(70/105)、97.14%(102/105),二者联合的检出率高于单独检查,且差异均有统计学意义(χ2=10.684、11.374,均P<0.01);对最大径>0.8 cm结石的检出率分别为95.51%(85/89)、93.26%(83/89)、100.00%(89/89) ,二者联合的检出率略高于单独检查,但差异均无统计学意义(χ2=0.684、0.457,均P>0.05)。
-
手术中共检出胰腺和胆道结石194颗,其中胆囊结石58颗、肝内胆管结石36颗、胆总管结石44颗、胆总管下端壶腹部结石30颗、胰管结石26颗。由表1可知,3D-SPACE联合3D-TSERT序列检查对不同部位的胰腺和胆道结石的检出率均高于单独检查,且差异均有统计学意义(χ2=9.105~15.715,均P<0.01)。
扫描方法 胆囊结石 肝内胆管结石 胆总管结石 胆总管下端壶腹部结石 胰管结石 3D-SPACE序列 82.76(48/58)a 83.33(30/36)a 84.09(37/44)a 76.67(23/30)a 76.92(20/26)a 3D-TSERT序列 81.03(47/58)a 77.78(28/36)a 77.27(34/44)a 80.00(24/30)a 76.92(20/26)a 3D-SPACE 联合3D-TSERT序列 100(58/58) 97.22(35/36) 100(44/44) 96.67(29/30) 96.15(25/26) 注:a表示与3D-SPACE联合3D-TSERT序列比较,差异均有统计学意义(χ2=9.105~15.715,均P<0.01)。MRCP为磁共振胰胆管成像;3D-SPACE为可变翻转角的三维快速自旋回波;3D-TSERT为三维快速恢复快速自旋回波 表 1 MRCP的不同扫描方法对不同部位的胰腺和胆道结石的检出率(%)
Table 1. The detection rate of different scanning methods of magnetic resonance cholangiopancreatography for different parts of pancreas and biliary tract calculi (%)
-
ROC曲线结果显示,3D-SPACE序列诊断胰腺和胆道结石的灵敏度、特异度和准确率分别为78.46%、79.68%和79.38%,95%CI:0.718~0.884;3D-TSERT序列诊断胰腺和胆道结石的灵敏度、特异度和准确率分别为77.53% 、78.62%和76.19%,95%CI:0.704~0.862;3D-SPACE 联合3D-TSERT序列诊断胰腺和胆道结石的灵敏度、特异度和准确率分别为89.73%、90.64%和88.26%,95% CI:0.846~0.943(图2)。3D-SPACE 联合3D-TSERT序列诊断胰腺和胆道结石的灵敏度、特异度、准确率均高于3D-SPACE、3D-TSERT序列。
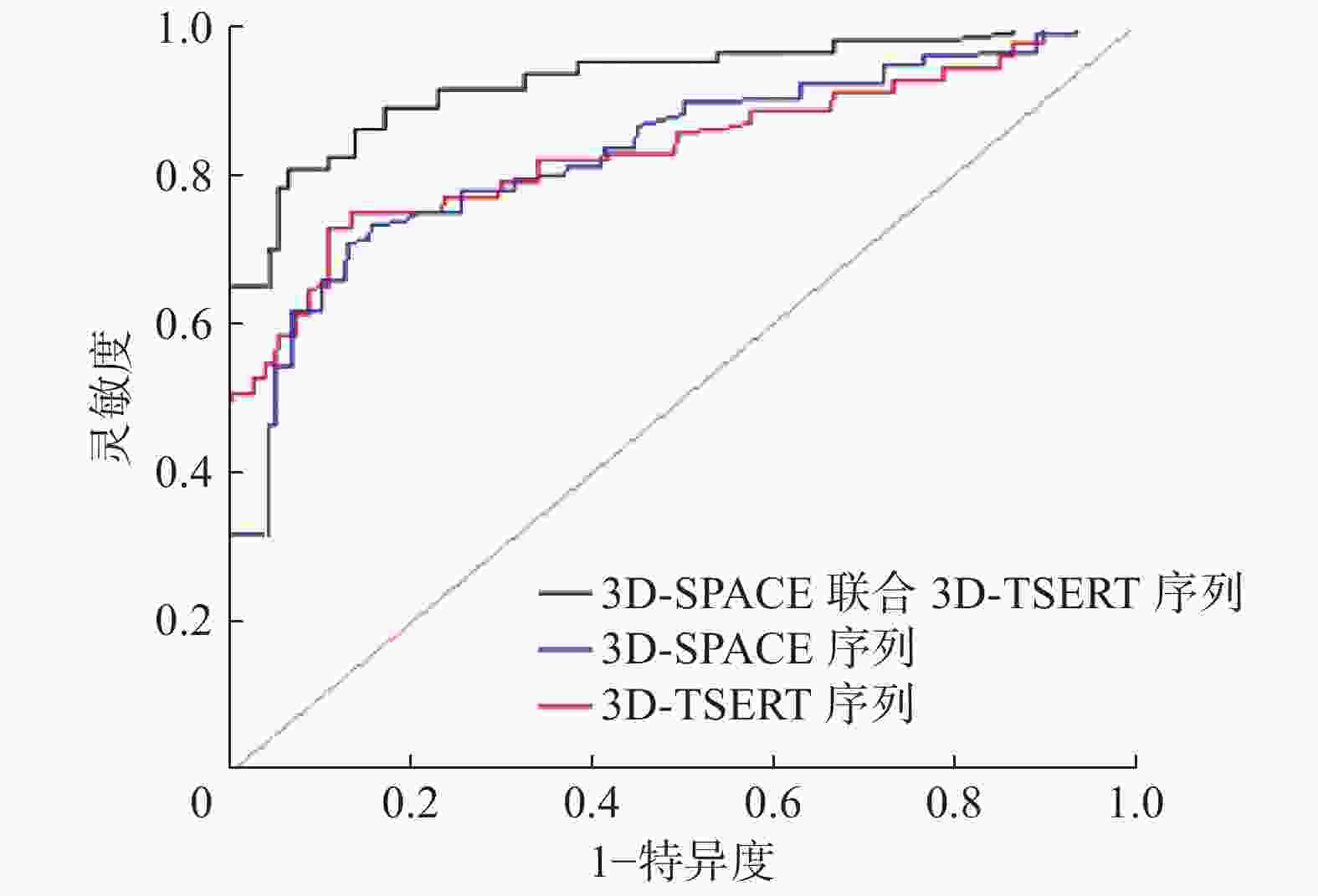
图 2 MRCP的不同扫描方法诊断胰腺和胆道结石效能的受试者工作特征曲线
Figure 2. Receiver operating characteristic curve of the effectiveness of different scanning methods of magnetic resonance cholangiopancreatography in diagnosing pancreatic and biliary tract calculi
-
胰腺和胆道结石是发展中国家的常见疾病,发病率约为3%~6%,多是由于饮食习惯、长期炎症等原因导致[8]。一般来说,单纯胰腺和胆道结石不会引起剧烈疼痛,但若结石从胆囊转移至胆总管,则可能引起剧烈疼痛或阵痛,给患者生活质量带来影响,甚至威胁患者的生命安全[9]。研究结果显示,12%~20%的胰腺和胆道结石患者伴有胆总管结石,且约2%~4%胰腺和胆道结石伴有胆总管结石可导致患者死亡,因此尽早诊断治疗具有重要的临床意义[10-11]。目前,临床诊断胰腺和胆道结石的影像学方法较多,包括超声、CT、MRI等,其中超声和CT虽有方便易行的优势,但极易受腹腔内气体、造影剂等多种因素干扰,导致诊断有一定的误差[12]。MRI是目前临床应用最多的诊断胰腺和胆道结石影像学技术,可在短时间内进行胰胆部位大范围薄层扫描,可清晰显示胰胆解剖结构及病理状态,但由于胰胆部位解剖结构较为复杂,单纯二维成像技术难以完整显示胰腺及胆囊结构,极易发生胰胆管结石的误诊和漏诊[13]。
-
MRCP技术是一种利用水的长波特征,采用长回波时间T2加权技术使水样结构保持较大横向磁化矢量,从而显影成像[14]。众所周知,人体内各组织结构均有特定的T2值,可根据TE长短决定T2值,当TE高于T2值时,组织结构可呈现低信号,当TE低于T2值时,组织结构可呈现高信号。因此,应用MRCP技术时,肝脏、脾脏、胰腺等组织表现为低信号,快速流动液体在流空效应下表现为信号缺失,而结石则表现为高信号[15]。基于上述原理,MRCP技术可在不应用外源性对比剂的情况下诊断胰腺和胆道结石,而该手段已经成为临床诊断胰腺和胆囊结石的首选方法。目前,MRCP扫描序列主要包括3D-TSERT序列和3D-SPACE序列 ,这2种序列扫描技术均基于MRCP原理,但在MRCP中却有一定的差异。3D-TSERT序列是一种基于快速回波序列的衍生技术,可在一次90°脉冲后,利用多个180°聚焦脉冲产生自旋回波,将横向磁化矢量重聚,从而进行MRCP[16]。3D-SPACE序列是一种基于3D-TSERT序列技术的变异,别称为“魔方成像”,传统3D-TSERT序列技术的重聚回波翻转角是恒定的,但3D-SPACE序列对回聚脉冲进行了翻转角设计,因可多角度成像被称为“魔方成像”,因此该技术在成像效果方面具有更佳的效果[17]。归纳来说,3D-TSERT序列和3D-SPACE序列各具优缺点,主要表现:(1)与3D-TSERT序列相比,3D-SPACE序列可获得更佳的MRCP对比度;(2)与3D-SPACE序列相比,3D-TSERT序列可使组织宏观纵向磁化矢量恢复,在保持较高图像质量的同时,缩短成像时间;(3)与3D-TSERT序列相比,由于3D-SPACE序列采用可变翻转角的回波链采集技术,不但可减少扫描时间,在克服T2值衰减和避免长回波链模糊效应方面同时具有较大的优势;(4)虽然3D-TSERT序列采用硬脉冲作为回聚脉冲,但与3D-SPACE序列相比,其具有回波间隔较短的特点,故可采集出更多的成像信息[18-19]。
-
从3D-TSERT和3D-SPACE 序列扫描技术的优缺点来看,3D-TSERT序列扫描具有成像时间较短、成像信息全面的优点,可避免3D-SPACE 序列扫描成像时间较长、成像信息单一的缺点,但3D-SPACE序列扫描成像具有对比度较高、长回波链模糊效应较弱的优点,可避免3D-TSERT序列扫描成像对比度较低和长回波链模糊效应较强的缺点,因此3D-TSERT联合3D-SPACE 序列应用可能提升3D-TSERT、3D-SPACE序列的MRCP诊断结石的准确率。本研究结果显示,3D-SPACE联合3D-TSERT序列对结石、不同部位胰腺和胆道结石的检出率均高于3D-SPACE、3D-TSERT序列;3D-SPACE、3D-TSERT序列及其二者联合对最大径>0.8 cm胰腺和胆道结石检出率的比较,差异无统计学意义,而3D-SPACE 联合3D-TSERT序列对最大径≤0.8 cm胰腺和胆道结石的检出率高于3D-SPACE、3D-TSERT序列,且差异有统计学意义。这提示,与3D-SPACE、3D-TSERT序列比较,3D-SPACE联合3D-TSERT序列扫描技术在不同部位MRCP对结石的诊断中有更高的检出率,尤其在微小结石的诊断中,具有更高的应用价值。另外,本研究ROC曲线分析结果也显示,3D-SPACE联合3D-TSERT序列在胰腺和胆道结石检测中的诊断灵敏度、特异度和准确度均高于3D-SPACE、3D-TSERT序列,这表明3D-SPACE联合3D-TSERT序列扫描技术可充分发挥3D-SPACE和3D-TSERT序列的优点,其缺点为扫描时间长,患者耐受性差。
综上所述,3D-TSERT和3D-SPACE序列扫描技术在MRCP成像中各具优缺点,与3D-SPACE、3D-TSERT序列比较,3D-SPACE联合3D-TSERT序列扫描技术在MRCP诊断胰腺和胆道结石中有更高的检出率,尤其对微小结石的检出率更高。因此,联合序列扫描技术在MRCP诊断结石中具有更佳的应用价值,值得临床推广应用。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 朱磊负责方法的建立、现场的试验、论文的撰写和审阅;张莉负责数据的收集与分析、现场的试验;孙梦晨负责数据的收集与整理。
3D-SPACE 联合3D-TSERT序列扫描技术在MRCP诊断结石中的价值
The value of 3D-SPACE combined with 3D-TSERT sequence scanning technology in MRCP diagnosis of calculi
-
摘要:
目的 评估可变翻转角的三维快速自旋回波(3D-SPACE)联合三维快速恢复快速自旋回波(3D-TSERT)序列扫描技术在磁共振胰胆管成像(MRCP)诊断结石中的价值。 方法 选取2019年1月至9月于徐州市中心医院确诊为胰腺和胆道结石的168例患者的临床资料进行回顾性研究,其中男性93例、女性75例,年龄24~70(42.91±3.20)岁。所有患者均行胰腺和胆道3D-SPACE和3D-TSERT序列的MRCP,以外科手术结果为诊断标准,分析并计算3D-SPACE、3D-TSERT序列及其二者联合对胰腺和胆道结石及不同大小、不同部位胰腺和胆道结石的检出率。采用ROC曲线分析3D-SPACE、3D-TSERT序列及其二者联合在MRCP对胰腺和胆道结石诊断中的灵敏度、特异度和准确率。2组间检出率的比较采用χ2检验。 结果 3D-SPACE联合3D-TSERT序列对胰腺和胆道结石的检出率(98.45%,191/194)高于3D-SPACE (81.44%,158/194)、3D-TSERT(78.87%,153/194)序列,且差异均有统计学意义(χ2=12.738、13.461,均P<0.01)。3D-SPACE联合3D-TSERT序列对最大径≤0.8 cm胰腺和胆道结石的检出率(97.14%,102/105)高于3D-SPACE (69.52%,73/105)、3D-TSERT(66.67%,70/105)序列,且差异均有统计学意义(χ2=10.684、11.374,均P<0.01)。3D-SPACE联合3D-TSERT序列对胆囊结石、肝内胆管结石、胆总管结石、胆总管下端壶腹部结石、胰管结石的检出率高于3D-SPACE、3D-TSERT 序列,且差异均有统计学意义(χ2=9.105~15.715,均P<0.01)。3D-SPACE联合3D-TSERT序列扫描技术对胰腺和胆道结石诊断的灵敏度、特异度和准确率分别为89.73%、90.64%和88.26%,高于3D-SPACE (78.46%、79.68%、79.38%)、3D-TSERT(77.53%、78.62%、76.19%)序列。 结论 3D-SPACE联合3D-TSERT序列扫描技术在MRCP中对不同部位胰腺和胆道结石(尤其微小结石)的诊断中具有很高的临床应用价值。 -
关键词:
- 磁共振成像 /
- 3D-SPACE 序列 /
- 3D-TSERT序列 /
- 结石 /
- 胰腺 /
- 胆道
Abstract:Objective To evaluate the value of variable flip angle three dimensional sampling perfertion with application optimized contrasts using deifferent flip angle evolutions (3D-SPACE) combined with three dimensional turbo spin echo retore (3D-TSERT) sequence scanning technology in the diagnosis of calculi using magnetic resonance cholangiopancreatography (MRCP). Methods A retrospective study was conducted on the clinical data of 168 patients diagnosed with pancreatic and biliary calculi in the Central Hospital of Xuzhou from January to September 2019. The patients comprised 93 males and 75 females, aged 24–70(42.91±3.20) years, who underwent pancreatic and biliary tract 3D-SPACE-sequence and 3D-TSERT-sequence MRCP. The surgical result was used as the diagnostic standard. 3D-SPACE-sequence, 3D-TSERT-sequence, and their combination were used to determine and analyze different sizes of calculi in the pancreas and biliary tract. The three methods were compared in terms of their detection rates of pancreatic and biliary tract calculi. Receiver operating characteristic curve was used to analyze the sensitivity, specificity, and accuracy of 3D-SPACE, 3D-TSERT sequence, and their combination in the diagnosis of pancreatic and biliary tract calculi in MRCP. χ2 test was used to compare the detection rates between the two groups. Result The detection rate of 3D-SPACE combined with 3D-TSERT sequence for pancreatic and biliary calculi (98.45%, 191/194) was higher than those of 3D-SPACE-sequence (81.44%, 158/194) and 3D-TSERT-sequence (78.87%, 153/194), and the difference was statistically significant (χ2=12.738, 13.461; both P<0.01). The detection rate of 3D-SPACE combined with 3D-TSERT sequence for pancreas and biliary tract calculi with maximum diameter ≤0.8 cm (97.14%, 102/105) was higher than those of 3D-SPACE-sequence (69.52%, 73/105) and 3D-TSERT-sequence (66.67%, 70/105), and the difference was statistically significant (χ2=10.684, 11.374; both P<0.01). The detection rates of 3D-SPACE combined with 3D-TSERT sequence for gallbladder calculi, intrahepatic bile duct calculi, common bile duct calculi, lower common bile duct ampullary calculi, and pancreatic duct calculi were higher than those of 3D-SPACE-sequence and 3D-TSERT-sequence, and the differences were statistically significant (χ2=9.105–15.715, all P<0.01). The sensitivity, specificity, and accuracy of 3D-SPACE combined with 3D-TSERT sequence for the diagnosis of pancreatic and biliary calculi were 89.73%, 90.64%, and 88.26%, respectively, which were higher than those of 3D-SPACE-sequence (78.46%, 79.68%, and 79.38%) and 3D-TSERT-sequence (77.53%, 78.62%, and 76.19%). Conclusion 3D-SPACE combined with 3D-TSERT sequence scanning technology has high clinical application value in the diagnosis of calculi (especially small calculi) through the MRCP of different parts of the pancreas and biliary tract. -
Key words:
- Magnetic resonance imaging /
- 3D-SPACE sequence /
- 3D-TSERT sequence /
- Calculi /
- Pancreas /
- Biliary tract
-
图 1 胆囊结石患者(女性,44岁)的磁共振胰胆管成像图 A为三维快速恢复快速自旋回波序列,未见胆囊结石;B为可变翻转角的三维快速自旋回波序列,清晰可见胆囊结石2颗,最大径分别为0.6 cm和0.7 cm
Figure 1. Magnetic resonance cholangiopancreatography of a patient with gallbladder calculi (female, 44 years old)
图 2 MRCP的不同扫描方法诊断胰腺和胆道结石效能的受试者工作特征曲线
Figure 2. Receiver operating characteristic curve of the effectiveness of different scanning methods of magnetic resonance cholangiopancreatography in diagnosing pancreatic and biliary tract calculi
表 1 MRCP的不同扫描方法对不同部位的胰腺和胆道结石的检出率(%)
Table 1. The detection rate of different scanning methods of magnetic resonance cholangiopancreatography for different parts of pancreas and biliary tract calculi (%)
扫描方法 胆囊结石 肝内胆管结石 胆总管结石 胆总管下端壶腹部结石 胰管结石 3D-SPACE序列 82.76(48/58)a 83.33(30/36)a 84.09(37/44)a 76.67(23/30)a 76.92(20/26)a 3D-TSERT序列 81.03(47/58)a 77.78(28/36)a 77.27(34/44)a 80.00(24/30)a 76.92(20/26)a 3D-SPACE 联合3D-TSERT序列 100(58/58) 97.22(35/36) 100(44/44) 96.67(29/30) 96.15(25/26) 注:a表示与3D-SPACE联合3D-TSERT序列比较,差异均有统计学意义(χ2=9.105~15.715,均P<0.01)。MRCP为磁共振胰胆管成像;3D-SPACE为可变翻转角的三维快速自旋回波;3D-TSERT为三维快速恢复快速自旋回波  下载: 导出CSV
下载: 导出CSV
-
[1] 李勇, 孙登群, 范育林, 等. 1268例胆总管结石治疗体会[J]. 中华灾害救援医学, 2019, 7(10): 586−588. DOI: 10.13919/j.issn.2095-6274.2019.10.013.
Li Y, Sun DQ, Fan YL, et al. Experience in the treatment of 1268 cases of common bile duct stones[J]. Chin J Disaster Med, 2019, 7(10): 586−588. DOI: 10.13919/j.issn.2095-6274.2019.10.013.[2] 刘雪娇, 贾红波. 毕Ⅱ式胃切除术后内镜逆行性胰胆管造影的应用及安全性分析[J]. 中华普通外科学文献(电子版), 2020, 14(2): 118−120. DOI: 10.3877/cma.j.issn.1674-0793.2020.02.010.
Liu XJ, Jia HB. Application and safety of endoscopic retrograde cholangiopancreatography after Billroth Ⅱ gastrectomy[J]. Chin Arch Gen Surg: Electron Ed, 2020, 14(2): 118−120. DOI: 10.3877/cma.j.issn.1674-0793.2020.02.010.[3] Muhammedoğlu B, Kale IT. Comparison of the safety and efficacy of single-stage endoscopic retrograde cholangiopancreatography plus laparoscopic cholecystectomy versus two-stage ERCP followed by laparoscopic cholecystectomy six-to-eight weeks later: a randomized controlled trial[J]. Int J Surg, 2020, 76: 37−44. DOI: 10.1016/j.ijsu.2020.02.021. [4] 郑恩双, 薛蕴菁, 孙斌, 等. 单次屏气3D-SPACE序列MR胰胆管成像技术的可行性初探[J]. 中华放射学杂志, 2020, 54(8): 799−803. DOI: 10.3760/cma.j.cn112149-20190921-00438.
Zheng ES, Xue YJ, Sun B, et al. Feasibility of single breath holding 3D-SPACE MR cholangiopancreatography: a preliminary study[J]. Chin J Radiol, 2020, 54(8): 799−803. DOI: 10.3760/cma.j.cn112149-20190921-00438.[5] Keus F, Gooszen HG, Van Laarhoven CJ. Open, small-incision, or laparoscopic cholecystectomy for patients with symptomatic cholecystolithiasis. An overview of Cochrane Hepato-Biliary Group reviews[J/OL]. Cochrane Database Syst Rev, 2010, 2010(1): CD008318[2020-09-14]. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD008318/full. DOI: 10.1002/14651858.CD008318. [6] Matsui Y, Hirooka S, Sakaguchi T, et al. Bile duct stones predict a requirement for cholecystectomy in older patients[J]. World J Surg, 2020, 44(3): 721−729. DOI: 10.1007/s00268-019-05241-2. [7] 练远书, 黄高, 陆开艺, 等. 两种手术方法对胆总管直径≥1.0 cm结石患者的疗效分析[J]. 中华普外科手术学杂志(电子版), 2020, 14(5): 530−533. DOI: 10.3877/cma.j.issn.1674-3946.2020.05.027.
Lian YS, Huang G, Lu KY, et al. A comparative study of LCBDE and LBEPS in the treatment of choledocholithiasis with ≥1.0 cm common bile duct diameter[J]. Chin J Oper Proc Gen Surg: Electron Ed, 2020, 14(5): 530−533. DOI: 10.3877/cma.j.issn.1674-3946.2020.05.027.[8] 张会来. 腹腔镜下胆囊切除术治疗胆囊结石的临床价值研究[J]. 内蒙古医学杂志, 2018, 50(9): 1074−1075. DOI: 10.16096/J.cnki.nmgyxzz.2018.50.09.029.
Zhang HL. Clinical value of laparoscopic cholecystectomy in the treatment of gallstones[J]. Inner Mongolia Med J, 2018, 50(9): 1074−1075. DOI: 10.16096/J.cnki.nmgyxzz.2018.50.09.029.[9] Portincasa P, Di Ciaula A, De Bari O, et al. Management of gallstones and its related complications[J]. Expert Rev Gastroenterol Hepatol, 2016, 10(1): 93−112. DOI: 10.1586/17474124.2016.1109445. [10] 施大伟, 沈娟. 磁共振多序列成像对胆总管下段结石的应用价值分析[J]. 齐齐哈尔医学院学报, 2015, 36(33): 5000−5002.
Shi DW, Shen J. Application value of multi-sequences MRI in the diagnosis of under choledoch stone[J]. J Qiqihar Univ Med, 2015, 36(33): 5000−5002.[11] 叶水平, 曹小娜. MRCP 2D FACE序列对胆道术后病变的诊断价值[J]. 当代医学, 2017, 23(28): 148−149. DOI: 10.3969/j.issn.1009-4393.2017.28.071.
Ye SP, Cao XN. The diagnostic value of MRCP 2D FACE sequence in postoperative biliary tract lesions[J]. Contemp Med, 2017, 23(28): 148−149. DOI: 10.3969/j.issn.1009-4393.2017.28.071.[12] He M, Xu J, Sun ZY, et al. Comparison and evaluation of the efficacy of compressed SENSE (CS) and gradient- and spin-echo (GRASE) in breath-hold (BH) magnetic resonance cholangiopancreatography (MRCP)[J]. J Magn Reson Imaging, 2020, 51(3): 824−832. DOI: 10.1002/jmri.26863. [13] Barros S, Gallego E, Lorente A, et al. Comparison of neutron and secondary gamma dose assessment using polygon mesh and voxel computational phantoms[J]. J Radiol Prot, 2020, 40(2): 583−595. DOI: 10.1088/1361-6498/ab7d8d. [14] Buell JF, Cronin DC, Funaki B, et al. Devastating and fatal complications associated with combined vascular and bile duct injuries during cholecystectomy[J]. Arch Surg, 2002, 137(6): 703−710. DOI: 10.1001/archsurg.137.6.703. [15] Kharga B, Sharma BK, Singh VK, et al. Obesity not necessary, risk of symptomatic cholelithiasis increases as a function of BMI[J]. J Clin Diagn Res, 2016, 10(10): PC28−PC32. DOI: 10.7860/JCDR/2016/22098.8736. [16] 吴晓军. CT与MRCP诊断胆道系统结石的影像学对比分析及应用价值评价[J]. 中国CT和MRI杂志, 2016, 14(12): 80−82. DOI: 10.3969/j.issn.1672-5131.2016.12.027.
Wu XJ. Contrast analysis and application value evaluation of CT and MRCP in the diagnosis of biliary calculi[J]. Chin J CT MRI, 2016, 14(12): 80−82. DOI: 10.3969/j.issn.1672-5131.2016.12.027.[17] 唐雨, 于加贝, 王翠, 等. 磁共振成像3D-STIR-SPACE序列对臂丛神经节后损伤的诊断价值[J]. 实用医学影像杂志, 2019, 20(1): 25−27. DOI: 10.16106/j.cnki.cn14-1281/r.2019.01.008.
Tang Y, Yu JB, Wang C, et al. The diagnostic value of MRI 3D-STIR-SPACE sequence in posterior brachial plexus nerve injury[J]. J Pract Med Imaging, 2019, 20(1): 25−27. DOI: 10.16106/j.cnki.cn14-1281/r.2019.01.008.[18] Gupta A, Rai P, Singh V, et al. Intrahepatic biliary duct branching patterns, cystic duct anomalies, and pancreas divisum in a tertiary referral center: a magnetic resonance cholangiopancreaticographic study[J]. Indian J Gastroenterol, 2016, 35(5): 379−384. DOI: 10.1007/s12664-016-0693-5. [19] 赵沁萍, 陈江, 刘春玉. 磁共振及磁共振胰胆管成像技术在诊断等密度胆系结石中的应用[J]. 广西医学, 2012, 40(6): 694−695, 700. DOI: 10.11675/j.issn.0253-4304.2018.06.26.
Zhao QP, Chen J, Liu CY. Application of magnetic resonance and magnetic resonance cholangiopancreatography in the diagnosis of equidensity biliary calculi[J]. Guangxi Med Sci, 2012, 40(6): 694−695, 700. DOI: 10.11675/j.issn.0253-4304.2018.06.26. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 6183
- HTML全文浏览量: 4551
- PDF下载量: 13