







-
行乳腺癌改良根治术的高危患者最常见的复发部位依次为胸壁、锁骨上下区、腋窝和内乳,因此胸壁和锁骨上下区为术后放疗常规照射部位[1]。乳腺癌患者行全乳切除术后胸壁较薄,在进行术后放疗时,通常对胸壁采用电子线照射,对锁骨上下区应用X射线照射,该放疗方式涉及到照射野的布野以及射野衔接问题。合理的体位设计能够保证混合射线照射野的布置,稳定的体位固定能够保证射野衔接处剂量分布的准确性,减小摆位误差,提高放疗位置的准确性。本研究回顾性分析采用两种装置(头颈肩热塑网罩和颈胸一体热塑体膜)固定患者的锁骨上下区的摆位误差和肩锁关节的位置移动,比较两种不同固定方式的优势。
-
选取2019年6至12月于中国医学科学院北京协和医学院肿瘤医院放疗科治疗的患者进行回顾性研究。本研究符合《赫尔辛基宣言》的原则。纳入标准:(1)能够接受乳腺癌改良根治术后放疗,并签署《放射治疗知情同意书》;(2)在锁骨上下靶区行X射线图像引导调强放疗,在胸壁(或胸壁+内乳)靶区行电子线放疗;(3)使用改造后的头颈肩热塑网罩或颈胸一体热塑体膜固定;(4)参考《放射治疗质量控制基本指南》[2]的要求,治疗前的锥形束CT(cone beam CT,CBCT)位置验证采用第一周连续3~5次,随后每周1次的扫描方式。排除标准:(1)因病情进展、幽闭恐惧等原因,不能保持体位进行放疗;(2)治疗前的CBCT次数少于5次。
根据以上标准,共入组40例女性患者,中位年龄为46(29~68)岁。其中,19例使用改造后的头颈肩热塑网罩固定(头颈肩网罩组,128次CBCT图像),21例使用颈胸一体热塑体膜固定(颈胸一体膜组,143次CBCT图像)。肿瘤发生在左侧的患者有25例、右侧15例。患者的卡氏评分为80~100分。中位体重指数(body mass index,BMI)为25.4(19.1~29.8)kg/m2,按照中国BMI标准[3]将所有患者分成BMI<24 kg/m2组(13例,86次CBCT扫描)和BMI≥24 kg/m2组(27例,185次CBCT扫描)。
-
使用改造后的头颈肩热塑网罩(广州科莱瑞迪医疗器材有限公司)固定患者,如图1所示,将患侧头颈肩网罩的固定边框自下面第二个固定钮处切除,使患侧上臂外展约45°,前臂内收,手掌扶髂前上棘,在体表标记手指的位置,肩部自然放松;健侧手臂置于体侧,手掌扶大腿外侧,肩部自然放松,根据患者颈长选择合适的头枕。使用颈胸一体热塑体膜(广州科莱瑞迪医疗器材有限公司)固定患者,如图2所示,患者两臂上举分别置于臂托和腕托之上,使患侧上臂外展约120°,双手分别握对应立柱,根据患者的身高、颈长,调节头枕的位置和型号。头颈肩网罩组在射野衔接处开半径约4 cm的圆孔,颈胸一体膜组使用专用的患侧乳腺区域开窗体膜。
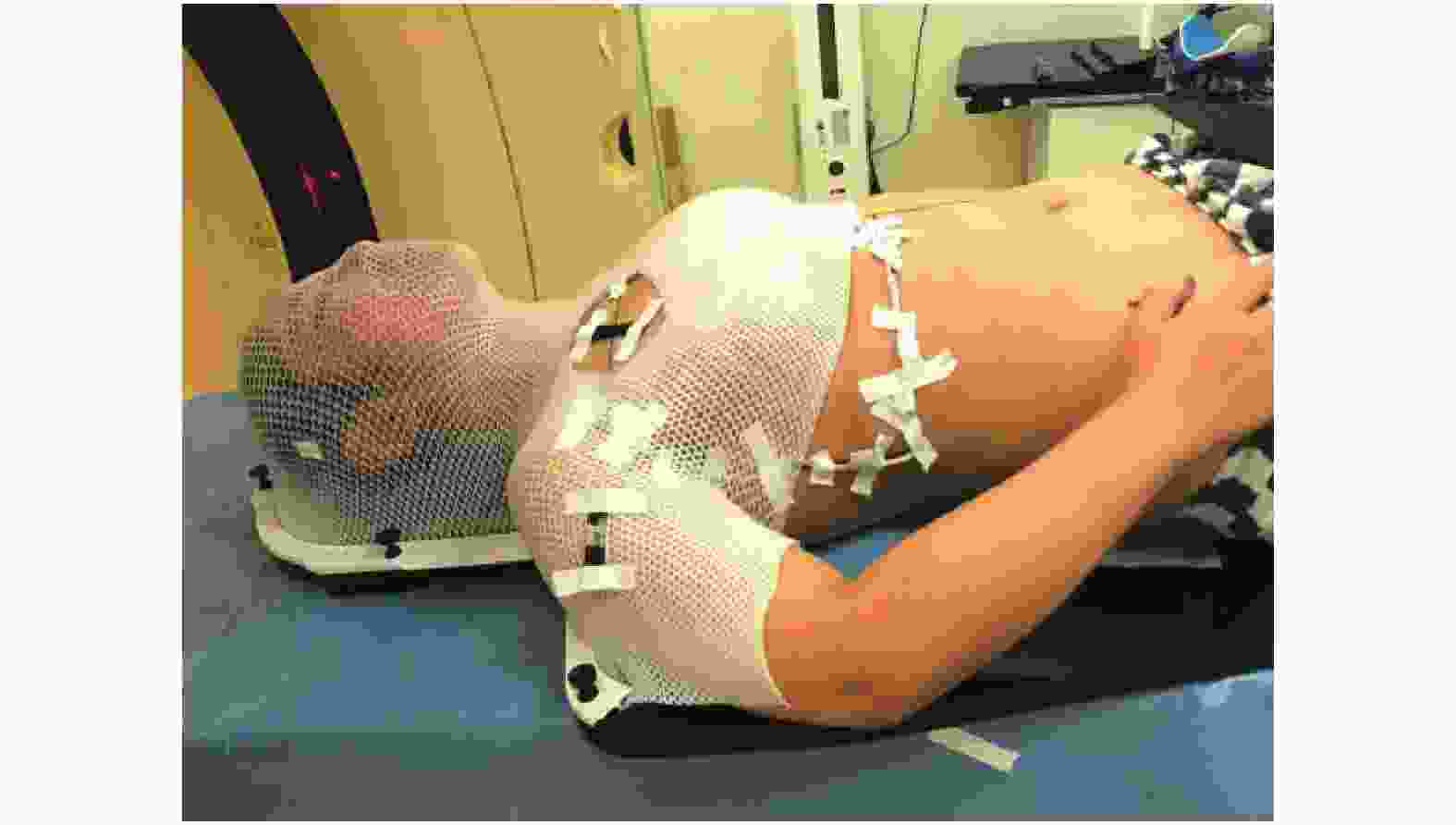
图 1 CT模拟定位患者的头颈肩热塑网罩体位固定
Figure 1. Patient immobilized with head/neck and shoulder thermoplastic mask during CT simulation

图 2 CT模拟定位患者的颈胸一体热塑体膜体位固定
Figure 2. Patient immobilized with integral cervicothoracic thermoplastic mask during CT simulation
-
所有患者均在自由呼吸状态下行CT定位扫描(CT仪为荷兰飞利浦公司的Brilliance Big Bore型或德国西门子公司的SOMATOM Definition AS 40型),锁骨上下区采用半野照射,通过小范围扫描,定出锁骨上下区的中心。锁骨上下区的治疗中心线标记在体表皮肤上,方便治疗时的摆位衔接。同时用铅丝在体表标出胸壁电子线射野范围。扫描层厚和层距均为5 mm,扫描上界至颅底,下界至肺部下方5 cm。在患者体表画摆位线,体中线延长至脐部。
-
通过MOSAIQ网络系统(瑞典医科达公司)将CT模拟定位图像传输至Pinnacle(version 9.10)计划系统(荷兰飞利浦公司)。术后预防照射的处方剂量为43.5 Gy(2.9 Gy/次),锁骨上下区靶区采用半野调强照射,6 MV X射线。胸壁内乳靶区采用电子线照射,根据胸壁弧度,机架角度偏向患侧乳腺30°~35°;根据胸壁的厚度和内乳区的深度,胸壁照射采用6 MeV 电子线(皮肤表面垫0.5 cm厚的硅胶,照射6~9次),内乳照射采用9~15 MeV 电子线。胸壁内乳野行电子线照射时需取下固定网罩或体膜,其上界与锁骨上下区半野的下界在体表皮肤上共线。合成X射线和电子线计划,限制和评估危及器官的剂量。
-
锁骨上下区调强放疗前行CBCT位置验证,扫描范围的上界在环状软骨上2 cm处,下界至健侧腺体下缘水平,前外界为腺体或胸壁皮肤以外,后内界包全整个椎体。配准框的范围以计划靶区(planning target volume,PTV)为基础在三维方向上各外扩2 cm,并包含椎体等附近固定的骨性结构。基于灰度值进行CBCT图像配准,记录平移摆位误差左右方向X、头脚方向Y、腹背方向Z和旋转摆位误差矢状面、横断面、冠状面,以颈椎和胸锁关节为配准标志,先自动配准,再手动调整。治疗时只做平移摆位误差校正,当平移摆位误差超过1 mm时,在线校正治疗床位置。
-
分析肩锁关节位置移动幅度时,以颈椎和胸锁关节为配准标志得到平移摆位误差X-sc、Y-sc、Z-sc,以肩锁关节为配准标志得到平移摆位误差X-ac、Y-ac、Z-ac,二者之差取绝对值,用ΔX=|X-sc−X-ac|、ΔY=|Y-sc−Y-ac|、ΔZ=|Z-sc−Z-ac|表示肩锁关节的位置移动幅度。用位移d(
$ d= $ $ \sqrt{{\varDelta X}^{2}+{\varDelta Y}^{2}+{\varDelta Z}^{2}} $ )表示肩锁关节在三维空间的位移。 -
采用文献[4]的公式MPTV=2.5∑+0.7σ计算靶区外放边界值,保证90%患者的CTV能够达到95%以上的处方剂量。上述公式中,M为外放边界;∑为系统摆位误差(个体患者误差平均值的标准差);σ为随机摆位误差(个体患者误差标准差的均方根)[5]。
-
应用SPSS 18.0软件对数据进行统计学分析。符合正态分布的数据以
$\bar x $ ±s表示,2组间的比较采用独立样本t检验(方差齐)。P<0.05为差异有统计学意义。 -
由表1可知,颈胸一体膜组在头脚方向的平移摆位误差和矢状面的旋转摆位误差的差异均有统计学意义(均P<0.05)。
组别 平移摆位误差(mm) 旋转摆位误差(度) 左右方向 头脚方向 腹背方向 矢状面 横断面 冠状面 头颈肩网罩组
(n=19)1.78±2.40 2.88±2.44 2.48±1.79 0.91±0.61 1.69±0.70 1.02±0.82 颈胸一体膜组
(n=21)2.26±1.91 2.29±1.89 1.66±2.00 0.67±0.53 0.92±0.75 0.75±0.71 t值 0.687 2.249 0.998 3.555 0.288 0.303 P值 0.496 0.030 0.325 0.001 0.776 0.763 注:∑为系统摆位误差(个体患者误差平均值的标准差);σ为随机摆位误差(个体患者误差标准差的均方根) 表 1 2组不同固定方式放疗患者锁骨上下区的平移和旋转摆位误差结果(∑±σ)
Table 1. Translation and rotation positioning errors of supra/infraclavicular of two groups of patients received radiotherapy with different fixation methods(∑±σ)
头颈肩网罩组和颈胸一体膜组在3个方向的平移摆位误差区间分布情况见图3~5。头颈肩网罩组和颈胸一体膜组在左右方向X、头脚方向Y、腹背方向Z平移摆位误差<3 mm的百分比分别为66.4%、57.0%、68.8%和67.1%、53.1%、73.4%,<5 mm的百分比分别为90.6%、81.3%、89.8%和89.5%、87.4%、93.0%;在矢状面、横断面、冠状面的旋转误差<1°的百分比分别为42.2%、43.0%、50.8%和74.8%、58.7%、67.8%,<2°的百分比分别为77.3%、64.8%、86.7%和97.2%、88.8%、93.7%。

图 3 2组不同固定方式放疗患者左右方向X平移误差的分布图
Figure 3. Distribution of translational errors of two groups of patients received radiotherapy with different fixation methods in left and right direction X

图 4 2组不同固定方式放疗患者头脚方向Y平移误差的分布图
Figure 4. Distribution of translational errors of two groups of patients received radiotherapy with different fixation methods in superior-inferior direction Y

图 5 2组不同固定方式放疗患者腹背方向Z平移误差的分布图
Figure 5. Distribution of translational errors of two groups of patients received radiotherapy with different fixation methods in anterior-posterior direction Z
-
头颈肩网罩组和颈胸一体膜组在左右方向X、头脚方向Y、腹背方向Z的位置移动幅度Δ X 、Δ Y 、Δ Z的平均值分别为3.65、4.61、3.11 mm和2.32、1.97、1.63 mm,三维空间位移d的平均值分别为7.36 mm和4.03 mm;在3个方向的最大位置移动幅度分别为14、20、13 mm和9、9、9 mm,最大三维空间位移分别为21.5 mm和15.0 mm。肩锁关节位置移动幅度及三维空间位移分布见图6。头颈肩网罩组的肩锁关节位置移动幅度ΔX、ΔY、ΔZ<10 mm的百分比分别为96.1%、88.3%、96.9%,<4 mm的百分比分别为55.5%、50.0%、67.2%;颈胸一体膜组的肩锁关节位置移动幅度ΔX、ΔY、ΔZ<6 mm的百分比分别为90.2%、93.7%、91.6%,<2 mm的百分比分别为45.5%、49.0%、66.4%。头颈肩网罩组和颈胸一体膜组的肩锁关节三维空间位移d<14 mm的百分比分别为89.1%和99.3%,d<10 mm的百分比分别为73.4%和93.0%,d<6 mm的百分比分别为46.9%和79.0%。
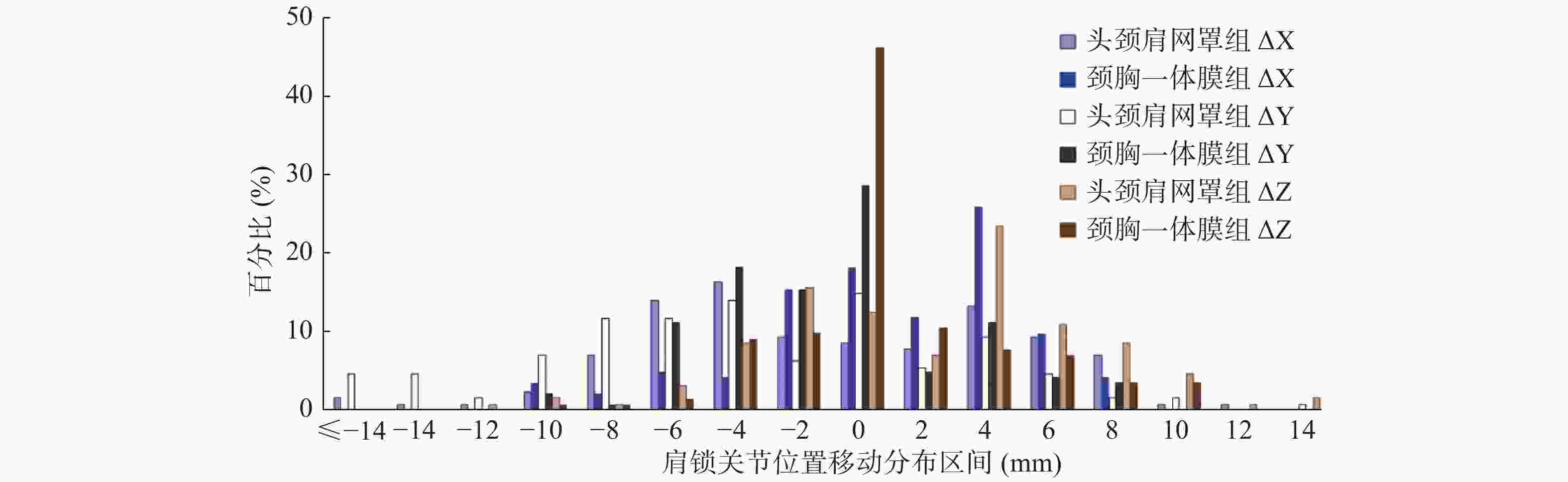
图 6 2组不同固定方式放疗患者固定肩锁关节位置移动幅度的分布图
Figure 6. Distribution of the range of acromioclavicular joint movement of two groups patients received radiotherapy with different frxation methods
-
由表2可知,BMI<24 kg/m2组和BMI≥24 kg/m2组患者在3个方向的平移和旋转摆位误差的差异均无统计学意义(均P>0.05)。
组别 平移摆位误差(mm) 旋转摆位误差(度) 左右方向 头脚方向 腹背方向 矢状面 横断面 冠状面 BMI<24组
(n=13)2.29±1.94 2.53±1.98 2.51±1.94 0.79±0.54 1.56±0.61 0.86±0.74 BMI≥24组
(n=27)1.92±2.24 2.87±2.25 1.91±1.89 1.01±0.58 1.20±0.77 0.89±0.78 t值 −0.439 0.478 0.218 0.938 −1.085 −1.103 P值 0.663 0.635 0.829 0.354 0.285 0.277 注:BMI为体重指数;∑为系统摆位误差(个体患者误差平均值的标准差);σ为随机摆位误差(个体患者误差标准差的均方根) 表 2 2组不同BMI放疗患者在3个方向的平移和旋转摆位误差(∑±σ)
Table 2. Setup errors of translation and rotation in three directions between the two groups of patients received radiotherapy with different body mass index(∑±σ)
-
头颈肩网罩组和颈胸一体膜组在左右方向X-sc、头脚方向Y-sc和腹背方向Z-sc的PTV外放边界值分别为6.1、8.9、7.5 mm和7.0、7.0、5.5 mm。
-
常规放疗时代,在行锁骨上野照射时,体位通常采用楔板加软枕的摆位装置,患侧手执耳,手臂上举外展,头偏向健侧。患者的手臂上举和外展角度以及头部偏转角度等没有限定,体位重复性无法保证,从而影响治疗的精度和剂量分布[6-7]。随着调强时代的到来,精准放疗面临着剂量梯度大、剂量分布易受摆位误差影响等挑战。本研究使用改造后的头颈肩热塑网罩固定,将患侧头颈肩网罩的固定边框自下面第二个固定钮处切除,可以使患侧上臂外展约45°,能够满足电子线布野的临床要求,还在射野衔接处开半径约4 cm的圆孔,在减少患者射野衔接处的皮肤牵拉的同时,尽量避免破坏网罩的整体性。本研究的锁骨上下区的摆位误差左右、头脚、腹背方向分别为(1.78±2.40)、(2.88±2.44)、(2.48±1.79) mm。按照相同的摆位误差计算公式统计研究锁骨上下区的摆位误差,结果发现吴传锋等[8]使用乳腺托架定位,锁骨上下区的摆位误差左右、头脚、腹背方向分别为(2.89±2.52)、(3.96±2.97)、(4.21±2.24) mm;本中心马茗微等[9]使用乳腺托架联合U型面罩固定头部,结果分别为(2.72±2.42)、(2.42±1.71)、(3.64±2.69) mm。由此可知,与传统的乳腺托架相比,头颈肩改造固定的方法简单易行,能够很好地固定患者的颈部,防止颈部旋转带来的位置不确定性。
除了头颈肩网罩外,乳腺托架、翼形板、负压真空袋和(或)发泡胶等其他乳腺摆位装置在临床上的应用也较多,上述装置虽然能够定量地对体位进行复位,但是对颈部和胸部没有固定,患者咳嗽、无意识性移动、身体僵直状态的改变等非自主性运动,可能会引起分次内误差较大[8]。本研究引入的颈胸一体架摆位装置有以下优势:(1)可以根据患者的体宽和臂展对臂托进行左右、进出和上下3个方向的位置调整,还可以进行臂托角度的调整,使患者上肢展开,方便乳腺和(或)胸壁切线野布野,同时患侧锁骨上下区皮肤展开无皱褶,可减轻皮肤反应;确保患侧上肢远离锁骨上下区,以免受到不必要的照射。(2)可以根据臂托的高度调节腕托的高度,提高上肢的稳定性。(3)可以根据手臂的松紧程度,调节握杆的位置,避免手臂发生旋转扭曲。(4)可以根据患者的身高颈长,调节头枕的位置和型号,提高患者的舒适性,保证放疗时患者的颈部体位有良好的重复性。
正常情况下,头颈肩网罩采用的是头颈部3个固定点和肩部2个固定点的“五点固定法”,在本研究中,我们为了使患侧手臂外展,切除了肩部的1个固定点,破坏了头颈肩网罩的整体性和稳定性,会导致固定效果下降。一般认为头颈部肿瘤的靶区外放为3~5 mm[10-11],但刘裕杰等[12]认为,颈部特有的非刚性运动较大,应将颈部靶区的外放扩大为5~10 mm,本研究锁骨上下区和颈部的摆位误差在左右、头脚、腹背方向分别为6.1、8.9、7.5 mm。有文献报道,头颈肩网罩固定的头颈部肿瘤下颈部的摆位误差大于头部,在左右 、头脚、腹背颈部系统误差分别是头部的2.33、1.67、1.56倍,颈部随机摆位误差分别是头部的2.57、1.34、0.99倍[13-14]。颈胸一体膜采用的是颈部2个固定点和胸部2个固定点的“四点固定法”,对颈部和胸部都有对称的2点固定,且颈部和胸部一体固定。本研究对科室使用的乳腺癌改良根治术后放疗的2种主要固定装置的摆位误差进行分组分析,结果表明,颈胸一体膜组对患者的头脚方向和矢状面的固定效果优于使用改造后的头颈肩网罩组。这是因为颈胸一体膜对颈、肩、胸部是整体固定的,而改造后的头颈肩面罩破坏了面罩的整体性和稳定性,只固定了头颈部,对肩部和胸部没有完整的固定,不能控制患者的“耸肩”、“垂肩”和“挺胸”动作。
锁骨上下区靶区采用X射线半野调强放疗,胸壁等采用电子线照射,二者的射野衔接尤为重要,而射野衔接处位于锁骨附近,肩关节的位置会对治疗中心造成影响。本研究分别测量了2组肩锁关节的位置移动幅度ΔX、ΔY、ΔZ,并进一步计算了肩锁关节的三维空间位移d。患者的“耸肩”和“垂肩”动作是以胸锁关节为定点,肩锁关节做三维空间上的钟摆运动,运动幅度的直观测量办法是在三个解剖平面用软件的测量工具测距,但所有患者测量的位置点很难统一。我们采用整体配准肩锁关节的办法,以胸锁关节(颈椎)为配准标志得到1组数据,然后以肩锁关节为配准标志得到另外1组数据,2者之差就是肩关节与定位时相比的移动量。结果表明,颈胸一体膜组肩关节的位置移动幅度的平均值以及三维空间位移的平均值均明显小于头颈肩网罩组。这是因为颈胸一体膜对上臂、前臂、腕部和手部均有定量的控制参数限制上肢体位,而头颈肩网罩仅要求患者手扶患侧髂前上棘部位,不能控制患者的“耸肩”或者“垂肩”动作,导致肩锁关节在三维方向上均有较大的摆位误差。
对于乳腺癌患者,摆位误差的大小也可能受BMI的影响[15-16]。本中心马茗微等[9]的前期研究报道,超重组(BMI≥24 kg/m2)与未超重组(BMI<24 kg/m2)在头脚和腹背方向的摆位误差差异无统计学意义,只有左右方向上的差异有统计学意义,归因为保乳术患者肥厚松弛的皮下脂肪。而本研究入组患者均为胸壁较薄的改良根治术患者,体表标记线相对保乳术患者不易受到牵拉影响,BMI≥24 kg/m2组与BMI<24 kg/m2组的平移摆位误差和旋转摆位误差的差异均无统计学意义。
2种固定方式均可用于乳腺癌改良根治术后的锁骨上下区的放疗,但相比头颈肩热塑网罩固定,颈胸一体热塑体膜固定在头脚方向的平移摆位和矢状面的旋转摆位误差均更小,而且对肩部的固定效果更优。根据以上研究结果,在行乳腺癌锁骨上下区放疗时,推荐采用颈胸一体热塑体膜固定体位。需要注意的是,由于患者背部无法垫斜板,对于胸壁内乳电子线照射,该固定方式只适合于胸壁表面在头脚方向上与电子线限光筒距离比较一致的患者。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 张彦新、郇福奎负责试验的设计与论文的撰写;耿松松、张焜、王宏负责数据的采集与整理;房辉、唐玉、景灏、王淑莲负责入组患者的筛选和放疗方案的制定;景灏、王淑莲、戴建荣负责论文的指导与修订。
乳腺癌改良根治术后放疗两种固定方式在锁骨上下区摆位误差的比较
Comparison of the setup errors of two mask systems for immobilizing supra/infraclavicular nodal region of breast cancer patients received postmastectomy radiotherapy
-
摘要:
目的 比较使用头颈肩热塑网罩和颈胸一体热塑体膜固定的乳腺癌改良根治术后放疗患者锁骨上下区的摆位误差。 方法 回顾性分析2019年6至12月中国医学科学院北京协和医学院肿瘤医院放疗科收治的40例女性乳腺癌改良根治术后患者[中位年龄46(29~68)岁]的锁骨上下区靶区的锥形束CT(CBCT)图像,其中19例使用头颈肩热塑网罩进行体位固定(头颈肩网罩组,128次CBCT图像),21例使用颈胸一体架膜进行体位固定(颈胸一体膜组,143次CBCT图像)。分析2组患者锁骨上下区的摆位误差,并分别测量肩锁关节的位置移动幅度ΔX、ΔY、ΔZ和三维空间位移d。应用公式计算临床靶区至计划靶区(PTV)的外放边界值。将所有患者分成体重指数(BMI)<24 kg/m2组(13例,86次CBCT扫描)和BMI≥24 kg/m2组(27例,185次CBCT扫描),分析比较2组的摆位误差。2组之间的比较采用独立样本t检验。 结果 头颈肩网罩组和颈胸一体膜组在锁骨上下区的平移摆位误差分别为左右方向:(1.78±2.40) mm和(2.26±1.91) mm(t=0.687,P=0.496)、头脚方向:(2.88±2.44) mm和(2.29±1.89) mm(t=2.249,P=0.030)、腹背方向:(2.48±1.79) mm和(1.66±2.00) mm(t=0.998,P=0.325);在矢状面的旋转摆位误差分别为(0.91±0.61)度和(0.67±0.53)度,差异有统计学意义(t=3.555,P=0.001)。头颈肩网罩组和颈胸一体膜组在肩锁关节的位置移动幅度ΔX、ΔY、ΔZ的平均值分别为3.65、4.61、3.11 mm和2.32、1.97、1.63 mm,三维空间位移d的平均值分别为7.36 mm和4.03 mm。头颈肩网罩组和颈胸一体膜组锁骨上下区在左右方向、头脚方向和腹背方向的PTV外放边界值分别为6.1、8.9、7.5 mm和7.0、7.0、5.5 mm。BMI<24 kg/m2组和BMI≥24 kg/m2组患者在3个方向的平移和旋转摆位误差的差异均无统计学意义(t=−1.103~0.938,均P>0.05)。 结论 对于乳腺癌改良根治术后行锁骨上下区放疗的患者,相比头颈肩网罩固定,使用颈胸一体膜固定在头脚方向的摆位误差更小,而且对肩锁关节的体位固定效果更优。 -
关键词:
- 乳腺肿瘤 /
- 乳房切除术,改良根治性 /
- 放射疗法,计算机辅助 /
- 体位固定 /
- 摆位误差
Abstract:Objective To compare the setup errors of breast cancer patients who received postmastectomy radiotherapy (PMRT) with head/neck and shoulder thermoplastic mask and integral cervicothoracic mask. Methods A retrospective analysis was performed on 40 female breast cancer patients (median age 46 (29–68) years) who treated with PMRT in Cancer Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College from June to December 2019. The supra/infraclavicular nodal region was irradiated with intensity-modulated radiotherapy technique and chest wall ± internal mammary chain were irradiated with electrons. A total of 271 cone beam CT (CBCT) images of the supra/infraclavicular nodal region were analyzed retrospectively. One hundred and twenty eight CBCT images were from 19 patients immobilized with head/neck and shoulder thermoplastic mask, and 143 CBCT images were from 21 patients immobilized with integral cervicothoracic thermoplastic mask. The setup errors of the two groups were analyzed, and the movement amplitude ΔX, ΔY, ΔZ and three-dimensional displacement d of acromioclavicular joint were measured. According to van Herk's formula, MPTV=2.5∑+0.7σ, the margin from clinical target volume to planning target volume (PTV) is calculated. According to whether body mass index (BMI)≥24 kg/m2, the patients were divided into two groups to analyze whether there was statistical difference of the setup errors. The differences were compared by independent sample t test. Results The translational setup errors of the supra/infraclavicular nodal region for head/neck and shoulder and integral cervicothoracic thermoplastic mask groups in the left–right, superior–inferior, and anterior–posterior directions were as follows: (1.78±2.40) mm and (2.26±1.91) mm (t=0.687, P=0.496); (2.88±2.44) mm and 2.29±1.89 mm (t=2.249, P=0.030); (2.48±1.79) mm and (1.66±2.00) mm (t=0.998, P=0.325), respectively; the rotational setup errors in the sagittal directions were (0.91±0.61)° and (0.67±0.53)°, and the difference was statistically significant (t=3.555, P=0.001). The arithmetic mean of movement amplitude of the acromioclavicular joint ( ΔX, ΔY, and ΔZ ) were 3.65, 4.61, 3.11 mm and 2.32, 1.97, 1.63 mm in the X, Y, and Z directions, respectively. The arithmetic mean of three-dimensional displacement d were 7.36 mm and 4.03 mm, respectively. The calculated PTV margin in the left–right, superior–inferior, and anterior–posterior directions with head/neck and shoulder and integral cervicothoracic mask groups were 6.1, 8.9, and 7.5 mm and 7.0, 7.0, and 5.5 mm, respectively. No significant difference was found between the BMI<24 and BMI≥24 kg/m2 groups in translation and rotation setup errors in the three directions (t=−1.103 to 0.938, all P>0.05). Conclusions The integral cervicothoracic mask system for patients who received PMRT in the supra/infraclavicular nodal region after the modified radical mastectomy provides smaller setup errors than the head and neck–shoulder thermoplastic mask system in the superior–inferior direction. This system also has remarkable body position fixation effects on the acromioclavicular region. -
图 1 CT模拟定位患者的头颈肩热塑网罩体位固定
Figure 1. Patient immobilized with head/neck and shoulder thermoplastic mask during CT simulation
图 2 CT模拟定位患者的颈胸一体热塑体膜体位固定
Figure 2. Patient immobilized with integral cervicothoracic thermoplastic mask during CT simulation
图 3 2组不同固定方式放疗患者左右方向X平移误差的分布图
Figure 3. Distribution of translational errors of two groups of patients received radiotherapy with different fixation methods in left and right direction X
图 4 2组不同固定方式放疗患者头脚方向Y平移误差的分布图
Figure 4. Distribution of translational errors of two groups of patients received radiotherapy with different fixation methods in superior-inferior direction Y
图 5 2组不同固定方式放疗患者腹背方向Z平移误差的分布图
Figure 5. Distribution of translational errors of two groups of patients received radiotherapy with different fixation methods in anterior-posterior direction Z
图 6 2组不同固定方式放疗患者固定肩锁关节位置移动幅度的分布图
Figure 6. Distribution of the range of acromioclavicular joint movement of two groups patients received radiotherapy with different frxation methods
表 1 2组不同固定方式放疗患者锁骨上下区的平移和旋转摆位误差结果(∑±σ)
Table 1. Translation and rotation positioning errors of supra/infraclavicular of two groups of patients received radiotherapy with different fixation methods(∑±σ)
组别 平移摆位误差(mm) 旋转摆位误差(度) 左右方向 头脚方向 腹背方向 矢状面 横断面 冠状面 头颈肩网罩组
(n=19)1.78±2.40 2.88±2.44 2.48±1.79 0.91±0.61 1.69±0.70 1.02±0.82 颈胸一体膜组
(n=21)2.26±1.91 2.29±1.89 1.66±2.00 0.67±0.53 0.92±0.75 0.75±0.71 t值 0.687 2.249 0.998 3.555 0.288 0.303 P值 0.496 0.030 0.325 0.001 0.776 0.763 注:∑为系统摆位误差(个体患者误差平均值的标准差);σ为随机摆位误差(个体患者误差标准差的均方根)  下载: 导出CSV
下载: 导出CSV
表 2 2组不同BMI放疗患者在3个方向的平移和旋转摆位误差(∑±σ)
Table 2. Setup errors of translation and rotation in three directions between the two groups of patients received radiotherapy with different body mass index(∑±σ)
组别 平移摆位误差(mm) 旋转摆位误差(度) 左右方向 头脚方向 腹背方向 矢状面 横断面 冠状面 BMI<24组
(n=13)2.29±1.94 2.53±1.98 2.51±1.94 0.79±0.54 1.56±0.61 0.86±0.74 BMI≥24组
(n=27)1.92±2.24 2.87±2.25 1.91±1.89 1.01±0.58 1.20±0.77 0.89±0.78 t值 −0.439 0.478 0.218 0.938 −1.085 −1.103 P值 0.663 0.635 0.829 0.354 0.285 0.277 注:BMI为体重指数;∑为系统摆位误差(个体患者误差平均值的标准差);σ为随机摆位误差(个体患者误差标准差的均方根)
下载: 导出CSV
-
[1] 王淑莲, 李晔雄, 宋清坤, 等. 1999−2008年中国乳腺癌根治术后放疗部位变化的临床流行病学研究[J]. 中华放射肿瘤学杂志, 2013, 22(5): 347−351. DOI: 10.3760/cma.j.issn.1004-4221.2013.05.002.
Wang SL, Li YX, Song QK, et al. Changes in postmastectomy radiotherapy targets among breast cancer patients in China from 1999 to 2008: an epidemiological study[J]. Chin J Radiat Oncol, 2013, 22(5): 347−351. DOI: 10.3760/cma.j.issn.1004-4221.2013.05.002.[2] 国家肿瘤诊疗质控中心放疗质控专家委员会, 赫捷, 王绿化, 等. 放射治疗质量控制基本指南[J]. 中华放射肿瘤学杂志, 2018, 27(4): 335−342. DOI: 10.3760/cma.j.issn.1004-4221.2018.04.001.
Comittee of Quality Control in Radiotherapy, National Cancer Diagnosis and Treatment Quality Control Center, He J, Wang LH, et al. Basic guidelines of quality control for radiotherapy[J]. Chin J Radiat Oncol, 2018, 27(4): 335−342. DOI: 10.3760/cma.j.issn.1004-4221.2018.04.001.[3] 国际生命科学学会中国办事处中国肥胖问题工作组联合数据汇总分析协作组, 陈春明. 中国成人体质指数分类的推荐意见简介[J]. 中华预防医学杂志, 2001, 35(5): 349−350. DOI: 10.3760/j.issn.0253-9624.2001.05.019.
Joint Data Collection and Analysis Cooperation Group of Chinese Obesity Working Group of International Life Science Society China Office, Chen CM. A brief introduction to the recommendation of Chinese adult body mass index classification[J]. Chin J Prev Med, 2001, 35(5): 349−350. DOI: 10.3760/j.issn.0253-9624.2001.05.019.[4] van Herk M. Errors and margins in radiotherapy[J]. Semin Radiat Oncol, 2004, 14(1): 52−64. DOI: 10.1053/j.semradonc.2003.10.003. [5] Hugo GD, Yan D, Liang J. Population and patient-specific target margins for 4D adaptive radiotherapy to account for intra- and inter-fraction variation in lung tumour position[J]. Phys Med Biol, 2007, 52(1): 257−274. DOI: 10.1088/0031-9155/52/1/017. [6] 徐晓, 张敏娜, 王冰, 等. 乳腺癌保乳术后调强放疗摆位误差相关因素分析[J]. 中华放射医学与防护杂志, 2019, 39(6): 434−438. DOI: 10.3760/cma.j.issn.0254-5098.2019.06.006.
Xu X, Zhang MN, Wang B, et al. Factors associated with set-up errors in intensity-modulated radiotherapy after breast conserving surgery[J]. Chin J Radiol Med Prot, 2019, 39(6): 434−438. DOI: 10.3760/cma.j.issn.0254-5098.2019.06.006.[7] 谢涛, 许青, 彭佳元, 等. 乳腺癌胸壁野结合锁骨上野放疗时头部固定的重要性研究[J]. 中华放射肿瘤学杂志, 2018, 27(5): 500−503. DOI: 10.3760/cma.j.issn.1004-4221.2018.05.013.
Xie T, Xu Q, Peng JY, et al. Study of significance of head fixation in the chest wall field combined with supraclavicular field radiotherapy for breast cancer[J]. Chin J Radiat Oncol, 2018, 27(5): 500−503. DOI: 10.3760/cma.j.issn.1004-4221.2018.05.013.[8] 吴传锋, 吴锦昌, 顾科, 等. 利用CBCT研究乳腺托架固定下乳腺癌放疗下颈摆位误差及相应CTV外放边界[J]. 中华放射医学与防护杂志, 2016, 36(10): 753−756. DOI: 10.3760/cma.j.issn.0254-5098.2016.10.007.
Wu CF, Wu JC, Gu K, et al. Analysis of lower neck setup errors and planning target margin by CBCT for breast cancer radiation with breast bracket immobilized[J]. Chin J Radiol Med Prot, 2016, 36(10): 753−756. DOI: 10.3760/cma.j.issn.0254-5098.2016.10.007.[9] 马茗微, 王淑莲, 覃仕瑞, 等. 面罩及乳腺托架固定下乳腺癌保乳术后放疗锁骨上下区摆位误差分析[J]. 中华放射肿瘤学杂志, 2019, 28(3): 217−221. DOI: 10.3760/cma.j.issn.1004-4221.2019.03.012.
Ma MW, Wang SL, Qin SR, et al. Breast board combined with a thermoplastic head mask immobilization can improve the reproducibility of the treatment setup for breast cancer patients receiving whole breast and supraclavicular nodal region irradiation[J]. Chin J Radiat Oncol, 2019, 28(3): 217−221. DOI: 10.3760/cma.j.issn.1004-4221.2019.03.012.[10] Lee SW, Back GM, Yi BY, et al. Preliminary results of a phase Ⅰ/Ⅱ study of simultaneous modulated accelerated radiotherapy for nondisseminated nasopharyngeal carcinoma[J]. Int J Radiat Oncol Biol Phys, 2006, 65(1): 152−160. DOI: 10.1016/j.ijrobp.2005.10.040. [11] van Lin ENJT, van der Vight L, Huizenga H, et al. Set-up improvement in head and neck radiotherapy using a 3D off-line EPID-based correction protocol and a customised head and neck support[J]. Radiother Oncol, 2003, 68(2): 137−148. DOI: 10.1016/s0167-8140(03)00134-8. [12] 刘裕杰, 周莉钧, 管西寅, 等. 图像引导的放射治疗在头颈部肿瘤治疗中的应用[J]. 中国癌症杂志, 2010, 20(9): 707−711. DOI: 10.3969/j.issn.1007-3639.2010.09.014.
Liu YJ, Zhou LJ, Guan XY, et al. Application of image-guided radiotherapy in head-and-neck cancer[J]. China Oncol, 2010, 20(9): 707−711. DOI: 10.3969/j.issn.1007-3639.2010.09.014.[13] 林承光, 林刘文, 刘秉梯, 等. 鼻咽癌三维适形和调强放疗过程中头部与颈部摆位误差比较研究[J]. 中华放射肿瘤学杂志, 2011, 20(4): 322−325. DOI: 10.3760/cma.j.issn.1004-4221.2011.04.018.
Lin CG, Lin LW, Liu BT, et al. A study of the positioning errors of head and neck in the process of intensity modulation radiated therapy of nasopharyngeal carcinoma[J]. Chin J Radiat Oncol, 2011, 20(4): 322−325. DOI: 10.3760/cma.j.issn.1004-4221.2011.04.018.[14] 许森奎, 姚文燕, 胡江, 等. 鼻咽癌发泡胶个体化塑形与标准化头枕放疗体位固定精确度比较[J]. 中华放射肿瘤学杂志, 2015, 24(2): 196−199. DOI: 10.3760/cma.j.issn.1004-4221.2015.02.022.
Xu SK, Yao WY, Hu J, et al. The research of accuracy immobilized using individualized polyurethane scaling agent compared to positioning foam with standard plastics pillow in the radiotherapy of nasopharyngeal carcinoma[J]. Chin J Radiat Oncol, 2015, 24(2): 196−199. DOI: 10.3760/cma.j.issn.1004-4221.2015.02.022.[15] Batumalai V, Phan P, Choong C, et al. Comparison of setup accuracy of three different image assessment methods for tangential breast radiotherapy[J]. J Med Radiat Sci, 2016, 63(4): 224−231. DOI: 10.1002/jmrs.180. [16] 于舒飞, 王淑莲, 唐玉, 等. 乳腺托架固定下全乳调强放疗CBCT测定摆位误差的研究[J]. 中华放射肿瘤学杂志, 2019, 28(7): 532−535. DOI: 10.3760/cma.j.issn.1004-4221.2019. 07.012.
Yu SF, Wang SL, Tang Y, et al. Study of setup error in cone beam CT for whole breast intensity-modulated radiotherapy with breast board immobilization[J]. Chin J Radiat Oncol, 2019, 28(7): 532−535. DOI: 10.3760/cma.j.issn.1004-4221.2019. 07.012. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 5603
- HTML全文浏览量: 4579
- PDF下载量: 28


