



-
放射性核素骨显像以99Tcm-MDP为示踪剂,其原理是通过与骨的羟基磷灰石晶体发生离子交换、化学吸附及与骨组织中有机成分结合沉积于骨组织中而显影,被广泛用于评价原发性骨肿瘤、各种恶性肿瘤的骨转移、感染和骨折等[1]。对于肿瘤患儿,已有不少关于骨显像时骨外组织器官或软组织肿瘤摄取99Tcm-MDP的个案报道[2-4],但缺少较大样本的研究。儿童骨外软组织肿瘤99Tcm-MDP显影与肿瘤组织病理学的关系尚未见报道。笔者收集骨显像时骨外软组织肿瘤显影的肿瘤患儿,结合其他相关影像学检查及病理检查结果,回顾性分析肿瘤患儿摄取99Tcm-MDP的常见骨外软组织肿瘤、肿瘤的影像学特点及其与组织病理学的关系。
-
收集2008年12月至2018年12月在上海交通大学医学院附属新华医院核医学科和同济大学附属第十人民医院核医学科行骨显像的肿瘤患儿共1025例,纳入33例骨外软组织肿瘤显影的肿瘤患儿进行回顾性研究,年龄3个月~10岁,中位年龄3岁,其中男患儿21例、女患儿12例。纳入标准:①未经专科治疗的骨外软组织肿瘤显影;②骨外显影的软组织肿瘤均由相邻期限内(2个月以内)其他的影像学检查证实,如CT、MRI、超声;③骨外显影的软组织肿瘤须有组织病理学检查;④鉴于儿童肿瘤好发年龄<15岁,因此根据Doll[5]修订的《国际标准人口》将≤14岁定义为儿童。排除标准:①非肿瘤原因引起的泌尿系统显影,包括因MDP经泌尿系统正常排泄引起的双肾、输尿管及膀胱的显影,和由结石等梗阻原因引起的泌尿系统显影;②由药物标记等技术原因引起的甲状腺显影;③由于技术因素导致的污染病例;④由于显像剂注射渗漏造成的淋巴结显影;⑤因骨折、感染等引起的骨外良性软组织显影。
33例患儿联合超声、MRI、CT等(均在骨显像前后1个月内)相关检查帮助定位显影的软组织肿瘤。所有患儿在行骨显像前后1周内血钙浓度均在正常范围内,所有诊断结果均于骨显像前后1~2个月通过穿刺活检或术后病理证实。骨显像均未发现骨转移灶。
所有患儿父母或其法定监护人均在检查前签署了知情同意书。本研究获得上海交通大学医学院附属新华医院(批准号:XHEC-D-2017-042)和同济大学附属第十人民医院伦理委员会批准(批准号:SHSY-IEC-KY-3.0/18-147/01)。
-
显像剂99Tcm-MDP注射液由上海原子科兴药业有限公司提供,放射化学纯度>95%。显像仪器为荷兰Philips公司 Precedence 16 SPECT/CT。图像处理系统为美国通用生产的Milwaukee WI,配低能高分辨平行孔准直器。检查前排空尿液,无法配合的患儿需给予口服水合氯醛镇静(0.5 mL/kg)。患儿以7.4 MBq(0.2 mCi)/kg静脉注射99Tcm-MDP,最小剂量37 MBq(1 mCi)[6],2~3 h后行全身骨显像,扫描速度10~20 cm/min,窗宽10%,能峰140 keV,矩阵256×1024。常规采集前后位图像,必要时采集侧位图像,未行同机断层CT检查,以避免患儿接受更多的辐射。疑有尿液污染时,清洗或除去污染衣物后加做局部显影。
-
由2位有5年以上工作经验的核医学科主治医师根据CT、MRI或超声提示的病灶位置,对骨外显像的软组织肿瘤内部最高摄取和全身骨骼的放射性浓聚程度进行判断。以病灶区放射性高于正常下肢软组织,低于正常肋骨放射性分布为“+”;等于或高于正常肋骨放射性分布,低于正常胸骨体或脊柱放射性分布为“++”;等于或高于正常胸骨体或脊柱放射性分布为“+++”。
-
所有病理结果根据第9版《病理学》[7]肿瘤分类原则进行分组。如按照患儿具体的组织病理学分类,则存在某些肿瘤例数过少,缺失格子数较多的现象。因此,本研究将33例患儿按照肿瘤的起源将其分为起源于幼稚细胞的母细胞瘤(包括神经母细胞瘤、肝母细胞瘤、肾母细胞瘤、胰母细胞瘤)、间叶组织肿瘤(骨肉瘤肺转移灶、恶性肾外横纹肌样瘤、脉管瘤)、生殖细胞肿瘤等3大类。另外,按照肿瘤的分化程度进行分类,分别分析不同病理类型、不同分化程度的肿瘤之间摄取99Tcm-MDP的差异及其原因。
-
采用IBM SPSS 24.0软件对数据进行统计学分析。多组间的比较采用等级资料的秩和检验(Kruskal-Willis H秩和检验)。P<0.05为差异有统计学意义。
-
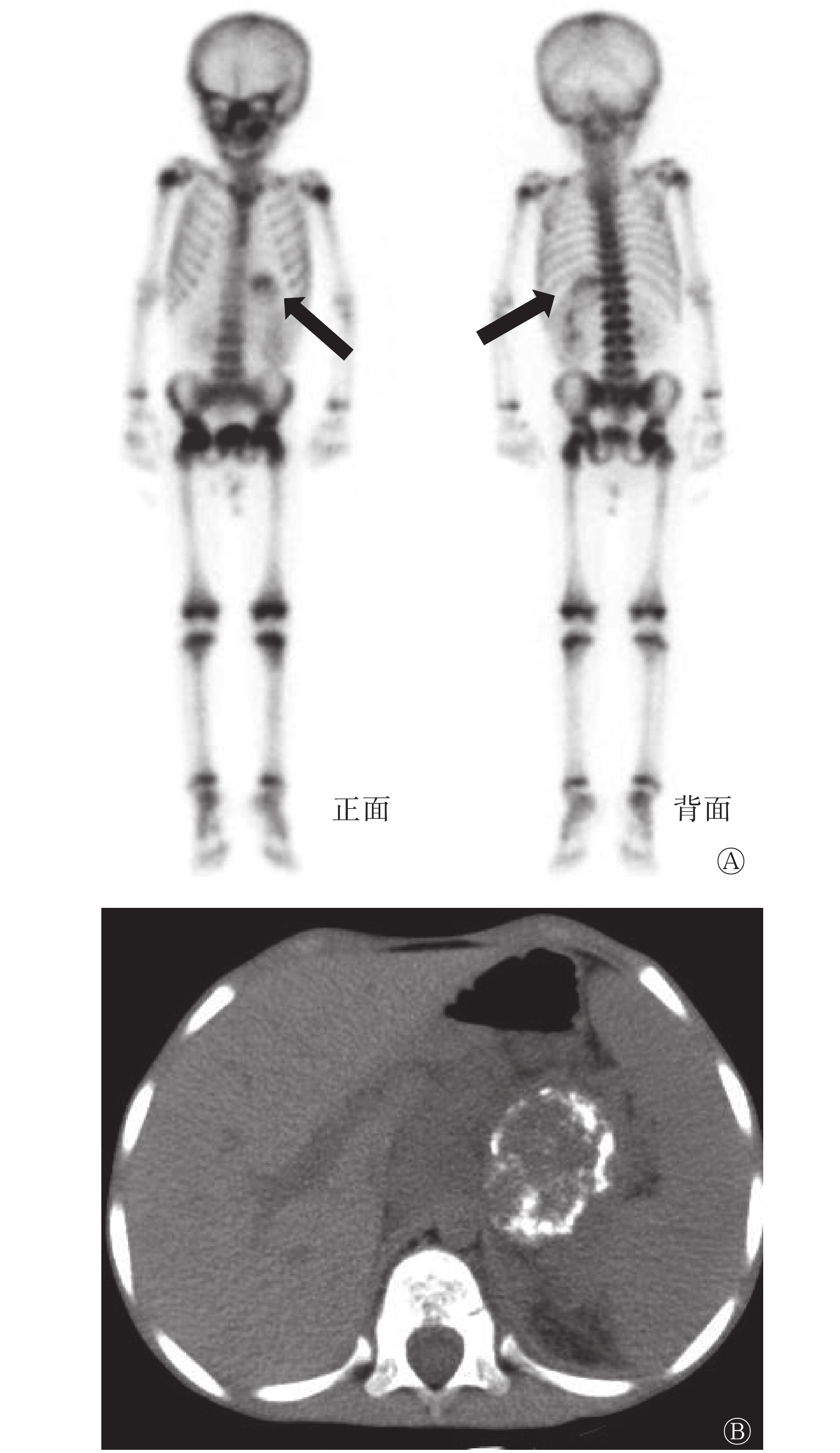
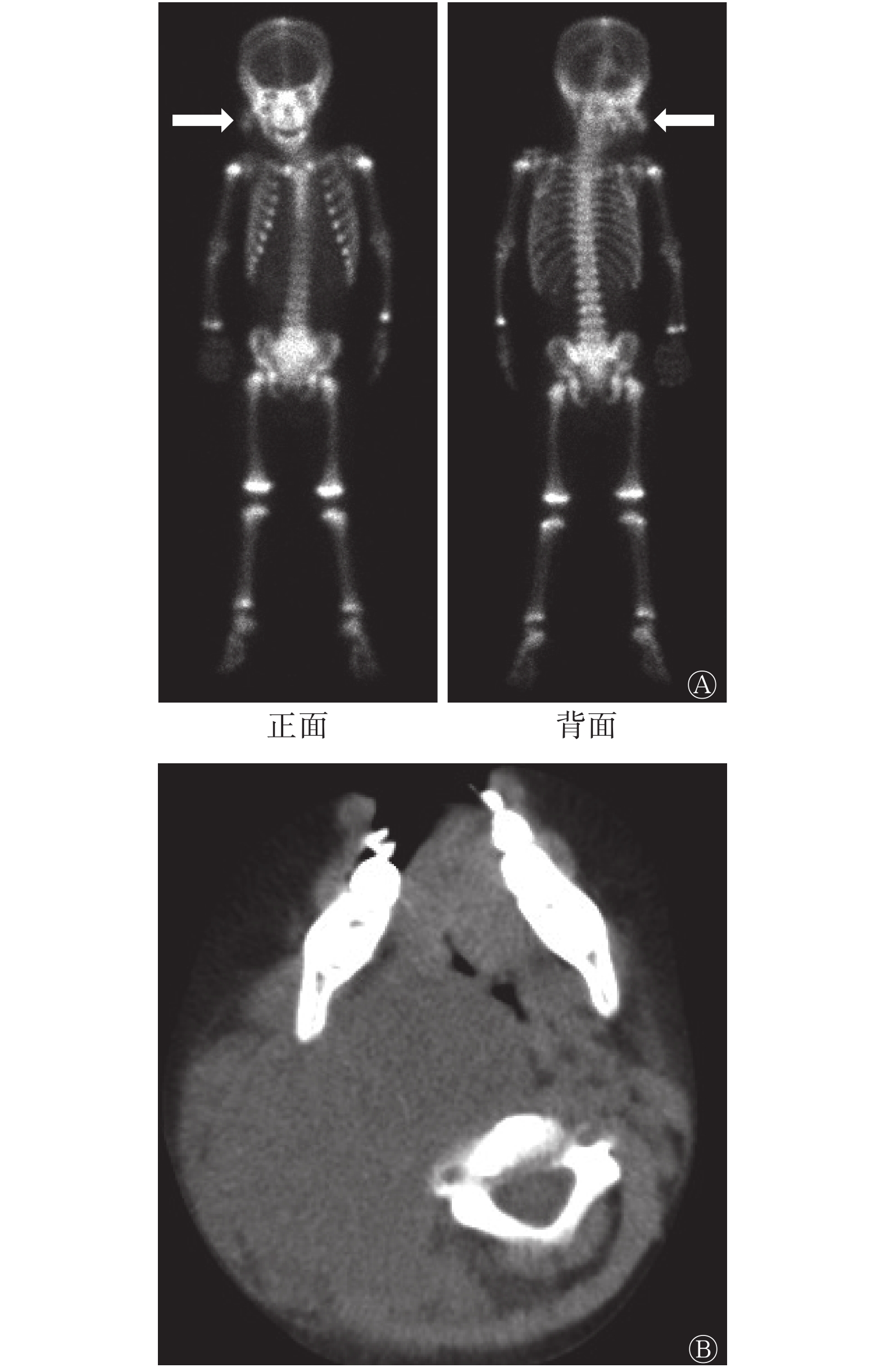
33例肿瘤患儿骨外软组织肿瘤摄取99Tcm-MDP的情况见表1,以神经母细胞瘤最多见,其次为肾母及肝母细胞瘤。另外,结合其他相关检查(包括CT、MRI、超声以及病理学检查结果),1例患儿右颈部恶性肾外横纹肌样瘤(图1);1例患儿左大腿脉管瘤均表现为密度均匀的软组织肿瘤(图2);3例患儿骨肉瘤肺转移灶本身含有骨样基质,其余28例(28/33,84.8%)患儿的软组织肿瘤均伴有不同程度的坏死和(或)钙化(图3),其他具体数据见表2。SPECT/CT显像结果显示,肿瘤内含有钙化和坏死、具有钙化或坏死其中之一表现,以及其他原因引起的99Tcm-MDP摄取程度之间的差异无统计学意义(H=2.313, P=0.315)。所有显影的骨外软组织肿瘤的长径为1.5~30.0 cm。33例患儿中仅4例进行过增强CT检查,均表现为不均匀明显强化。
肿瘤分类 软组织肿瘤类型 例数(%) 放射性浓聚程度(例) + ++ +++ 母细胞瘤 神经母细胞瘤 15(45.5) 2 5 8 肾母细胞瘤 6(18.2) 2 2 2 肝母细胞瘤 4(12.1) 0 2 2 胰母细胞瘤 1(3.0) 1 0 0 间叶组织肿瘤 骨肉瘤肺转移灶 3(9.1) 0 1 2 恶性肾外横纹肌样瘤 1(3.0) 0 1 0 左大腿脉管瘤 1(3.0) 1 0 0 生殖细胞肿瘤 生殖细胞肿瘤 2(6.1) 0 0 2 合计 33 6 11 16 注:表中,以病灶区放射性高于正常下肢软组织,低于正常肋骨放射性分布为“+”;等于或高于正常肋骨放射性分布,低于正常胸骨体或脊柱放射性分布为“++”;等于或高于正常胸骨体或脊柱放射性分布为“+++”。MDP:亚甲基二膦酸盐 表 1 33例摄取99Tcm-MDP的患儿软组织肿瘤的类型和放射性浓聚程度的比较
Table 1. Types of pediatric soft tissue tumors and their degrees of 99Tcm-MDP uptake in 33 children patients

图 1 右颈部恶性肾外横纹肌样瘤99Tcm-MDP骨显像及CT图像(男患儿,2岁)
Figure 1. 99Tcm-MDP uptake in malignant extrarenal rhabdoid tumor in the right neck and its corresponding CT image (male, 2 years old)

图 2 左大腿软组织脉管瘤99Tcm-MDP骨显像及CT图像(男患儿,1岁)
Figure 2. 99Tcm-MDP uptake in the left thigh vascular tumor and its corresponding CT image (male, 1 year old)
浓聚程度 钙化伴坏死 坏死 钙化 其他a 合计 + 0 4(66.7) 1(16.7) 1(16.7) 6 ++ 6(54.5) 0 3(27.3) 2(18.2) 11 +++ 8(50.0) 0 6(37.5) 2(12.5) 16 合计 14 4 10 5 33 注:表中,a:包含骨外软组织肿瘤未见明显坏死及钙化2例(摄取99Tcm-MDP的程度分别为“+”、“++”各1例)及3例含有骨化基质(摄取99Tcm-MDP的程度表现为“++”1例,“+++”2例)的患者。以病灶区放射性高于正常下肢软组织,低于正常肋骨放射性分布为“+”;等于或高于正常肋骨放射性分布,低于正常胸骨体或脊柱放射性分布为“++”;等于或高于正常胸骨体或脊柱放射性分布为“+++” 表 2 33例患儿骨外软组织肿瘤中的钙化和坏死的情况 [例(%)]
Table 2. Main imaging features of pediatric extraosseous soft tissue tumors in 33 children patients
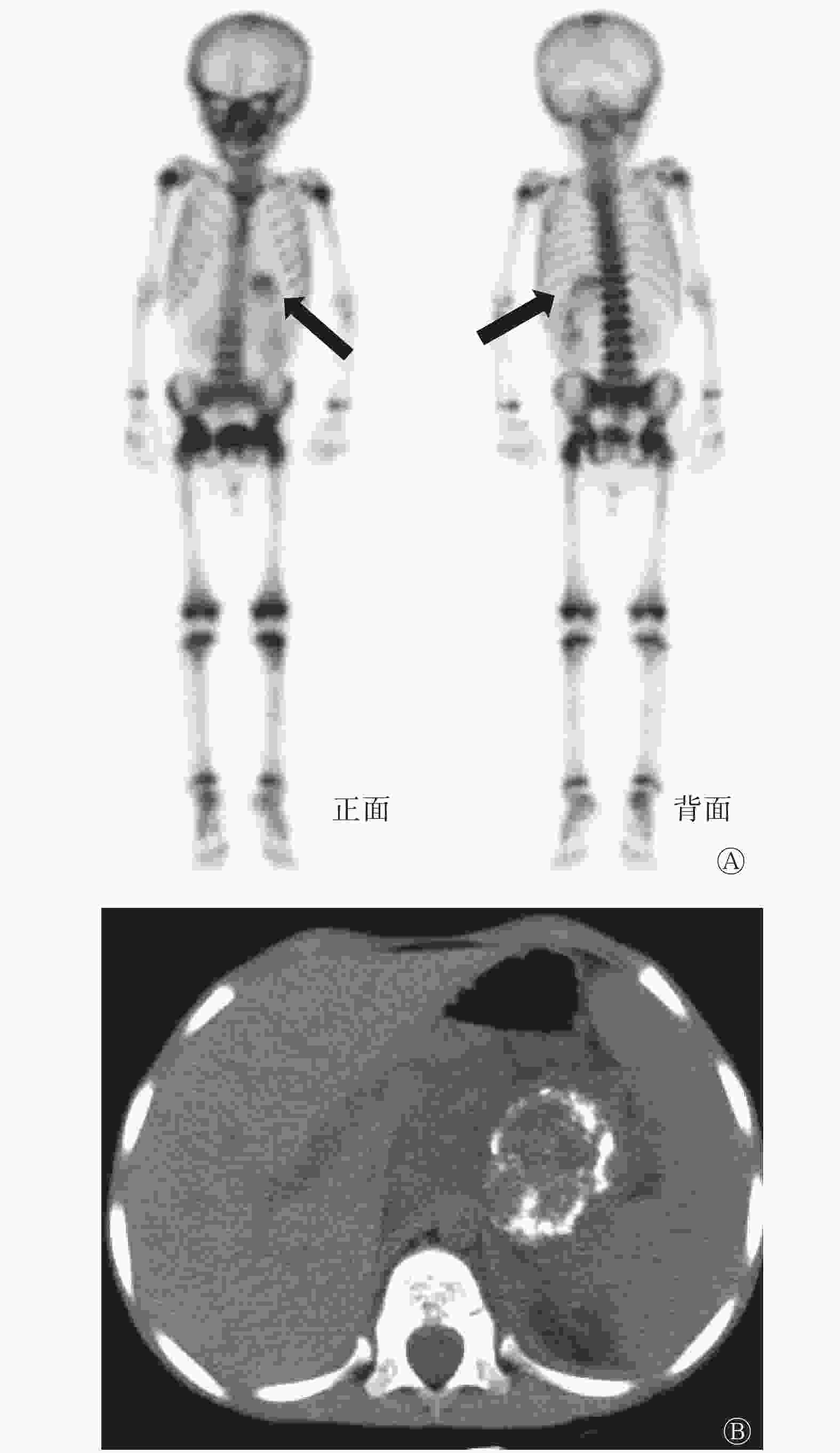
图 3 左侧腹膜后神经母细胞瘤99Tcm-MDP骨显像及CT图像(男患儿,7岁)
Figure 3. 99Tcm-MDP uptake in neuroblastoma in the left retroperitoneum and its corresponding CT image (male, 7 years old)
-
33例不同病理分类患儿的软组织肿瘤中,摄取程度表现为“+”的6例(6/33, 18.2%),包括母细胞瘤5例(5/6, 83.3%)、间叶组织肿瘤1例(1/6, 16.7%);摄取程度为“++”的11例(11/33, 33.3%),包括母细胞瘤9例(9/11, 81.8%)、间叶组织肿瘤2例(2/11, 18.2%);摄取程度为“+++”的16例(16/33, 48.5%),包括母细胞瘤12例(12/16, 75.0%)、间叶组织肿瘤2例(2/16, 12.5%)、生殖细胞肿瘤2例(2/16, 12.5%)。3种不同病理类型的儿童软组织肿瘤摄取99Tcm-MDP程度的差异无统计学意义(H=1.993,P=0.369)。
-
33例肿瘤患儿中,15例神经母细胞瘤患儿具有组织分化程度的详细诊断,包含以分化型为主的6例(6/15,40%),其中“+”1例,“++”4例,“+++”1例;以分化差型为主的9例(9/15,60%),其中“+”1例,“++”1例,“+++”7例。
-
放射性核素骨显像时,骨外软组织异常摄取99Tcm-MDP通常见于技术伪影、正常组织器官显影和肿瘤组织异常摄取[8-12]。本研究收集的33例肿瘤患儿仅有1例为良性脉管瘤,其余32例均为恶性肿瘤,因此,我们认为在排除正常组织器官99Tcm-MDP显影及技术因素的前提下,骨显像时骨外软组织肿瘤异常摄取99Tcm-MDP多提示恶性肿瘤的可能,这与之前的报道基本一致[13-14],但由于骨显像受检者大多数有肿瘤病史或为怀疑患有肿瘤的患者,纳入研究的人群本身存在偏倚,也可能会造成恶性肿瘤患者占比较高。以往文献报道肿瘤患儿摄取99Tcm-MDP的骨外软组织肿瘤有神经母细胞瘤、骨肉瘤和横纹肌肉瘤等[3,15-16],但缺少较大样本的系统研究。本研究分析了近10年2家核医学中心骨外软组织肿瘤显影的33例患儿,结果显示,摄取99Tcm-MDP的骨外软组织肿瘤以神经母细胞瘤最为多见(15/33,45.5%),其次为肾母细胞瘤(6/33,18.2%)和肝母细胞瘤(4/33,12.1%)。
鉴于99Tcm-MDP骨显像的显像原理,儿童骨外软组织肿瘤摄取99Tcm-MDP的机制主要与肿瘤的坏死和(或)钙化、丰富的血供以及肿瘤本身含有骨样基质有关[14,17-18],但本研究初步发现上述原因引起的99Tcm-MDP的摄取程度并无明显差别。28例患儿的(28/33,84.8%)软组织肿瘤均伴有不同程度的坏死和(或)钙化。由于儿童恶性软组织肿瘤多起源于恶性程度高的幼稚细胞,因此生长快,肿瘤体积大,容易形成缺血性坏死、营养不良性钙化,且钙化的特点有其特异性[18]。结合其他常规影像学检查,本研究收集的儿童恶性软组织肿瘤的钙化多表现为大块状、蛋壳样、片状或絮状钙化。另外,儿童恶性软组织肿瘤的坏死范围大,坏死组织摄取99Tcm-MDP的原因可能与细胞坏死时细胞质内的线粒体、内质网肿胀形成空泡,线粒体基质无定形钙致密物堆积等超微结构的变化有关[19]。若坏死细胞和细胞碎片未被及时清除,后期易吸收钙盐和其他矿物质沉积,则引起营养不良性钙化[20],此时在CT图像上可见明显的钙化。因此,儿童恶性软组织肿瘤摄取99Tcm-MDP的程度明显增高,表现为“+++”的肿瘤16例(48.4%),这与儿童肿瘤恶性程度高,肿瘤钙化的密度高,范围广,形式多样,坏死面积亦较大等特点相符[21-22]。本研究纳入的病例中仅有1例良性软组织肿瘤,为脉管瘤,免疫组化结果提示以血管瘤为主,轻度摄取99Tcm-MDP,我们推测肿瘤摄取99Tcm-MDP的原因与其丰富的血供有关。
以往文献报道对成人患者骨显像时,显影的骨外软组织肿瘤与肿瘤组织病理学的关系结论不一[13]。对于儿童患者,本研究结果显示,母细胞瘤、间叶组织肿瘤和生殖细胞肿瘤摄取99Tcm-MDP程度的差异无统计学意义,提示就儿童肿瘤大体分类而言,儿童软组织肿瘤摄取99Tcm-MDP的程度可能与肿瘤分类无明显相关性,其原因可能与儿童恶性肿瘤的自身特点有关,即无论肿瘤具体的组织起源于何处,儿童恶性肿瘤一般均生长快,体积大,肿瘤本身具有骨样基质,或易形成坏死、钙化。由于本研究纳入的肿瘤患儿仅有15例具有组织分化程度的诊断,且全部为神经母细胞瘤,其中摄取程度为“+++”的8例患儿中分化差型为主的7例(87.5%),但不能就此说明分化差的软组织肿瘤摄取99Tcm-MDP明显高于分化好的肿瘤。因此,儿童骨外软组织肿瘤摄取99Tcm-MDP的程度与肿瘤的不同组织病理学分型、不同分化程度的关系还需要我们再增大样本量进行验证。
总之,在对儿童患者99Tcm-MDP骨显像诊断时,若发现骨外软组织显影,核医学科医师在排除显像剂、显像技术及污染等原因后,可根据浓聚影的部位和浓聚程度对显影的骨外软组织作出初步判断,为进一步确诊提供有效的依据。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 刘思敏、武凤玉负责命题的设计、数据的收集、统计学的分析、论文的初步撰写;蔡海东负责研究项目的设计、统计学方法的提出;郑慧、郁霞青负责数据的收集、统计学的分析;马超、吕中伟、王辉负责论文的审阅与修订。
儿童骨外软组织肿瘤摄取99Tcm-MDP的特点与肿瘤组织病理学的关系
The characteristics of 99Tcm-MDP uptakes in pediatric extraosseous soft tissue tumors on bone scintigraphy and its correlation with tumors histopathology
-
摘要:
目的 探讨肿瘤患儿骨显像中骨外软组织肿瘤摄取99Tcm-亚甲基二膦酸盐(MDP)的特点,以及其与肿瘤组织病理学的关系。 方法 回顾性分析2008年12月至2018年12月在上海交通大学医学院附属新华医院和同济大学附属第十人民医院行骨显像的33例肿瘤患儿的临床资料,其中男患儿21例、女患儿12例,年龄3个月~10岁。根据病理学结果将肿瘤类型分为母细胞瘤、间叶组织肿瘤和生殖细胞肿瘤3大类。根据骨显像等影像学结果,将骨外软组织肿瘤的最高放射性浓聚程度从低到高分为“+”、“++”和“+++”, 分析骨显像的特点及其与肿瘤病理学的关系。软组织肿瘤摄取99Tcm-MDP的多组间比较采用Kruskal-Willis H秩和检验。 结果 33例患儿中母细胞瘤26例(78.8%,包括神经母细胞瘤15例、肾母细胞瘤6例、肝母细胞瘤4例和胰母细胞瘤1例)、间叶组织肿瘤5例(15.2%,包括骨肉瘤肺转移灶3例、恶性肾外横纹肌样瘤1例和左大腿脉管瘤1例)和生殖细胞肿瘤2例(6.0%),软组织肿瘤的3种类型摄取99Tcm-MDP程度的差异无统计学意义(H=1.993,P=0.369)。所有患儿骨外软组织肿瘤骨显像内部特点为钙化、坏死和其他特点(含有骨化基质或实性肿块无明显坏死及钙化),摄取99Tcm-MDP为“+” 的6例(6/33,18.2%)、 “++”的11例(11/33,33.3%)和 “+++”的16例(16/33,48.5%),肿瘤内钙化伴坏死、钙化、坏死和其他原因引起的99Tcm-MDP摄取程度的差异无统计学意义(H=2.313,P=0.315)。不同病理类型的肿瘤摄取99Tcm-MDP为“+”的6例(18.2%,包括母细胞瘤5例、间叶组织肿瘤1例)、“++”的11例(33.3%,包括母细胞瘤9例、间叶组织肿瘤2例)和“+++”的16例(48.5%,包括母细胞瘤12例、间叶组织肿瘤2例、生殖细胞肿瘤2例)。 结论 骨显像时患儿骨外软组织肿瘤摄取99Tcm-MDP多提示为恶性肿瘤,以神经母细胞瘤最常见,其程度与组织病理学分类无明显相关性。 Abstract:Objective This study aimed to explore the characteristics of 99Tcm-methylene diphosphonate (MDP) accumulated in extraosseous soft tissue tumors in children via bone scintigraphy and determine the correlation between tracer uptake and tumor histopathology. Methods A total of 33 pediatric patients with 99Tcm-MDP uptake in extraosseous soft tissue tumors, who underwent bone scintigraphy in Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine and Tenth People's Hospital of Tongji University from December 2008 to December 2018, were retrospectively identified. The patients included 21 male children and 12 female children, ranging in age from 3 months to 10 years. On the basis of histopathology, the extraosseous soft tissue tumors in children were categorized into blastomas, mesenchymal tumors, and germ cell tumors. The highest degree of radioactivity accumulation in focal lesions was classified as “+,” “++,” and “+++” based on the results of bone scan. The features of 99Tcm-MDP uptake in different pathological types of tumors and the correlations between 99Tcm-MDP uptake in soft tissue tumors and tumor pathology were investigated. Rank sum test was performed. Results Among 33 children, there were 26 cases of blastomas (78.8%, including 15 cases of neuroblastoma, 6 cases of Wilms' tumor, 4 cases of hepatoblastoma, and 1 case of pancreatoblastoma). Five cases were mesenchymal tumors (15.2%, including 3 cases of pulmonary metastases from osteosarcoma, 1 case of malignant extrarenal rhabdoid tumor, and 1 case of left thigh vascular tumor). Two cases were germ cell tumors (6.0%). No statistical significant difference was found in the degree of 99Tcm-MDP uptake in 33 pediatric patients with three different types of soft tissue tumors (H=1.993, P=0.369). The main imaging features of 33 cases of extraosseous tissue tumors included calcification, necrosis, and other features. Six cases of 99Tcm-MDP uptake were “+” (6/33, 18.2%), 11 cases were “++” (11/33, 33.3%), and 16 cases were “+++” (16/33, 48.5%). No significant difference in the degree of MDP uptake was found in 33 patients with different reasons causing 99Tcm-MDP accumulation (H=2.313, P=0.315). In terms of different pathological types of tumors, six cases of 99Tcm-MDP uptake were “+” (18.2%, including 5 cases of blastoma and 1 case of mesenchymal tumor). Eleven cases were “++” (33.3%, including 9 cases of blastoma and 2 cases of mesenchymal tumor). Sixteen cases were “+++” (48.5%, including 12 cases of blastoma, 2 cases of mesenchymal tumor, and 2 cases of germ cell tumor). Conclusions During the bone scan, pediatric extraosseous soft tissue tumors with 99Tcm-MDP accumulation mostly indicate malignancy, and neuroblastoma was the most common type. No significant correlation was found in the degree of neoplastic 99Tcm-MDP uptake and the histopathological types in child. -
Key words:
- Child /
- Technetium Tc 99m medronate /
- Bone imaging /
- Soft tissue neoplasms /
- Histopathology
-
图 1 右颈部恶性肾外横纹肌样瘤99Tcm-MDP骨显像及CT图像(男患儿,2岁)
Figure 1. 99Tcm-MDP uptake in malignant extrarenal rhabdoid tumor in the right neck and its corresponding CT image (male, 2 years old)
图 2 左大腿软组织脉管瘤99Tcm-MDP骨显像及CT图像(男患儿,1岁)
Figure 2. 99Tcm-MDP uptake in the left thigh vascular tumor and its corresponding CT image (male, 1 year old)
图 3 左侧腹膜后神经母细胞瘤99Tcm-MDP骨显像及CT图像(男患儿,7岁)
Figure 3. 99Tcm-MDP uptake in neuroblastoma in the left retroperitoneum and its corresponding CT image (male, 7 years old)
表 1 33例摄取99Tcm-MDP的患儿软组织肿瘤的类型和放射性浓聚程度的比较
Table 1. Types of pediatric soft tissue tumors and their degrees of 99Tcm-MDP uptake in 33 children patients
肿瘤分类 软组织肿瘤类型 例数(%) 放射性浓聚程度(例) + ++ +++ 母细胞瘤 神经母细胞瘤 15(45.5) 2 5 8 肾母细胞瘤 6(18.2) 2 2 2 肝母细胞瘤 4(12.1) 0 2 2 胰母细胞瘤 1(3.0) 1 0 0 间叶组织肿瘤 骨肉瘤肺转移灶 3(9.1) 0 1 2 恶性肾外横纹肌样瘤 1(3.0) 0 1 0 左大腿脉管瘤 1(3.0) 1 0 0 生殖细胞肿瘤 生殖细胞肿瘤 2(6.1) 0 0 2 合计 33 6 11 16 注:表中,以病灶区放射性高于正常下肢软组织,低于正常肋骨放射性分布为“+”;等于或高于正常肋骨放射性分布,低于正常胸骨体或脊柱放射性分布为“++”;等于或高于正常胸骨体或脊柱放射性分布为“+++”。MDP:亚甲基二膦酸盐  下载: 导出CSV
下载: 导出CSV
表 2 33例患儿骨外软组织肿瘤中的钙化和坏死的情况 [例(%)]
Table 2. Main imaging features of pediatric extraosseous soft tissue tumors in 33 children patients
浓聚程度 钙化伴坏死 坏死 钙化 其他a 合计 + 0 4(66.7) 1(16.7) 1(16.7) 6 ++ 6(54.5) 0 3(27.3) 2(18.2) 11 +++ 8(50.0) 0 6(37.5) 2(12.5) 16 合计 14 4 10 5 33 注:表中,a:包含骨外软组织肿瘤未见明显坏死及钙化2例(摄取99Tcm-MDP的程度分别为“+”、“++”各1例)及3例含有骨化基质(摄取99Tcm-MDP的程度表现为“++”1例,“+++”2例)的患者。以病灶区放射性高于正常下肢软组织,低于正常肋骨放射性分布为“+”;等于或高于正常肋骨放射性分布,低于正常胸骨体或脊柱放射性分布为“++”;等于或高于正常胸骨体或脊柱放射性分布为“+++”
下载: 导出CSV
-
[1] 王荣福, 安锐, 李亚明, 等. 核医学[M]. 9版. 北京: 人民卫生出版社, 2018: 143−153.
Wang RH, An R, Li YM, et al. Nuclear medcine[M]. 9th ed. Beijing: People's Medical Publishing House, 2018: 143−153.[2] Banezhad F, Ayati N, Toosi FS, et al. Extraosseous accumulation of Technetium-99m-methyl diphosphonate (99mTc-MDP) in a child with all: a case report[J]. Asia Ocean J Nucl Med Biol, 2018, 6(1): 57−60. DOI: 10.22038/aojnmb.2017.9679. [3] Franco A, Henderson PR, McDonough CH. Unusual concentration of Tc-99m methylendiphosphonate in rhabdomyosarcoma[J/OL]. J Radiol Case Rep, 2012, 6(9): 29−34[2020-04-04]. http://www.radiologycases.com/index.php/radiologycases/index. DOI: 10.3941/jrcr.v6i9.1144. [4] Zhao XF, Zhao RF, Wu H. Unexpected pyelonephritis incidentally revealed on 99mTc MDP bone scintigraphy[J]. Clin Nucl Med, 2017, 42(12): 978−979. DOI: 10.1097/RLU.0000000000001860. [5] Doll R, Payne P, Waterhouse J. Cancer incidence in five continents[M]. Berlin: Springer,1966:1-244. [6] 陈跃, 王辉, 杨吉刚, 等. 儿童骨显像操作指南[J]. 中国医学影像技术, 2017, 33(1): 153−156. DOI: 10.13929/j.1003-3289.201611010.
Chen Y, Wang H, Yang JG, et al. Guidelines for pediatric bone imaging[J]. Chin J Med Imaging Technol, 2017, 33(1): 153−156. DOI: 10.13929/j.1003-3289.201611010.[7] 步宏, 李一雷, 来茂德, 等. 病理学[M]. 9版. 北京: 人民卫生出版社, 2018: 100,152.
Bu H, Li YL, Lai MD, et al. Pathology[M]. 9th ed. Beijing: People's Medical Publishing House, 2018: 100,152.[8] Loutfi I, Collier BD, Mohammed AM. Nonosseous abnormalities on bone scans[J]. J Nucl Med Technol, 2003, 31(3): 149−153. [9] Zou YT, Chen Y, Huang ZW, et al. Elevated 99mTc-MDP and 18F-NaF uptake in a bladder stone[J]. Clin Nucl Med, 2016, 41(9): 732−733. DOI: 10.1097/RLU.0000000000001295. [10] 曾德春, 陈跃, 蔡亮, 等. 99mTc-MDP全身骨显像异常骨外软组织摄取分析[J]. 重庆医学, 2016, 45(15): 2073−2074, 2077. DOI: 10.3969/j.issn.1671-8348.2016.15.013.
Zeng DC, Chen Y, Cai L, et al. Analysis of abnormal uptake of extraskeletal soft tissue in 99mTc-MDP whole bone scan[J]. Chongqing Med, 2016, 45(15): 2073−2074, 2077. DOI: 10.3969/j.issn.1671-8348.2016.15.013.[11] Lima MC, Passarelli MC, Dario V, et al. The use of SPECT/CT in the evaluation of heterotopic ossification in para/tetraplegics[J]. Acta Ortop Bras, 2014, 22(1): 12−16. DOI: 10.1590/S1413-78522014000100001. [12] 付占立, 张旭初, 范岩, 等. 99mTc-MDP全身骨显像诊断外伤性骨化性肌炎一例[J]. 中华核医学杂志, 2007, 27(4): 252. DOI: 10.3760/cma.j.issn.2095-2848.2007.04.021.
Fu ZL, Zhang XC, Fan Y, et al. A case of traumatic myositis ossificans diagnosed by 99mTc-MDP whole bone scan[J]. Chin J Nucl Med, 2007, 27(4): 252. DOI: 10.3760/cma.j.issn.2095-2848.2007.04.021.[13] 刘思敏, 左书耀, 王国明, 等. 骨外软组织肿瘤骨显像时显影与组织细胞学类型的关系[J]. 中华核医学与分子影像杂志, 2008, 28(2): 110−112. DOI: 10.3760/cma.j.issn.2095-2848.2008.02.012.
Liu SM, Zuo SY, Wang GM, et al. Relationship between the extraosseous uptake of 99Tcm-MDP by soft tissue tumors and their pathology[J]. Chin J Nucl Med Mol Imaging, 2008, 28(2): 110−112. DOI: 10.3760/cma.j.issn.2095-2848.2008.02.012.[14] Wale DJ, Wong KK, Savas H, et al. Extraosseous findings on bone scintigraphy using fusion SPECT/CT and correlative imaging[J]. AJR Am J Roentgenol, 2015, 205(1): 160−172. DOI: 10.2214/AJR.14.13914. [15] Soundararajan R, Naswa N, Sharma P, et al. SPECT-CT for characterization of extraosseous uptake of 99mTc-methylene diphosphonate on bone scintigraphy[J]. Diagn Interv Radiol, 2013, 19(5): 405−410. DOI: 10.5152/dir.2013.054. [16] Mebarki M, Medjahedi A, Menemani A, et al. Osteosarcoma pulmonary metastasis mimicking abnormal skeletal uptake in bone scan: utility of SPECT/CT[J]. Clin Nucl Med, 2013, 38(10): e392−e394. DOI: 10.1097/RLU.0b013e318266cdcb. [17] Zuckier LS, Freeman LM. Nonosseous, nonurologic uptake on bone scintigraphy: atlas and analysis[J]. Semin Nucl Med, 2010, 40(4): 242−256. DOI: 10.1053/j.semnuclmed.2010.02.003. [18] Hanafy AK, Mujtaba B, Roman-Colon AM, et al. Imaging features of adrenal gland masses in the pediatric population[J/OL]. Abdom Radiol(NY), 2020, 45(4): 964–981[2020-04-04]. https://link.springer.com/journal/261. DOI: 10.1007/s00261-019-02213-x. [19] 步宏, 李一雷, 来茂德. 病理学[M]. 9版. 北京: 人民卫生出版社, 2018: 100−117.
Bu H, Li YL,Lai MD. Pathology[M]. 9th ed. Beijing: People's Medical Publishing House, 2018: 100−117.[20] Verma S, Kumar N, Kheruka SC, et al. Extraosseous 99mTc-methylene diphosphonate uptake on bone scan: unusual scenario[J]. Indian J Nucl Med, 2016, 31(4): 280−282. DOI: 10.4103/0972-3919.190799. [21] Flynt KA, Dillman JR, Davenport MS, et al. Pediatric adrenocortical neoplasms: can imaging reliably discriminate adenomas from carcinomas?[J]. Pediatr Radiol, 2015, 45(8): 1160−1168. DOI: 10.1007/s00247-015-3308-x. [22] Melo-Leite AF, Elias PC, Teixeira SR, et al. Adrenocortical neoplasms in adulthood and childhood: distinct presentation. Review of the clinical, pathological and imaging characteristics[J]. J Pediatr Endocrinol Metab, 2017, 30(3): 253−276. DOI: 10.1515/jpem-2016-0080. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 3090
- HTML全文浏览量: 2122
- PDF下载量: 11