


-
大量循证医学证据表明,核素心肌灌注显像(myocardial perfusion imaging,MPI)在冠心病的诊断、危险分层、存活心肌检测、治疗决策制定、疗效评价、预后评估以及其他多种心脏疾病的诊治中具有重要的临床价值[1]。其中负荷MPI目前被广泛用于临床。目前临床应用的负荷药物有潘生丁、腺苷和多巴酚丁胺等,但都有不同的局限性。前两者不宜应用于慢性阻塞性肺部疾病及Ⅱ度和Ⅲ度房室传导阻滞患者,后者不宜用于高血压患者。瑞加诺生(regadenoson,商品名为Lexiscan)是选择性的腺苷A2A受体激动剂,不仅可以扩张冠状动脉,而且操作方法简单,仅一次静脉推注;较少引起房室传导阻滞和支气管收缩,所以将成为临床较安全的心脏负荷试验药物[2]。本研究比较瑞加诺生注射液与腺苷注射液作为负荷药物行MPI,评价其诊断冠心病的有效性及安全性。
-
选取2017年9月至2018年10月于山西医科大学第一医院心内科住院的疑似冠心病的42名受试者进行回顾性研究。对所有受试者采用完全随机法及开放、阳性药对照设计,阳性药对照选用腺苷注射液(供诊断用)。所有受试者均签署知情同意书后行MPI。采用完全随机法获得药物编号并将受试者分为2组:瑞加诺生组[男性8名、女性9名,年龄(59.83±7.88)岁]和腺苷组[男性12名、女性13名,年龄(56.32±7.34)岁],分别行瑞加诺生和腺苷注射液的静息MPI后再行负荷MPI,检查结束后2周内所有受试者行冠状动脉血管造影(coronary angiography,CAG)检查(检查前2周内已完成CAG检查且没有接受经皮冠状动脉介入治疗的受试者无需重复检查)。本研究获得山西医科大学第一医院药理临床试验伦理委员会的批准(批准号:[2017]伦审字(30)号)。
纳入标准:① 18岁≤年龄≤75岁,性别不限;② 临床确诊或疑似冠心病,但未行经皮冠状动脉介入治疗;③ 受试者理解研究程序,并签署书面知情同意书。排除标准:① 患有支气管哮喘或严重慢性阻塞性肺部疾病;② Ⅱ度或Ⅲ度房室传导阻滞及病窦综合征者;③ 收缩压<90 mm Hg(1 mm Hg=0.133 kPa)和(或)舒张压<60 mm Hg;④ 未控制的重度高血压,收缩压≥180 mm Hg和(或)舒张压≥110 mm Hg;⑤ 负荷MPI检查前停服β受体阻滞剂、硝酸酯类药物的时间小于48 h(不包括硝酸甘油);⑥ 负荷MPI检查前停用双嘧达莫药物的时间小于48 h;⑦ 负荷MPI检查前停用茶碱类药物或含咖啡因及茶碱的饮料的时间小于12 h;⑧ 发生不稳定心绞痛、急性冠状动脉综合征或急性心肌梗死后的时间小于2~4 d;⑨ 受试者对腺苷有过敏反应史;⑩ 患有先天性心脏病、慢性心瓣膜病、心肌病和各种心律失常者。
-
显像仪器为德国SIEMENS公司生产的Symbia T16 SPECT/CT仪。显像剂为99Tcm-MIBI,由北京原子高科股份有限公司生产,放射化学纯度>95%。瑞加诺生注射液由宝利化(南京)制药有限公司生产;腺苷注射液由美国Teva制药工业有限公司生产。瑞加诺生注射液和腺苷注射液均由南京海美生物医药有限公司提供(获得该公司授权)。
-
① 瑞加诺生的方法:单次快速(约10 s)静脉推注5 mL(含0.4 mg)瑞加诺生注射液。注射完毕立即用5 mL生理盐水冲洗后,即刻推注740~1110 MBq(20~30 mCi)的99Tcm-MIBI。② 腺苷的方法:按体重140 μg/kg·min(总量为0.84 mg/kg)匀速静脉输入腺苷,共6 min,输入腺苷3 min时从另一静脉通道推注740~1110 MBq(20~30 mCi)的99Tcm-MIBI。2组受试者全程心电监护,检测心率、心电图和血压,观察受试者的不适症状,记录药物的不良反应。③ 中止标准:典型心绞痛伴明显心电图ST段压低>2 mm或抬高;血压明显降低(收缩压较用药前降低≥20 mm Hg收缩压或<90 mm Hg)伴头晕、恶心、大汗等;血压明显增高[收缩压≥180 mm Hg和(或)舒张压≥110 mm Hg];心电图检查示严重心律失常或Ⅲ度房室传导阻滞;其他受试者不能耐受的症状。
-
所有受试者注射99Tcm-MIBI后20 min进食脂餐,1~1.5 h进行门控心肌显像,配低能高分辨率准直器,能峰140 keV,窗宽±20%,ZOOM 1.45,矩阵64×64,6°/帧,180°采集,每帧采集35 s,门控采集将每个心动周期分为8帧。图像重建采用迭代法,获得心脏短轴、水平长轴和垂直长轴的图像。
-
所有图像均由2位核医学科副主任医师共同讨论判读获得一致意见。图像异常判断标准:连续2个层面在同一部位负荷时放射性核素聚集程度减低或缺损,静息显像改善或恢复正常者,则该节段心肌为缺血性改变;如仍为放射性核素聚集程度的缺损,则为心肌梗死改变;如放射性核素聚集程度缺损部分改善者,则为心肌梗死合并缺血性改变。
-
左、右冠状动脉主支或其一级分支的血管支至少有1支管腔直径狭窄≥50%,则判断为阳性。
-
采用SPSS 17.0软件对数据进行统计学分析。符合正态分布的计量资料以
$\bar x$ ±s表示,组间比较采用两独立样本t检验(方差齐)、配对t检验或方差分析;不符合正态分布的组间比较采用Wilcoxon Z秩和检验。计数资料组间比较采用χ2检验(McNemar检验)或Fisher's确切概率法(样本量<40)。2种方法的一致性检验采用Kappa检验。P<0.05为差异有统计学意义。 -
瑞加诺生组和腺苷组受试者的冠状动脉血管数目分别为51支和75支,2组一般资料的比较,差异均无统计学意义(表1)。17名瑞加诺生组受试者CAG阳性的有10支(19.6%,10/51),其中狭窄≥50%且<75%、狭窄≥75%的患者均为5支(50%);25名腺苷组受试者CAG阳性的有14支(18.7%,14/75),其中狭窄≥50%且<75%、狭窄≥75%的患者分别为6支(42.9%)、8支(57.1%)。瑞加诺生组与腺苷组CAG阳性率及狭窄程度的比较,差异均无统计学意义(Fisher's确切概率法,均P>0.05)。
组别 男性/
女性(例)年龄
(岁)身高
(cm)体重
(kg)体重指数
(kg/cm2)收缩压
(mm Hg)舒张压
(mm Hg)心率
(次/min)高血压
[例(%)]糖尿病
[例(%)]高血脂
[例(%)]腺苷组(n=25) 12/13 56.32±7.34 165.68±6.55 69.08±10.13 25.12±2.92 137.04±16.15 84.04±11.17 64.28±9.42 18(72.00) 5(20.00) 11(44.00) 瑞加诺生组(n=17) 8/9 59.83±7.88 165.56±9.03 67.22±8.33 24.54±2.67 131.67±11.72 80.83±9.76 63.39±11.51 12(70.59) 7(41.12) 7(41.12) 检验值 −0.228a −1.503b 0.052b 0.638b 0.670b 1.201b 0.978b −1.286b −0.371a −1.346a −0.228a P值 0.820 0.141 0.961 0.527 0.506 0.237 0.334 0.206 0.710 0.178 0.740 注:表中,1 mm Hg=0.133 kPa。a为Wilcoxon Z秩和检验;b为t检验 表 1 2组疑似冠心病的受试者的临床资料比较
Table 1. Comparison of clinical characteristics between two groups of subjects with coronary disease
-
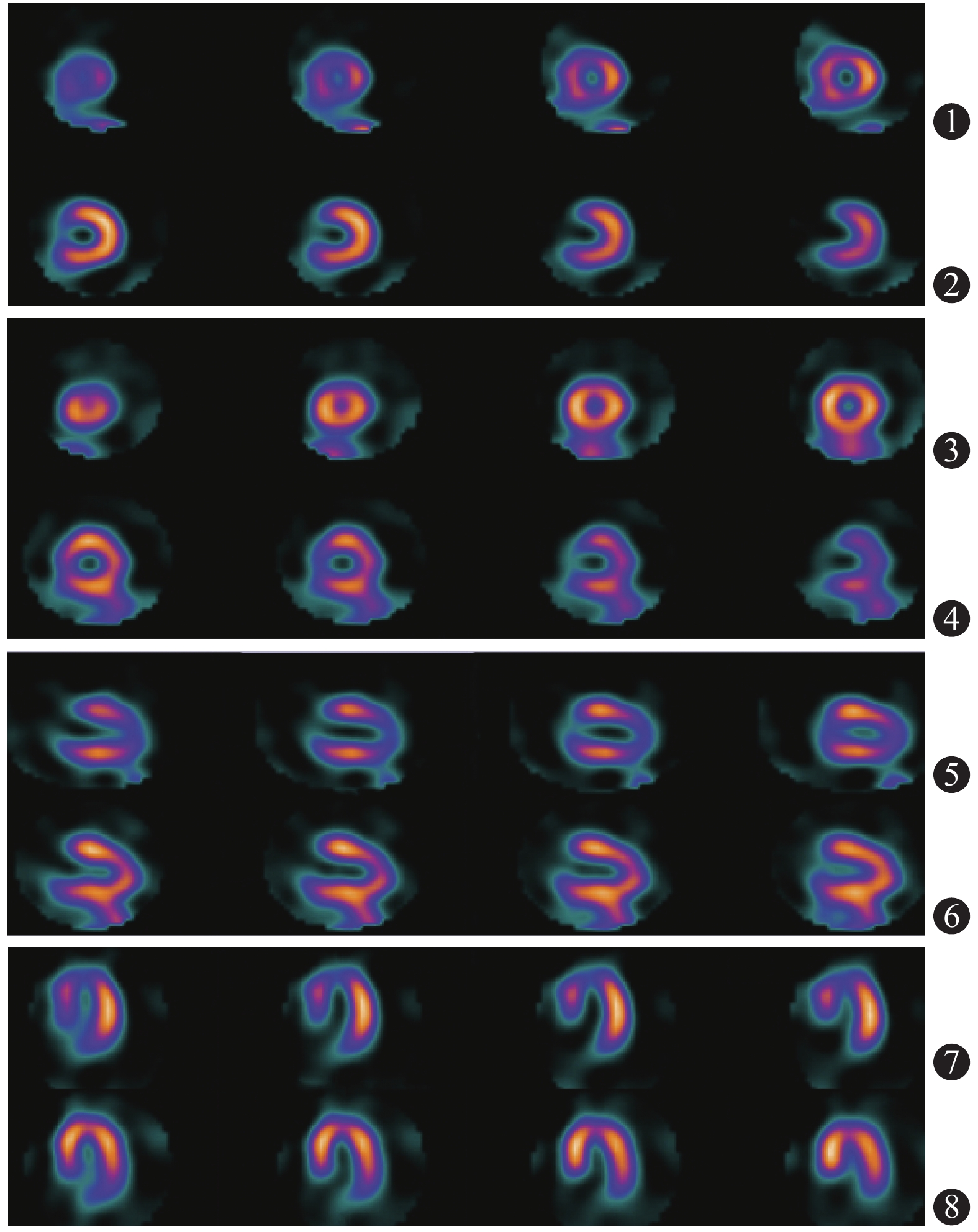
典型病例的瑞加诺生负荷MPI图见图1,显像结果为前壁心尖段及间壁可逆性缺血,CAG显像结果为左前降及近段长病变,最窄处80%~90%狭窄。17名受试者51支血管中,CAG诊断冠状动脉正常41支、异常10支;MPI诊断正常39支、异常12支(表2),2种诊断方法结果的比较,差异无统计学意义(McNemar检验,P=0.727)。以CAG为标准,瑞加诺生组负荷MPI诊断冠心病的灵敏度为70.00%(7/10)、特异度为87.80%(36/41)、阳性预测值为58.33%(7/12),阴性预测值为92.31%(36/39)、准确率为84.31%(43/51)。瑞加诺生负荷MPI与CAG诊断一致性分析,结果显示存在中度一致性(κ=0.537,P<0.001)。
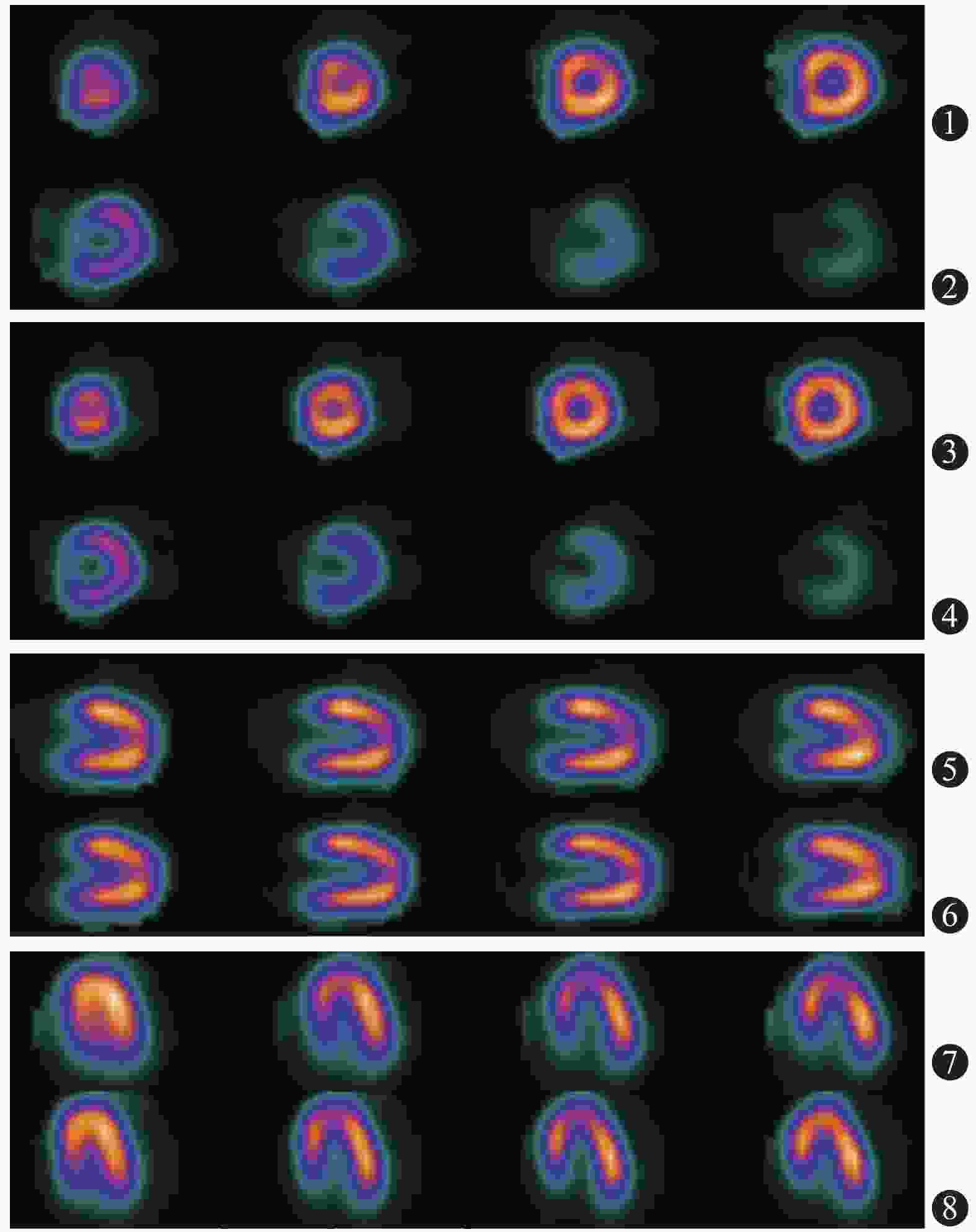
图 1 冠心病患者(女性,62岁)的瑞加诺生负荷心肌灌注显像图
Figure 1. Myocardial perfusion imaging diagram of regadenoson stress in corouary disease patient(female, 62 years old)
CAG 瑞加诺生组(n=17) 腺苷组(n=25) 阳性 阴性 合计 阳性 阴性 合计 阳性 7 3 10 10 4 14 阴性 5 36 41 8 53 61 合计 12 39 51 18 57 75 注:表中,2组分别与CAG诊断结果的比较,差异均无统计学意义(McNemar检验,P=0.727、0.388)。MPI:心肌灌注显像;CAG:冠状动脉血管造影 表 2 2组疑似冠心病受试者的MPI与CAG诊断结果的比 较(例)
Table 2. Comparing the results of myocardial perfusion imaging and coronary angiography of two groups of subjects with suspected coronary disease (case)
-
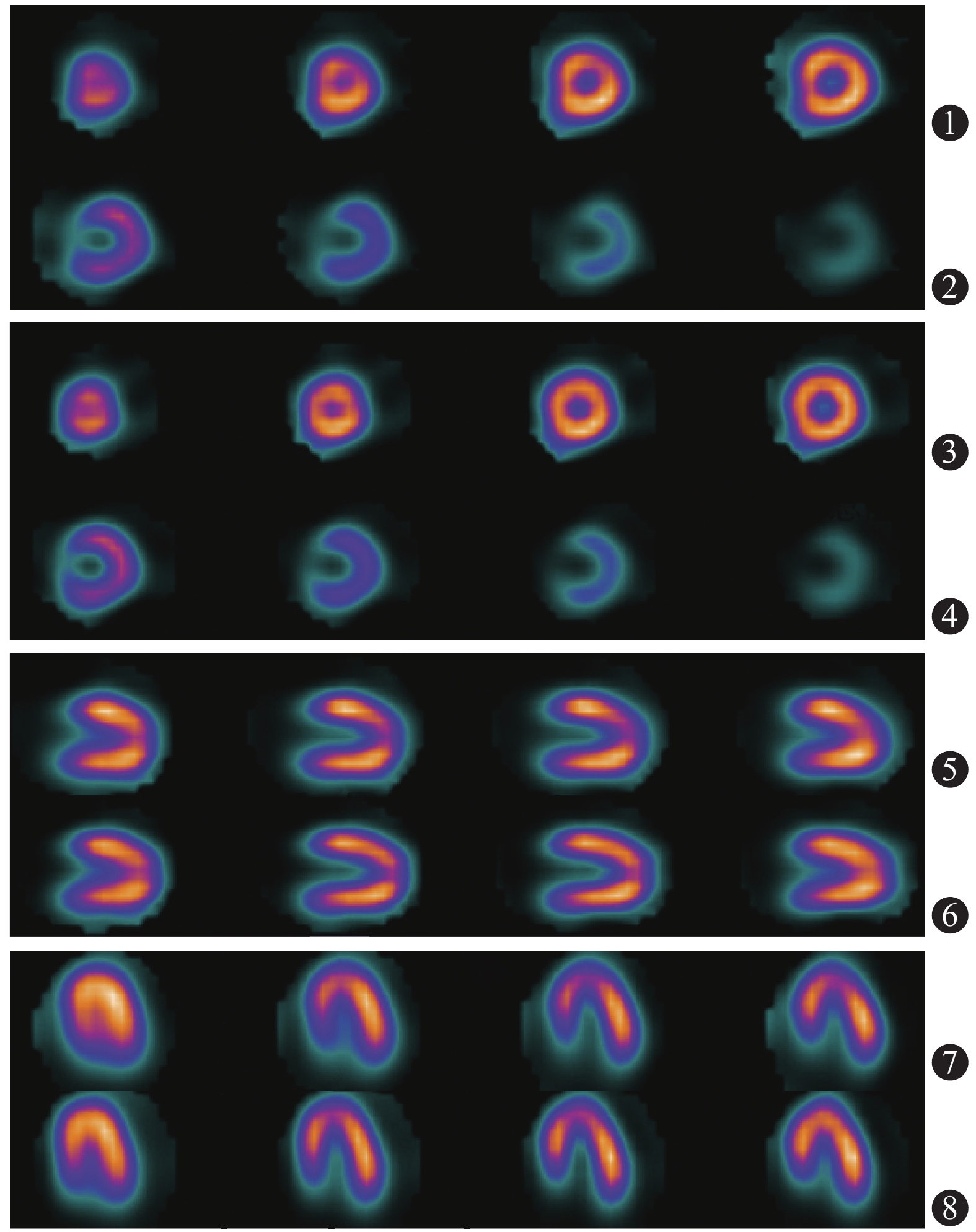
典型病例的腺苷负荷MPI图见图2,显像结果为心尖、前壁的心尖段及间壁可逆性缺血,CAG显像结果为左前降支近段可见80%狭窄。25名受试者75支血管中,CAG诊断冠状动脉正常61支、异常14支;MPI诊断正常57支、异常18支(表2),2种诊断方法结果的比较差异无统计学意义(McNemar检验,P=0.388)。以CAG为标准,腺苷组负荷MPI诊断冠心病的灵敏度为71.43%(10/14)、特异度为86.89%(53/61)、阳性预测值为55.56%(10/18)、阴性预测值为92.98%(53/57)、准确率为84.00%(63/75)。腺苷负荷MPI与CAG诊断一致性分析,结果显示存在中度一致性(κ=0.525,P<0.001)。
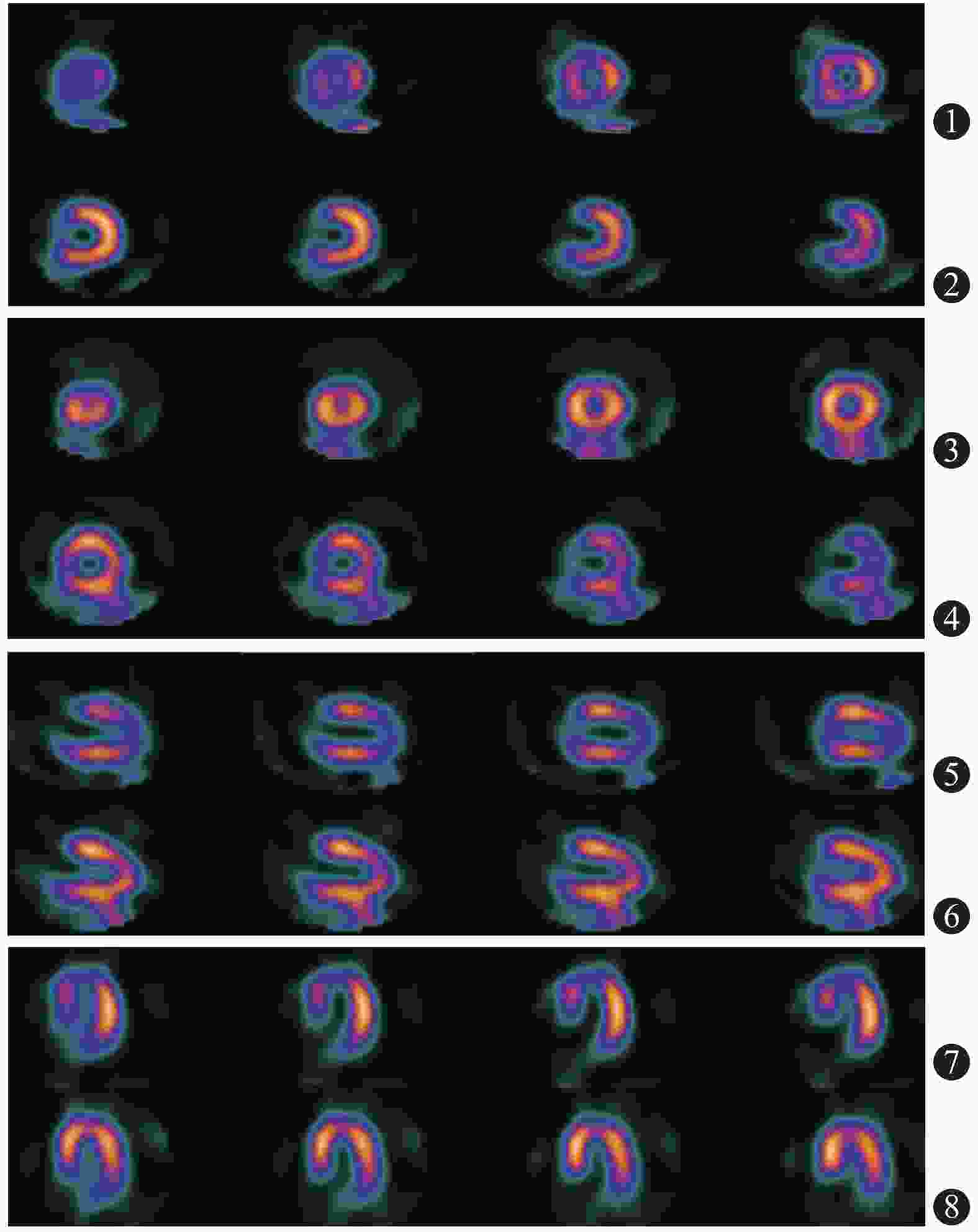
图 2 冠心病患者(男性,51岁)的腺苷负荷心肌灌注显像图 显像结果为心尖、前壁的心尖段及间壁可逆性缺血。图中,第1、2横排为负荷心肌显像短轴图像;第3、4横排为静息心肌显像短轴图像;第5横排为负荷心肌显像垂直长轴图像;第6横排为静息显像垂直长轴图像;第7横排为负荷心肌显像水平长轴图像;第8横排为静息心肌显像水平长轴图像
Figure 2. Myocardial perfusion imaging diagram of adenosine stress in coronary disease patient(male, 51 years old)
-
以CAG为标准,2种诊断方法的灵敏度、特异度、阳性预测值、阴性预测值和准确率的比较差异均无统计学意义(Fisher's确切概率法,均P=1.00)。
-
本试验共发生38例次与研究药物有关的不良反应,主要表现为心悸、胸闷、头晕、胸痛和恶心等。部分受试者同时出现多种不良反应,多数发生在开始用药后1~2 min,症状较轻微,一般停药后很快自行缓解,无需干预,瑞加诺生组与腺苷组均未见严重不良反应。2组药物综合不良反应比较,差异无统计学意义(Fisher's确切概率法,P>0.05)。但瑞加诺生组的不良反应较少见静息脸红、胸痛、呼吸困难和恶心,而腹部不适、头晕头痛较多。其中,2组的比较只有腹部不适的差异有统计学意义(Fisher's确切概率法,P=0.044)(表3)。
组别 总不良反应 脸红 胸痛、胸闷 呼吸困难 头晕、头痛 恶心 腹部不适 心悸 瑞加诺生组(n=17) 74.47 5.88 35.29 23.53 58.82 5.88 35.29 23.53 腺苷组(n=25) 84.00 12.00 48.00 32.00 44.00 20.00 4.00 16.00 Pa值 0.694 0.635 0.530 0.731 0.530 0.374 0.044 0.694 注:表中,a:检验方法为Fisher's确切概率法,无检验值 表 3 2组疑似冠心病受试者药物不良反应发生率的比较(%)
Table 3. Comparison of adverse incidence of two groups of subjects with suspected coronary disease (%)
-
MPI应用于冠心病的诊断、危险度的分层、预后判断及疗效评价等方面已得到了充分肯定和推荐[3-4]。尤其负荷MPI试验是目前诊断冠心病必不可少的手段,大量临床研究结果已证实,负荷MPI正常的患者,心脏不良事件的年发生率<1%,与正常人心脏不良事件的发生率相近[1, 5]。所以,MPI是冠心病患者发生不良心脏事件重要的预测因子。
负荷主要有运动和药物负荷试验。运动负荷试验对于部分老、弱、病、残者常不适用,具有一定局限性。药物负荷试验主要有多巴酚丁胺、潘生丁及腺苷等;多巴酚丁胺的作用机制类似于人体生理的运动负荷试验,但不良反应较多,高血压患者不宜;腺苷作为A2A受体激动剂,通过A2A受体的特异性激活诱导冠状动脉和外周血管扩张,从而导致心肌血流量增加。运动负荷试验目前应用最广泛,但可同时出现心率减慢、房室传导阻滞、心肌收缩力减弱以及交感神经兴奋性降低等不良反应,不宜用于慢性阻塞性肺疾病、哮喘及缓慢型心律失常的患者[6-7]。
国内外学者的临床研究结果显示,腺苷负荷MPI用于诊断冠心病的灵敏度为52.6%~91%、特异度为81.8%~93%、准确率为67%~91%、阳性预测值为76.9%~90.9%、阴性预测值为61.4~84%[8-9]。虽然结果波动范围较大,但均证实腺苷负荷MPI对诊断可疑冠心病心肌缺血有重要意义。
本研究分析了25名疑似冠心病受试者的75支冠状动脉,行腺苷负荷MPI,诊断冠心病的灵敏度为71.43%、特异度为86.89%、阳性预测值为55.56%、阴性预测值为92.98%、准确率为84.00%,与CAG结果比较,一致性为中度(κ=0.525)。其中阳性预测值低于上述国内外报道,可能与本研究的病例数较少及入选受试者CAG阳性的狭窄程度较轻(狭窄<5%占43.6%)有关。
瑞加诺生是一种新型的腺苷A2A受体激动剂,已被美国食品药品管理局(FDA)批准使用于负荷MPI。瑞加诺生能选择性地激活腺苷A2A受体,从而扩张冠状动脉和增加冠状动脉血流量、心肌血流量;其作用维持时间较腺苷长,而且一次静脉推注(静注)即可完成MPI,具有不需持续静注、剂量不需按体重调整、较少引起房室传导阻滞和支气管收缩等优点[10]。
文献报道,瑞加诺生可以用于MPI评价心肌缺血,与腺苷一样其安全性及有效性得到临床研究证实,并在不同性别、年龄、体重指数及糖尿病患者中被证实,而且其耐受性优于腺苷[11]。另外,瑞加诺生负荷MPI与腺苷负荷MPI图像定性及定量指标的结果比较均无显著差异。2组药物的不良反应比较,瑞加诺生总的不良反应显著减少(P=0.015),此外在受试者不良反应耐受性方面,瑞加诺生优于腺苷(P=0.001)[12]。
本研究是国内首次应用瑞加诺生注射液进行负荷MPI,17名受试者51支冠脉血管的MPI结果显示,瑞加诺生负荷MPI诊断冠心病的灵敏度为70.00%、特异度为87.80%、阳性预测值为58.33%、阴性预测值为92.31%、准确率为84.31%;与CAG结果比较,κ=0.537(P<0.001)。各项结果与腺苷MPI比较,2种诊断药物的有效性和安全性评价相似,差异均无统计学意义。这些结果初步证实,在对可疑冠心病的人群行核素MPI时,瑞加诺生在辅助诊断冠心病方面与腺苷具有相似的临床应用价值,可以应用于冠心病的诊断。本研究结果与文献报道的结果一致[11-12]。
本研究中,2组药物总的不良反应对比无明显差异。但瑞加诺生组受试者脸红、胸痛、呼吸困难、恶心等不良反应较少,而腹部不适、头晕头痛较多,其中只有腹部不适的差异有统计学意义,与国外报道相似[11, 13]。
另外,瑞加诺生与腺苷相比,目前已有多项临床研究[2, 14-15]报道,哮喘、慢性阻塞性肺部疾病及慢性肾脏疾病患者可很好地耐受瑞加诺生,这也是瑞加诺生作为负荷显像药物的优势之一。所以该药在今后的应用中可能更安全、范围更广泛。
本研究存在不足之处:试验样本量不够大,随机分组后2组数据有差距,而且未纳入左主干病变;虽然为了减少误差分析是针对每支冠状动脉,并应用了针对样本量少的统计学方法,但仍存在一定的局限性。今后需进行更大样本、更长时间的临床试验,尤其在慢性阻塞性肺部疾病和哮喘患者的临床应用等方面更需进一步验证。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 郭小闪负责试验的设计、研究的实施、数据的采集与分析、论文的撰写;靳春荣负责试验的实施;武志芳、武萍、李莉、陈伟强负责协助完成试验与技术的支持;李思进负责论文的审阅与最终版本的修订。
瑞加诺生负荷心肌灌注显像诊断冠心病的初步临床研究
Regadenoson stress myocardial perfusion imaging for detecting coronary artery disease
-
摘要:
目的 探讨瑞加诺生注射液作为负荷药物行核素心肌灌注显像(MPI)诊断冠心病的有效性及安全性。 方法 选取2017年9月至2018年10月于山西医科大学第一医院住院的疑似冠心病的42名受试者进行回顾性研究。采用完全随机法将受试者分为2组:瑞加诺生组[男性8名、女性9名,年龄(59.83±7.88)岁]和腺苷组[男性12名、女性13名,年龄(56.32±7.34)岁],分别行瑞加诺生和腺苷注射液的静息MPI后再行负荷MPI,之后2周内所有受试者均行冠状动脉血管造影(CAG)检查。以CAG结果为标准,分析2组MPI诊断冠心病的效能并观察不良反应。计量资料的组间比较采用两独立样本t检验、配对t检验或方差分析、Wilcoxon Z秩和检验;计数资料的组间比较采用McNemar检验或Fisher's确切概率法;瑞加诺生和腺苷的MPI检查方法的一致性比较采用Kappa检验。 结果 2组一般资料、CAG阳性率及狭窄程度的比较,差异均无统计学意义(t=−1.503~1.201,Z=−1.346~−0.228,Fisher's确切概率法,均P>0.05)。瑞加诺生负荷MPI诊断冠心病的灵敏度为70.00%(7/10)、特异度为87.80%(36/41)、阳性预测值为58.33%(7/12)、阴性预测值为92.31%(36/39)、准确率为84.31%(43/51);腺苷负荷MPI诊断冠心病的灵敏度为71.43%(10/14)、特异度为86.89%(53/61)、阳性预测值为55.56%(10/18)、阴性预测值为92.98%(53/57)、准确率为84.00%(63/75),2种MPI方法诊断效能的各项指标的比较差异均无统计学意义(Fisher's确切概率法,均P=1.00),其分别与CAG结果比较,均存在中度一致性(κ=0.537、0.525,均P<0.001)。药物不良反应为轻微和暂时的,2组间在脸红、胸痛和胸闷、呼吸困难、头晕和头痛、恶心、心悸等不良反应的比较,差异均无统计学意义(Fisher's确切概率法,均P>0.05),只有腹部不适的差异有统计学意义(Fisher's确切概率法,P=0.044)。 结论 瑞加诺生作为心脏负荷试验药物用于MPI诊断冠心病,与腺苷注射液比较具有相似的有效性及安全性。 Abstract:Objective To investigate the efficacy and safety of regadenoson injection as cardiac stress medicine. It was compared with adenosine injection by using radionuclide myocardial perfusion imaging (MPI) to diagnose coronary disease. Coronary angiography (CAG) was the standard used for this study. Methods Forty-two subjects with suspected coronary heart disease who were admitted in the First Hospital of Shanxi Medical University from September 2017 to October 2018 were retrospectively analyzed. All subjects were randomly divided into two groups, namely, regadenoson group (8 males; 9 females; age: 59.83±7.88 years old) and adenosine group (12 males; 13 females; age: 56.32±7.34 years old). All subjects underwent rest MPI and stress MPI. Regadenoson and adenosine were injected as medicines. All subjects underwent CAG within 2 weeks. The diagnostic efficacy of regadenoson and adenosine were compared with the results of CAG, which was defined as the gold standard. Adverse reactions were also observed for the two drugs. Two sample t-test, paired t-test or analysis of variance, and Wilcoxon Z rank sum test were used to compare measurement data. Two sample McNemar test or Fisher's exact test were used to measure data. Kappa test was used to test the consistency of the two groups. Results There were no statistically significant difference between the two groups of general data, the positive rate and the degree of stenosis (t=−1.503−1.201, Z=−1.346−−0.228, Fisher's exact test, all P>0.05). With the results of CAG as the gold standard, the diagnosis sensitivity of regadenoson MPI was 70.00% (7/10), specificity was 87.80% (36/41), positive predictive value was 58.33% (7/12), negative predictive value was 92.31% (36/39), and accuracy was 84.31% (41/51). The sensitivity of adenosine MPI was 71.43% (10/14), specificity was 86.89% (53/61), positive predictive value was 55.56% (10/18), negative predictive value was 92.98% (53/57), and accuracy was 84.00% (63/75). No obvious statistically significant difference for each value was found between the two drugs (Fisher's exact test, all P=1.00). The consistency was moderate between the two groups of drugs and CAG (κ=0.537, 0.525, respectively, both P<0.001). The side effects were mild and transient. No obvious statistically significant difference (Fisher's exact test, all P>0.05) was found between the two groups in terms of adverse reactions, such as blushing, chest pain, chest tightness, dyspnea, dizziness, headache, nausea, and palpitation. Statistically significant difference was only found for abdominal discomfort (Fisher's exact test, P=0.044). Conclusion Regadenoson injection is similar in terms of efficacy and safety when compared with the injection drug load of adenosine according to the results of myocardial perfusion imaging. -
Key words:
- Coronary disease /
- Myocardial perfusion imaging /
- Regadenoson /
- Adenosine /
- Coronary angiography
-
图 1 冠心病患者(女性,62岁)的瑞加诺生负荷心肌灌注显像图
Figure 1. Myocardial perfusion imaging diagram of regadenoson stress in corouary disease patient(female, 62 years old)
图 2 冠心病患者(男性,51岁)的腺苷负荷心肌灌注显像图 显像结果为心尖、前壁的心尖段及间壁可逆性缺血。图中,第1、2横排为负荷心肌显像短轴图像;第3、4横排为静息心肌显像短轴图像;第5横排为负荷心肌显像垂直长轴图像;第6横排为静息显像垂直长轴图像;第7横排为负荷心肌显像水平长轴图像;第8横排为静息心肌显像水平长轴图像
Figure 2. Myocardial perfusion imaging diagram of adenosine stress in coronary disease patient(male, 51 years old)
表 1 2组疑似冠心病的受试者的临床资料比较
Table 1. Comparison of clinical characteristics between two groups of subjects with coronary disease
组别 男性/
女性(例)年龄
(岁)身高
(cm)体重
(kg)体重指数
(kg/cm2)收缩压
(mm Hg)舒张压
(mm Hg)心率
(次/min)高血压
[例(%)]糖尿病
[例(%)]高血脂
[例(%)]腺苷组(n=25) 12/13 56.32±7.34 165.68±6.55 69.08±10.13 25.12±2.92 137.04±16.15 84.04±11.17 64.28±9.42 18(72.00) 5(20.00) 11(44.00) 瑞加诺生组(n=17) 8/9 59.83±7.88 165.56±9.03 67.22±8.33 24.54±2.67 131.67±11.72 80.83±9.76 63.39±11.51 12(70.59) 7(41.12) 7(41.12) 检验值 −0.228a −1.503b 0.052b 0.638b 0.670b 1.201b 0.978b −1.286b −0.371a −1.346a −0.228a P值 0.820 0.141 0.961 0.527 0.506 0.237 0.334 0.206 0.710 0.178 0.740 注:表中,1 mm Hg=0.133 kPa。a为Wilcoxon Z秩和检验;b为t检验  下载: 导出CSV
下载: 导出CSV
表 2 2组疑似冠心病受试者的MPI与CAG诊断结果的比 较(例)
Table 2. Comparing the results of myocardial perfusion imaging and coronary angiography of two groups of subjects with suspected coronary disease (case)
CAG 瑞加诺生组(n=17) 腺苷组(n=25) 阳性 阴性 合计 阳性 阴性 合计 阳性 7 3 10 10 4 14 阴性 5 36 41 8 53 61 合计 12 39 51 18 57 75 注:表中,2组分别与CAG诊断结果的比较,差异均无统计学意义(McNemar检验,P=0.727、0.388)。MPI:心肌灌注显像;CAG:冠状动脉血管造影
下载: 导出CSV
表 3 2组疑似冠心病受试者药物不良反应发生率的比较(%)
Table 3. Comparison of adverse incidence of two groups of subjects with suspected coronary disease (%)
组别 总不良反应 脸红 胸痛、胸闷 呼吸困难 头晕、头痛 恶心 腹部不适 心悸 瑞加诺生组(n=17) 74.47 5.88 35.29 23.53 58.82 5.88 35.29 23.53 腺苷组(n=25) 84.00 12.00 48.00 32.00 44.00 20.00 4.00 16.00 Pa值 0.694 0.635 0.530 0.731 0.530 0.374 0.044 0.694 注:表中,a:检验方法为Fisher's确切概率法,无检验值
下载: 导出CSV
-
[1] 中华医学会核医学分会, 中华医学会心血管病学分会. 核素心肌显像临床应用指南(2018)[J]. 中华心血管病杂志, 2019, 47(7): 519−527. DOI: 10.3760cma.j.issn.0253-3758.2019.07.003.
Chinese Society of Nuclear Medicine of Chinese Medical Association, Chinese Society of Cardiology of Chinese Medical Association. Guideline for the clinical use of myocardial radionuclide imaging (2018)[J]. Chin J Cardiol, 2019, 47(7): 519−527. DOI: 10.3760cma.j.issn.0253-3758.2019.07.003.[2] Leaker BR, O'Connor B, Hansel TT, et al. Safety of regadenoson, an adenosine A2A receptor agonist for myocardial perfusion imaging, in mild asthma and moderate asthma patients: a randomized, double-blind, placebo-controlled trial[J]. J Nucl Cardiol, 2008, 15(3): 329−336. DOI: 10.1016/j.nuclcard.2008.02.009. [3] Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC committee to revise the 1995 guidelines for the clinical use of cardiac radionuclide imaging)[J]. J AM Coll Cardiol, 2003, 42(7): 1318−1333. DOI: 10.1016/j.jacc.2003.08.011. [4] Gibbons RJ, Abrams J, Chatterjee K, et al. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Chronic Stable Angina)[J]. Circulation, 2003, 107(1): 149−58. DOI: 10.1161/01.cir.0000047041.66447.29. [5] Nakajima K, Nishimura T. Cardiovascular events in Japan. Lessons from the J-ACCESS multicenter prognostic study using myocardial perfusion imaging[J]. Circ J, 2012, 76(6): 1313−1321. DOI: 10.1253/circj.cj-12-0260. [6] 付瑛, 王蒨. 冠心病危险度分层的无创性影像技术研究进展[J]. 心肺血管病杂志, 2014, 33(2): 305−307. DOI: 10.3969/j.issn.1007-5062.2014.02.040.
Fu Y, Wang Q. Advances in noninvasive evaluation in the risk stratification of coronary heart disease using imaging techniques[J]. J Cardio Pulmonary Dis, 2014, 33(2): 305−307. DOI: 10.3969/j.issn.1007-5062.2014.02.040.[7] Henzlova MJ, Duvall WL, Einstein AJ, et al. ASNC imaging guidelines for SPECT nuclear cardiology procedures: stress, protocols, and tracers[J]. J Nucl Cardiol, 2016, 23(3): 606−639. DOI: 10.1007/s12350-015-0387-x. [8] 王丽娟, 李晓鹃, 孙英贤, 等. 腺苷负荷99m 锝-甲氧基异丁基异腈门控心肌灌注显像在冠心病诊断中的价值[J]. 中国循环杂志, 2011, 26(3): 170−173. DOI: 10.3969/j.issn.1000-3614.2011.03.004.
Wang LJ, Li XJ, Sun YX, et al. The clinical value of adenosine stress 99mTc-MIBI gated myocardial perfusion imaging in diagnosis of coronary artery disease[J]. Chin Circ J, 2011, 26(3): 170−173. DOI: 10.3969/j.issn.1000-3614.2011.03.004.[9] Kapur A, Latus KA, Davies G, et al. A comparison of three radionuclide myocardial perfusion tracers in clinical practice: the ROBUST study[J]. Eur J Nucl Med Mol Imaging, 2002, 29(12): 1608−1616. DOI: 10.1007/s00259-002-0998-8. [10] Reyes E. Regadenoson stress for myocardial perfusion imaging[J]. Future Cardiol, 2016, 12(1): 59−67. DOI: 10.2217/fca.15.70. [11] Cerqueira MD, Nguyen P, Staehr P, et al. Effects of age, gender, obesity, and diabetes on the efficacy and safety of the selective A2A agonist regadenoson versus adenosine in myocardial perfusion imaging: integrated ADVANCE-MPI trial results[J]. JACC Cardiovasc Imaging, 2008, 1(3): 307−316. DOI: 10.1016/j.jcmg.2008.02.003. [12] Thomas DM, Minor MR, James KA, et al. Effects of adenosine and regadenoson on hemodynamics measured using cardiovascular magnetic resonance imaging[J]. J Cardiovasc Magn Reson, 2017, 19(1): 96. DOI: 10.1186/s12968-017-0409-8. [13] Vleeming EJ, Lazarenko SV, van der Zant FM, et al. Cardiac displacement during 13N-Aammonia myocardial perfusion PET/CT: comparison between adenosine- and regadenoson-induced stress[J]. J Nucl Med Technol, 2018, 46(2): 114−122. DOI: 10.2967/jnmt.117.199463. [14] Salgado-Garcia C, Jimenez-Heffernan A, Ramos-Font C, et al. Safety of regadenoson in patients with severe chronic obstructive pulmonary disease[J]. Rev Esp Med Nucl Imagen Mol, 2016, 35(5): 283−286. DOI: 10.1016/j.remn.2016.03.005. [15] Gupta A, Bajaj N. Regadenoson use for stress myocardial perfusion imaging in advance chronic kidney disease and dialysis: safe, effective, and efficient[J]. J Nucl Cardiol, 2018, 25(1): 150−152. DOI: 10.1007/s12350-017-1038-1. -

 点击查看大图
点击查看大图
计量
- 文章访问数: 4208
- HTML全文浏览量: 2660
- PDF下载量: 40
