


-
心绞痛是心血管内科常见的一种疾病,该病多发于老年人,会使患者胸腔中央产生压榨性疼痛,并逐步延伸到身体的其他部位,严重影响患者的生活质量[1]。心绞痛可分为稳定型心绞痛(stable angina pectoris,SAP)和非稳定型心绞痛(unstable angina pectoris,UAP)。有研究结果显示,心绞痛患者的预后与冠状动脉内的斑块性质密切相关[2]。因此,可通过对斑块性质的检查分析心绞痛患者的预后。冠状动脉CT血管造影(CT angiography,CTA)是一种无创性的检查方法,其能使血管显影,从而了解冠状动脉狭窄程度,判断斑块性质[3]。在本研究中我们探究了冠状动脉CTA对心绞痛斑块性质及预后的评估价值,以期为临床治疗提供参考。
-
回顾性分析2018年8月1日至2019年7月31日南京市高淳人民医院收治的139例心绞痛患者的临床资料,根据心绞痛分型分为SAP组(n=50)和UAP组(n=89)。纳入标准:均行冠状动脉CTA确诊;SAP组患者符合SAP诊断标准[4],UAP组患者符合UAP诊断标准[5];患者年龄>18周岁者。排除标准:对造影剂过敏者;存在严重肝肾功能不全者;伴有精神性疾病者。本研究获得我院伦理学委员会审核批准,批准文号为GRY201807022,且所有患者均签署了知情同意书。
-
患者于CTA检查前12 h停用致心率加快的药物,并于检查当日测量心率;对心率过快的患者,予以美托洛尔1 mg/kg[阿斯利康药业(中国)有限公司]舌下含服,使心率控制在60~75次/min。
用双筒高压注射器经肘静脉注射碘海醇350 mg I/mL(欧乃派克,美国GE公司)。注射速度为5 mL/s,注射剂量为40~60 mL,对比剂注射完毕后,注射30 mL 0.9%的生理盐水冲管。
使用美国GE公司的Revolution 256排螺旋CT行CTA检查,在整个扫描期间要求患者屏气,并在扫描前嘱咐患者进行呼吸训练。扫描范围自心底至心尖。扫描参数:管电压100 kV,管电流400~650 mA,0.28 s/转,噪声指数20。ROI选定于升主动脉处,触发阈值设为250 HU,延迟3 s触发扫描。增强扫描参数同平扫参数。
对所有患者行1年病情随访,且均无失访。记录患者发生心血管事件的情况,将发生心血管事件定义为预后不良,将未发生心血管事件定义为预后良好。
-
扫描完成后采集40%~50%(收缩期)、70%~80%(舒张期)时相,对数据进行50%基于多模型的迭代重建(ASiR-V)。使用美国GE公司CT机器自带的ADW4.7图像工作站测量斑块的CT值,并评估斑块性质。软斑块:CT值<50 HU;混合斑块:50 HU≤CT值≤130 HU;钙化斑块:CT值>130 HU。由2位有10年以上工作经验的放射科医师独立进行CT图像分析,意见不一致时由2位医师协商确定诊断结果。
-
使用SPSS 22.0软件进行统计学分析。符合正态分布的计量资料用
$\bar x $ ±s表示,组间比较采用两配对样本t检验;计数资料以百分比表示,采用χ2检验进行比较。P<0.05为差异有统计学意义。 -
由表1可知,2组患者在性别、年龄、体重指数间的比较差异均无统计学意义。
组别 男性/女性(例) 年龄(岁) 体重指数(kg/m2) UAP组(n=89) 58/31 65.54±12.26 22.29±1.95 SAP组(n=50) 35/15 64.47±11.85 22.17±2.04 检验值 χ2=0.34 t=0.50 t=0.34 P值 0.56 0.62 0.73 注:表中,UAP:非稳定型心绞痛;SAP:稳定型心绞痛 表 1 2组心绞痛患者一般资料的比较
Table 1. Comparison of general data between the two groups of angina pectoris patients
-
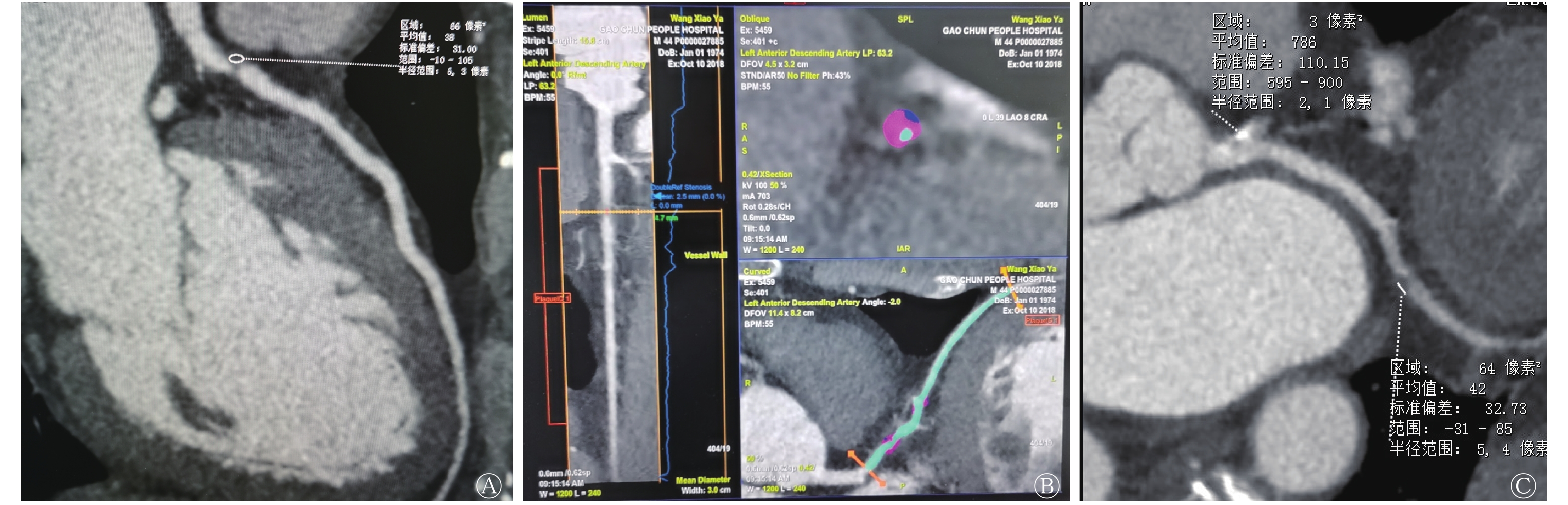
UAP和SAP患者的典型CTA图像见图1。UPA患者的左前降支近段中度狭窄伴软斑块形成,而SAP患者左冠状动脉多发硬斑块。
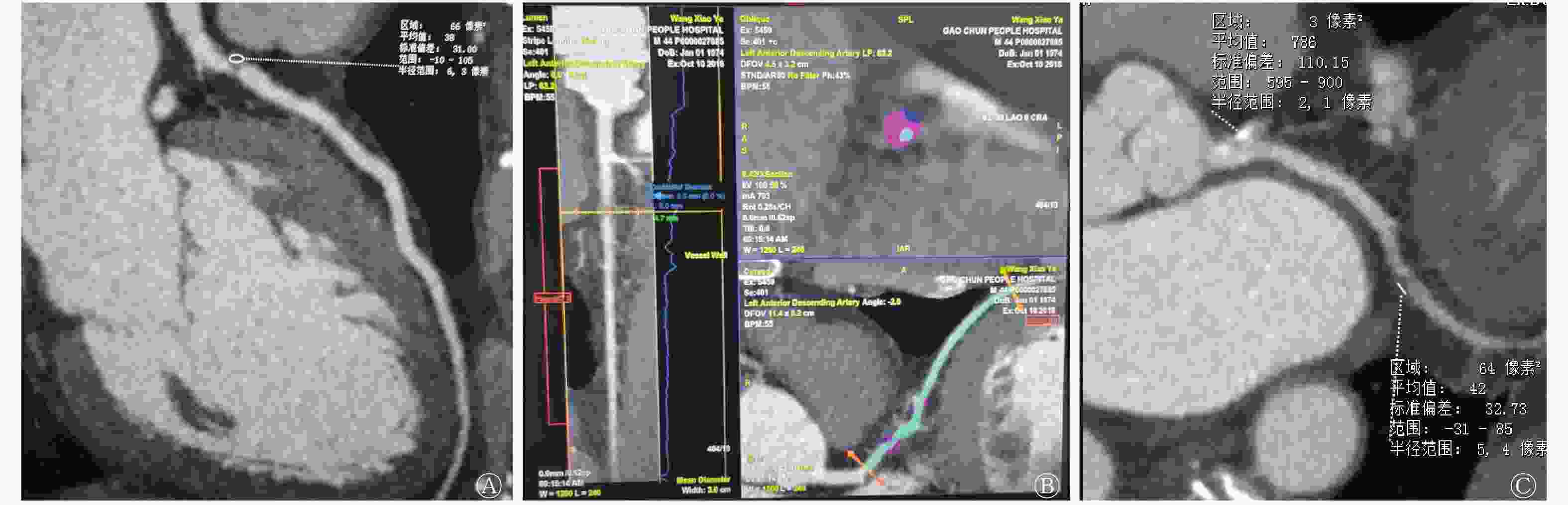
图 1 心绞痛患者的CT血管造影图像
Figure 1. CT angiography in patients with angina pectoris
-
由表2可知,UAP组患者软斑块发生率明显高于SAP组患者,钙化斑块发生率明显低于SAP组患者,且差异均有统计学意义(χ2=28.92、26.06,均P<0.01),2组患者混合斑块的发生率比较,差异无统计学意义。
组别 斑块总数(个) 软斑块[个(%)] 混合斑块[个(%)] 钙化斑块[个(%)] UAP组(n=89) 362 152(41.99) 72(19.89) 138(38.12) SAP组(n=50) 170 31(18.24) 34(20.00) 105(61.76) χ2值 − 28.92 0.00 26.06 P值 − 0.01 0.98 0.01 注:表中,UAP:非稳定型心绞痛;SAP:稳定型心绞痛;−:无此项数据 表 2 2组心绞痛患者不同性质斑块数量的比较
Table 2. Comparison of the number of plaque of different nature between two groups of patients with angina pectoris
-
由表3可知,UAP组的89例患者中,有25例患者发生心血管事件,其中心力衰竭5例、急性心肌梗死5例、UAP反复发作15例;预后不良与预后良好患者混合斑块发生率的比较,差异无统计学意义(χ2=0.00,P>0.05),预后不良患者的软斑块发生率明显高于预后良好患者,差异有统计学意义(χ2=61.29,P<0.05),而钙化斑块发生率明显低于预后良好的患者,差异有统计学意义(χ2=63.75,P<0.05)。SAP组的50例患者中,有5例患者发生心血管事件,其中急性心肌梗死1例、发展为UAP4例;预后不良与预后良好患者混合斑块发生率的比较,差异无统计学意义(χ2=0.00,P>0.05),预后不良患者的软斑块发生率明显高于预后良好患者,差异有统计学意义(χ2=22.57,P<0.05),而钙化斑块发生率明显低于预后良好患者,差异有统计学意义(χ2=15.01,P<0.05)。
组别 例数 斑块总数(个) 软斑块[个(%)] 混合斑块[个(%)] 钙化斑块[个(%)] UAP组 预后良好 64 252 72(28.57)a 50(19.84) 130(51.59)a 预后不良 25 110 80(72.73) 22(20.00) 8(7.27) SAP组 预后良好 45 151 20(13.25)a 30(19.87) 101(66.89)a 预后不良 5 19 11(57.89) 4(21.05) 4(21.05) 注:表中,a:与预后不良相比,差异均有统计学意义(χ2=15.01~63.75,均P<0.05)。UAP:非稳定型心绞痛;SAP:稳定型心绞痛 表 3 2组心绞痛患者不同预后的斑块数量的比较
Table 3. Comparison of the number of plaques with different prognosis between two groups of patients with angina pectoris
-
近年来,随着人们工作压力的增大,心绞痛的发生率越来越高。心绞痛属于冠心病的一种,主要由冠状动脉粥样硬化所导致。根据心绞痛患者病情的严重程度,心绞痛又可分为SAP和UAP。冠状动脉CTA技术是目前临床上常用的一种冠状动脉病变诊断手段,可多视角观察冠状动脉管腔狭窄程度,更为准确地获得斑块的信息,有利于对斑块性质做出判断[6]。有研究结果显示,斑块性质与心绞痛的发生和预后密切相关[7],因此本研究采用冠状动脉CTA技术对不同类型心绞痛患者的斑块性质及其与预后的关系进行分析,结果显示斑块性质与心绞痛的发生和预后具有一定的关系,与上述研究结果相符。
杨文兵等[8]研究发现,不同类型心绞痛患者的斑块性质存在差异。软斑块主要由大量的脂质及少量的平滑肌组成,内无胶原纤维,因此易发生破裂[9]。混合斑块含脂质成分较软斑块少,且含有丰富的纤维和钙质,其稳定性适中[10]。钙化斑块由钙质组成,其硬度大,表面裂隙较少,斑块较稳定,不易产生破裂情况[11]。郭长磊[12]研究发现,SAP患者以钙化斑块为主,UAP患者以软斑块为主,2组患者的混合斑块数量比较,差异无统计学意义。本研究结果发现,UAP组患者的软斑块发生率明显高于SAP组患者,钙化斑块发生率明显低于SAP组患者,2组患者混合斑块发生率的比较差异无统计学意义,与上述研究结果相符。
斑块的不稳定性是导致心血管疾病发生的关键,斑块破裂后易形成血栓,继而引发一系列心血管疾病,不利于患者的预后。本研究中UAP组预后不良患者的软斑块发生率明显高于预后良好患者,钙化斑块发生率明显低于预后良好患者,SAP组预后不良患者的软斑块发生率明显高于预后良好患者,钙化斑块发生率明显低于预后良好患者。这提示软斑块是患者发生心血管事件的关键。通过分析可知,软斑块表面存在多处裂隙,导致血小板在裂隙处聚集,同时患者体内脂代谢紊乱会使软斑块表面裂隙增宽,致使更多的血小板堆积,引发血栓,进而导致患者发生严重心血管事件,不利于患者的预后[13]。而钙化斑块表面裂隙少,硬度大,不易发生破裂,使患者病情处于相对稳定状态。尹小花等[14]研究发现,混合斑块会提高心血管风险的发生率,但本研究中2组预后不良及预后良好患者的混合斑块发生率间的差异均无统计学意义,这说明混合斑块对心绞痛的预后无重要影响,与上述试验结果不符,因此关于混合斑块的性质还需要我们进一步研究。
综上所述,软斑块和钙化斑块与心绞痛患者发生心血管事件密切相关,而冠状动脉CTA能有效评估斑块性质,预测患者的预后。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 傅晓明负责研究命题的提出与设计、方法的建立、现场的试验、数据的获取与分析、论文的起草与修订;李宝新负责研究命题的提出与设计、方法的建立、论文的审阅与修订。
冠状动脉CT血管造影对心绞痛斑块性质及预后的评估价值分析
Value of coronary CT angiography in evaluating the nature and prognosis of angina pectoris plaque
-
摘要:
目的 探究冠状动脉CT血管造影(CTA)对心绞痛斑块性质及预后的评估价值。 方法 回顾性分析2018年8月1日至2019年7月31日南京市高淳人民医院收治的139例心绞痛患者的临床资料,根据心绞痛分型分为稳定型心绞痛(SAP)组(n=50)和非稳定型心绞痛(UAP)组(n=89)。所有患者均行CTA,比较2组患者的斑块性质情况并分析斑块性质与预后的关系。2组计量资料的比较采用配对t检验;计数资料的比较采用χ2检验。 结果 UAP组患者软斑块发生率明显高于SAP组患者[41.99%(152/362)对18.24%(31/170),χ2=28.92,P<0.01],钙化斑块发生率明显低于SAP组患者[38.12%(138/362)对61.76%(105/170),χ2=26.06,P<0.01]。UAP组的89例患者中,有25例患者发生心血管事件,其中心力衰竭5例、急性心肌梗死5例、UAP反复发作15例;预后不良患者的软斑块发生率明显高于预后良好患者[72.73%(80/110)对28.57%(72/252),χ2=61.29,P<0.05],而钙化斑块发生率明显低于预后良好的患者[7.27%(8/110)对51.59%(130/252),χ2=63.75,P<0.05]。SAP组的50例患者中,有5例患者发生心血管事件,其中急性心肌梗死1例、发展为UAP4例;预后不良患者的软斑块发生率明显高于预后良好患者[57.89%(11/19)对13.25%(20/151),χ2=22.57,P<0.05],而钙化斑块发生率明显低于预后良好患者[21.05%(4/19)对66.89%(101/151),χ2=15.01,P<0.05]。 结论 冠状动脉CTA能有效评估斑块性质,预测患者的预后情况。 -
关键词:
- 冠状动脉疾病 /
- 斑块,动脉粥样硬化 /
- 计算机体层摄影血管造影术 /
- 心绞痛 /
- 预后
Abstract:Objective To explore the value of coronary CT angiography in evaluating the nature and prognosis of angina pectoris plaque. Methods A retrospective analysis of 139 patients with angina pectoris treated in Gaochun People's Hospital of Nanjing was conducted from 1 August 2018 to 31 July 2019. According to their clinical data, they were divided into stable angina pectoris (SAP, n=50) group and unstable angina pectoris (UAP, n=89) group. The plaque properties of the two groups were compared, and the relationship between their plaque properties and prognosis was analyzed. The measurement data of the two groups were compared by paired t test. The count data were compared by χ2 test. Results The rate of soft plaque detection in the UAP group was significantly higher than that in SAP group (41.99% (152/362) vs. 18.24% (31/170)), and the rate of calcified plaque detection was significantly lower than that in the SAP group (38.12% (138/362) vs. 61.76% (105/170)) (χ2=28.92 and 26.06, both P<0.01). Among the 89 patients in the UAP group, 25 patients had cardiovascular events, including 5 cases of heart failure, 5 cases of acute myocardial infarction, and 15 cases of recurrent UAP. The rate of soft plaque detection in patients with poor prognosis in the UAP group was significantly higher than that in patients with good prognosis (72.73% (80/110) vs. 28.57% (72/252), χ2=61.29, P<0.05), and the rate of calcified plaque detection was significantly lower than that in patients with good prognosis (7.27% (8/110) vs. 51.59% (130/252), χ2=63.75, P<0.05). Among the 50 patients in the SAP group, 5 patients had cardiovascular events, including 1 case of acute myocardial infarction and 4 cases of UAP. The rate of soft plaque detection in patients with poor prognosis in the SAP group was significantly higher than that in patients with good prognosis (57.89% (11/19) vs. 13.25% (20/151), χ2=22.57, P<0.05), and the rate of calcified plaque detection was significantly lower than that in patients with good prognosis (21.05% (4/19) vs. 66.89% (101/151), χ2=15.01, P<0.05). Conclusion Coronary CT angiography can effectively assess the nature of plaque and predict the prognosis of patients. -
表 1 2组心绞痛患者一般资料的比较
Table 1. Comparison of general data between the two groups of angina pectoris patients
组别 男性/女性(例) 年龄(岁) 体重指数(kg/m2) UAP组(n=89) 58/31 65.54±12.26 22.29±1.95 SAP组(n=50) 35/15 64.47±11.85 22.17±2.04 检验值 χ2=0.34 t=0.50 t=0.34 P值 0.56 0.62 0.73 注:表中,UAP:非稳定型心绞痛;SAP:稳定型心绞痛  下载: 导出CSV
下载: 导出CSV
表 2 2组心绞痛患者不同性质斑块数量的比较
Table 2. Comparison of the number of plaque of different nature between two groups of patients with angina pectoris
组别 斑块总数(个) 软斑块[个(%)] 混合斑块[个(%)] 钙化斑块[个(%)] UAP组(n=89) 362 152(41.99) 72(19.89) 138(38.12) SAP组(n=50) 170 31(18.24) 34(20.00) 105(61.76) χ2值 − 28.92 0.00 26.06 P值 − 0.01 0.98 0.01 注:表中,UAP:非稳定型心绞痛;SAP:稳定型心绞痛;−:无此项数据
下载: 导出CSV
表 3 2组心绞痛患者不同预后的斑块数量的比较
Table 3. Comparison of the number of plaques with different prognosis between two groups of patients with angina pectoris
组别 例数 斑块总数(个) 软斑块[个(%)] 混合斑块[个(%)] 钙化斑块[个(%)] UAP组 预后良好 64 252 72(28.57)a 50(19.84) 130(51.59)a 预后不良 25 110 80(72.73) 22(20.00) 8(7.27) SAP组 预后良好 45 151 20(13.25)a 30(19.87) 101(66.89)a 预后不良 5 19 11(57.89) 4(21.05) 4(21.05) 注:表中,a:与预后不良相比,差异均有统计学意义(χ2=15.01~63.75,均P<0.05)。UAP:非稳定型心绞痛;SAP:稳定型心绞痛
下载: 导出CSV
-
[1] Kloner RA, Chaitman B. Angina and its management[J]. J Cardiovasc Pharmacol Ther, 2017, 22(3): 199−209. DOI: 10.1177/1074248416679733. [2] 邵静, 朱晓萌. 不稳定型心绞痛患者血管紧张素转换酶基因多态性与中医证型及冠状动脉斑块性质的关系[J]. 中医杂志, 2015, 56(19): 1671−1674. DOI: 10.13288/j.11-2166/r.2015.19.014.
Shao J, Zhu XM. The relationship between angiotensin converting enzyme gene polymorphism, TCM syndrome and coronary artery plaque characteristic in patients with unstable angina pectoris[J]. J Tradit Chin Med, 2015, 56(19): 1671−1674. DOI: 10.13288/j.11-2166/r.2015.19.014.[3] 王建刚, 席建堂, 李劲松, 等. 心绞痛患者冠脉CT血管造影与颈动脉粥样硬化的相关性分析[J/OL]. 中西医结合心血管病杂志: 电子版, 2015, 3(20): 109−111[2019-11-17]. http://qikan.cqvip.com/Qikan/Article/Detail?id=666960194. DOI: 10.16282/j.cnki.cn11-9336/r.2015.20.06.
Wang JG, Xi JT, Li JS, et al. Correlation analysis of coronary angiography and carotid atherosclerosis in patients with angina pectoris[J/OL]. Cardiovasc Dis J Integr (Electron Ed), 2015, 3(20): 109−111[2019-11-17]. http://qikan.cqvip.com/Qikan/Article/Detail?id=666960194. DOI: 10.16282/j.cnki.cn11-9336/r.2015.20.06.[4] 王安璐, 罗静, 于美丽, 等. 基于陈可冀院士血瘀证辨证方法治疗冠心病稳定性心绞痛的实用性随机对照研究[J]. 中国中西医结合杂志, 2017, 37(10): 1174−1180. DOI: 10.7661/j.cjim.20170908.369.
Wang AL, Luo J, Yu ML, et al. Pragmatic randomized controlled trial on treating stable angina pectoris of coronary heart disease based on Chen Ke-ji's pattern identification methods of blood-stasis syndrome[J]. Chin J Integr Tradit West Med, 2017, 37(10): 1174−1180. DOI: 10.7661/j.cjim.20170908.369.[5] 胡元会, 贾秋蕾, 孟昊, 等. 冠心病不稳定型心绞痛患者血瘀证与外周血血小板微粒膜蛋白表达的相关性[J]. 中医杂志, 2017, 58(4): 321−324. DOI: 10.13288/j.11-2166/r.2017.04.013.
Hu YH, Jia QL, Meng H, et al. Correlation of syndrome of blood stasis and the expressions of peripheral blood platelet microparticle membrane protein in patients with coronary heart disease unstable angina pectoris[J]. J Tradit Chin Med, 2017, 58(4): 321−324. DOI: 10.13288/j.11-2166/r.2017.04.013.[6] 沈洁云, 王忠敏, 陈克敏. 冠状动脉斑块的CT血管造影评价[J]. 中国医学计算机成像杂志, 2016, 22(1): 97−100.
Shen JY, Wang ZM, Chen KM. CT angiographic evaluation of coronary artery plaque[J]. Chin Comput Med Imag, 2016, 22(1): 97−100.[7] Gu H, Gao Y, Hou ZH, et al. Prognostic value of coronary atherosclerosis progression evaluated by coronary CT angiography in patients with stable angina[J]. Eur Radiol, 2018, 28(3): 1066−1076. DOI: 10.1007/s00330-017-5073-8. [8] 杨文兵, 查云飞, 阳朝晖, 等. 冠脉CTA评估冠状动脉斑块性质及其与炎症分子、MMPs/TIMPs的相关性[J]. 海南医学院学报, 2017, 23(21): 2929−2932, 2936. DOI: 10.13210/j.cnki.jhmu.20171011.008.
Yang WB, Zha YF, Yang ZH, et al. Coronary plaque property evaluation by coronary CTA and its correlation with inflammatory olecules and MMPs/TIMPs[J]. J Hainan Med Univ, 2017, 23(21): 2929−2932, 2936. DOI: 10.13210/j.cnki.jhmu.20171011.008.[9] Hu XY, Zhang W, Zhao NR, et al. Low- to high-density lipoprotein cholesterol ratio followed by coronary computed tomography angiography improves coronary plaque classification accuracy[J/OL]. Oncotarget, 2017, 9(7): 7727−7738[2019-11-17]. https://pubmed.ncbi.nlm.nih.gov/29484147. DOI: 10.18632/oncotarget.23558. [10] 王蓉, 孙凯. 冠状动脉CT诊断斑块性病变的无创影像学进展[J]. 国际放射医学核医学杂志, 2017, 41(6): 449−451. DOI: 10.3760/cma.j.issn.1673-4114.2017.06.012.
Wang R, Sun K. Uninvasive imaging of coronary artery CT diagnosis of plaque lesions[J]. Int J Radiat Med Nucl Med, 2017, 41(6): 449−451. DOI: 10.3760/cma.j.issn.1673-4114.2017.06.012.[11] 汤艳萍, 李令建. 64排螺旋CT与选择性冠状动脉造影评价急性冠状动脉综合征患者易损斑块形态、成分及大小的价值对比研究[J]. 临床放射学杂志, 2016, 35(8): 1181−1185. DOI: 10.13437/j.cnki.jcr.2016.08.010.
Tang YP, Li LJ. Comparative study on the value of 64 slice spiral CT and selective coronary angiography in patients with ACS plaque morphology, composition and size[J]. J Clin Radilolgy, 2016, 35(8): 1181−1185. DOI: 10.13437/j.cnki.jcr.2016.08.010.[12] 郭长磊. 冠脉CTA评估心绞痛患者斑块性质及其与心血管事件的相关性研究[J]. 中国CT和MRI杂志, 2018, 16(12): 62−64. DOI: 10.3969/j.issn.1672-5131.2018.12.020.
Guo CL. Plaque properties of patients with angina pectoris evaluated by coronary CTA and their correlation with cardiovascular events[J]. Chin J CT MRI, 2018, 16(12): 62−64. DOI: 10.3969/j.issn.1672-5131.2018.12.020.[13] Vergallo R, Porto I, D'Amario D, et al. Coronary atherosclerotic phenotype and plaque healing in patients with recurrent acute coronary syndromes compared with patients with long-term clinical stability: an in vivo optical coherence tomography study[J/OL]. JAMA Cardiol, 2019, 4(4): 321−329[2019-11-17]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6484796. DOI: 10.1001/jamacardio.2019.0275. [14] 尹小花, 徐荣, 程韬, 等. 冠状动脉CT血管造影联合心肌应变预测冠状动脉斑块患者发生主要不良心脏事件的价值研究[J]. 中国医学装备, 2017, 14(9): 61−66. DOI: 10.3969/J.ISSN.1672-8270.2017.09.017.
Yin XH, Xu R, Cheng T, et al. A research on the value of CCTA combined with 4D-STE for prognosticating MACE of patients with coronary plaque[J]. China Med Equip, 2017, 14(9): 61−66. DOI: 10.3969/J.ISSN.1672-8270.2017.09.017. -

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 3501
- HTML全文浏览量: 2393
- PDF下载量: 11
