


-
泌尿系统结石是泌尿外科的一种常见病,其患者数量在泌尿外科住院患者中高居榜首[1]。泌尿系统结石在临床上表现为血尿、肾绞痛和尿路梗阻。一般输尿管管腔较细,引起的梗阻程度多较重,容易导致进行性肾脏损害;肾盂容积较大,早期肾盂压力增高可代偿,暂不影响肾脏功能,肾小球滤过率(glomerular filtration rate,GFR)早期可无变化,但如果不能及时解除梗阻,可能会出现尿路感染和肾功能衰竭,甚至危及生命[2]。99Tcm-DTPA肾动态显像较传统的血清肾功能检查可以更早地发现肾功能异常,在了解肾脏的形态和血流灌注等情况的同时,还可以计算分肾的GFR,具有灵敏度高、重复性好和安全无创等优点,是目前了解肾功能最好的方法之一[3-5]。本研究通过99Tcm-DTPA肾动态显像对单侧肾积水患者健侧肾代偿能力进行研究,可更好地评价单侧肾积水患者的肾功能情况,为临床医师选择治疗方案及对疾病疗效的预测提供帮助。
-
回顾性分析2016年1月1日至2019年7月31日天津医科大学第二医院泌尿外科收治的257例单侧肾积水患者的临床资料,其中男性149例、女性108例,年龄12~87(52.84±14.23)岁;患肾为左肾者123例、右肾者134例;结石位于肾盂者101例、位于输尿管者156例。
纳入标准:①经腹部超声初次确诊有且仅有一侧上尿路结石并发肾积水;②仅患有肾结石或输尿管结石;③具有完整的腹部超声、放射性核素肾动态显像资料,且以上2种检查均在一周内完成。在选定时间段内多次行放射性核素肾动态显像的患者,选取其首次检查结果进行统计。
排除标准:①患有肾结石合并输尿管结石;②合并其他泌尿系统疾病;③短时间内使用过中草药、氨基糖苷类及含碘造影剂等肾毒性药物。
所有患者均签署了知情同意书。本研究符合《赫尔辛基宣言》的原则。
-
显像仪器为美国GE公司的双探头 Infinia Hawkeye 4型SPECT仪,显像剂为北京原子高科医药有限公司提供的99Tcm-DTPA,放射化学纯度>95%。患者检查前3 天不可做强化CT或肾盂输尿管造影,检查当日早晨停服降压药。于显像前30 min饮水300~500 mL,检查前排空膀胱。采集前对满针注射器进行计数。患者取仰卧位,经肘静脉“弹丸”式注射99Tcm-DTPA 185~370 MBq (5~10 mCi),注射后立即以患者双肾为视野中心进行动态采集。采集条件:低能高分辨率准直器,能峰140 keV,窗宽20%。肾血流灌注显像:1 s/帧,共60 s;肾功能动态显像:60 s/帧,共20 min。采集结束后,再对空针注射器进行计数。
-
由2名有10年以上工作经验的核医学医师利用ROI技术勾画双肾轮廓及本底,计算机自动生成双肾时间-放射性曲线,并通过Gates法计算经体表面积标准化的GFR。意见不一致时,由1名有20年以上工作经验的医师进行指导,最终结果取平均值。将检查所得的健侧肾GFR与《核医学诊断与治疗规范》[6]中单侧肾的GFR正常值上限(63.5 mL/min)进行比较,得出健侧肾GFR的代偿率(%)。健侧肾的GFR代偿率(%)=(健侧肾的GFR−单侧肾的GFR正常值上限)/单侧肾的GFR正常值上限×100%。
-
记录所有患者的性别、年龄、肾积水位置、肾受损程度、肾结石位置、肾积水程度,并进行分组。其中按照年龄将患者分为4组,①≤30岁;②30岁<年龄≤40岁;③40岁<年龄≤50岁;④>50岁。按照腹部超声影像提示的肾积水程度[7]将患者分为3组 ,①轻度肾积水组:超声提示肾盂肾盏变钝;②中度肾积水组:超声示肾盂肾盏杯口完全消失;③重度肾积水组:超声提示肾脏体积明显增大,肾实质明显变薄或不能显示,失去正常形态,肾盂肾盏呈明显囊袋状扩张改变。按照肾动态显像结果分析患侧肾的GFR[8],即患侧肾的受损程度,将患者分为5组,①近无功能组:GFR<10 mL/min,肾实质几乎未见显像剂聚集;②重度损伤组:10 mL/min≤GFR<20 mL/min,肾实质显像剂聚集明显减少;③中度损伤组:20 mL/min≤GFR<30 mL/min,肾脏影像欠清晰,肾实质显像剂聚集中度减少;④轻度损伤组:30 mL/min≤GFR<40 mL/min肾脏影像较清晰,肾实质显像剂聚集略减少;⑤正常组:GFR≥40 mL/min,肾实质显像剂聚集及排泄较迅速。
-
采用SPSS 23.0软件对数据进行统计学分析。符合正态分布的计量资料用
$\bar x $ ±s表示,健侧肾与患侧肾GFR的比较采用两独立样本t检验(方差齐);偏态分布的计量资料用M(P25,P75)表示,并采用Mann-Whitney U 检验和Kruskal-Wallis检验对影响健侧肾代偿能力的因素进行分析。P<0.05为差异有统计学意义。 -
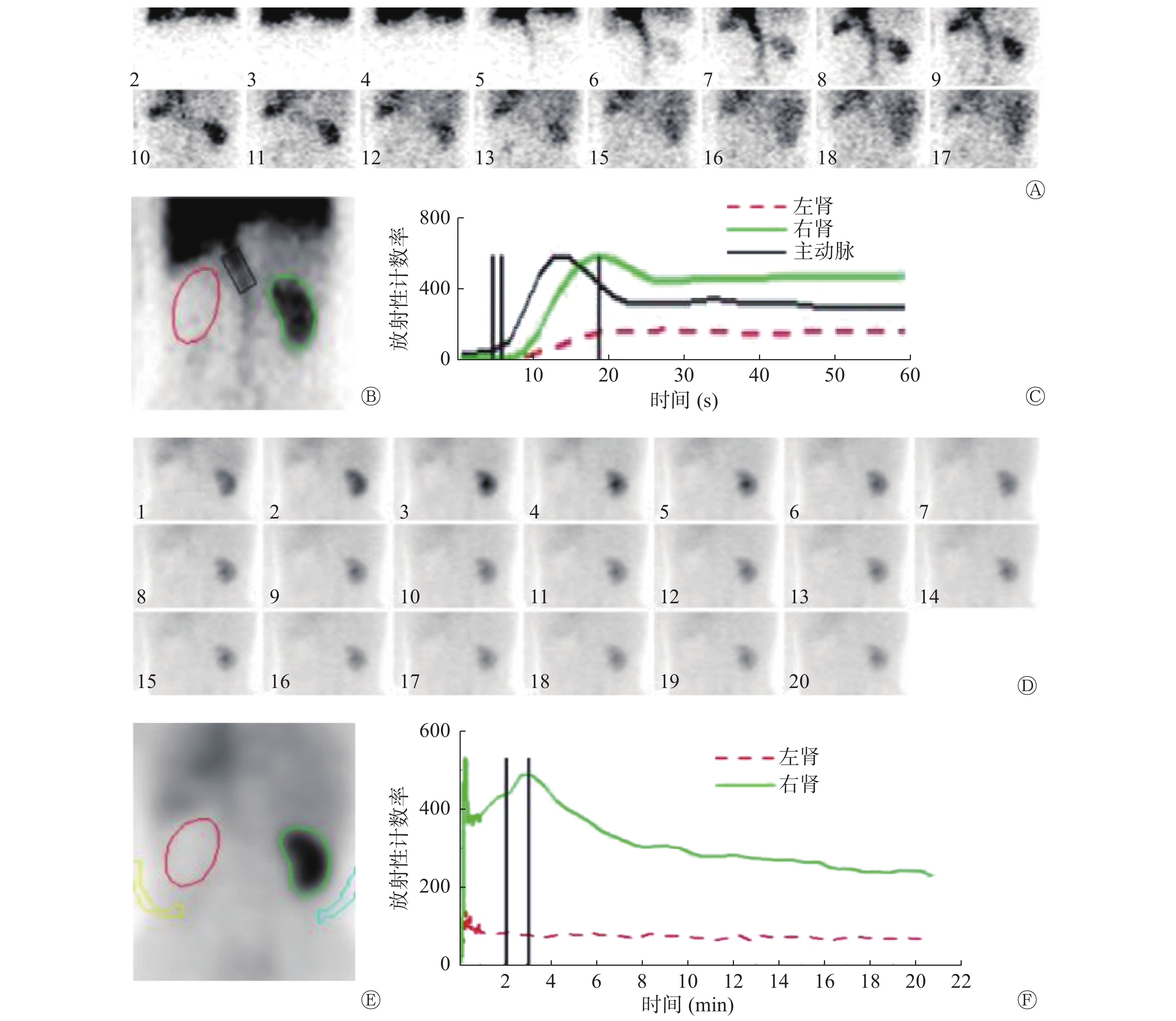
患者的99Tcm-DTPA肾动态显像结果显示,健侧肾血流灌注曲线大致正常,位置和体积大致正常,形态规则、影像清晰,肾实质聚集及排泄较迅速;患侧肾血流灌注及肾实质显像剂摄取多呈不同程度的减低,均未见明显排泄(图1)。经放射性核素肾动态显像检查后测得患者的患侧肾的GFR为(28.60±15.13)mL/min、健侧肾的GFR为(63.17±15.74)mL/min、总的GFR为(92.94±24.46)mL/min。患侧肾的GFR明显低于健侧肾的GFR,且差异有统计学意义(t=25.39,P<0.001)。
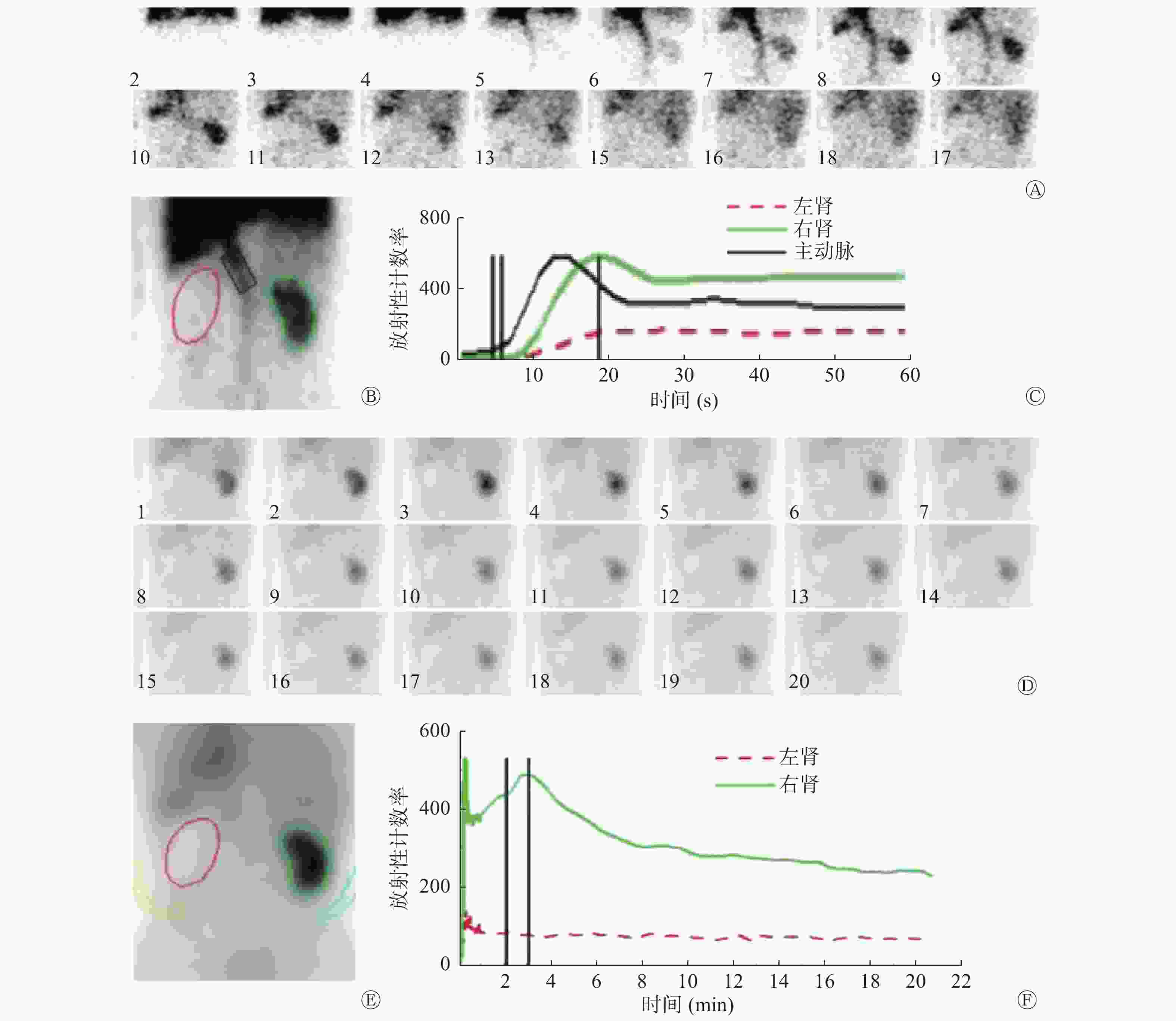
图 1 左侧输尿管结石伴肾积水患者(女性,61岁)的99Tcm-DTPA肾动态显像图
Figure 1. 99Tcm-DTPA renal dynamic imaging of left ureteral stones with hydronephrosis patient (female, 61 years old)
-
患者健侧肾的GFR较GFR正常值上限存在不同程度的增高,存在代偿情况,GFR代偿率为9.54%(−5.94%,26.45%)。由表1可知,患者不同年龄和患侧肾不同的积水程度对健侧肾的GFR的代偿率有影响,且差异均有统计学意义(χ2=47.32、12.71,均P<0.01)。且随着年龄的增长,健侧肾的代偿能力呈下降趋势;随着患侧肾积水程度的加重,健侧肾的GFR代偿能力增强。患者健侧肾的GFR代偿率不受患侧肾受损程度、肾积水位置、肾结石位置和性别的影响,其差异均无统计学意义。
影响因素 例数 健侧肾的GFR代偿率[%,M(P25,P75)] 检验值 P值 年龄 ≤30岁 21 19.62( 8.89,30.38) χ2=47.32 <0.01 30岁<年龄≤40岁 26 16.07(− 7.59,36.53) 40岁<年龄≤50岁 51 6.36(−15.24,24.85) >50岁 159 −9.92(−21.26, 4.69) 肾积水程度 轻度肾积水 55 −8.80(−19.97,6.43) χ2=12.71 <0.01 中度肾积水 79 −3.51(−17.45,7.09) 重度肾积水 123 5.53(−7.21,24.85) 肾受损程度 近无功能 25 1.37(−16.64,35.37) χ2=4.34 0.36 重度损伤 63 −1.92(−19.70,12.54) 中度受损 54 −1.36(−14.57,12.46) 轻度受损 53 −2.91(−17.01,11.72) 正常 62 5.81(−10.85,13.68) 肾积水位置 左肾 123 −0.27(−14.60,14.79) Z=−0.51 0.68 右肾 134 −0.88(−15.79,12.77) 肾结石位置 肾盂 101 −3.87(−20.37, 9.21) Z=−1.62 0.10 输尿管 156 −1.55(−16.50,16.96) 性别 男 149 1.45(−14.68,16.07) Z=−1.41 0.16 女 108 −1.36(−16.20, 9.31) 注:表中,GFR:肾小球滤过率 表 1 不同因素分组的257例单侧肾积水患者健侧肾GFR的代偿率
Table 1. GFR compensation rate in healthy kidney of different factor groups of 257 case of unilateral hydronephrosis
-
肾积水是由泌尿系统梗阻引起的肾盂肾盏扩张和尿液潴留。本研究讨论的病例为泌尿系统结石引起的单侧肾积水,根据结石大小、位置、梗阻时间等情况的不同,肾积水程度会有所不同。肾积水时,由于尿液淤滞,有时可能导致尿路感染,使原有结石体积增大,梗阻进一步加重,形成恶性循环。及时发现肾功能的异常并早期治疗对单侧肾积水患者尤为重要。本研究通过99Tcm-DTPA肾动态显像对单侧肾积水患者的肾功能进行分析,结果发现患侧肾的GFR明显低于健侧肾的GFR。Yang等[9]利用白兔建立输尿管结石模型,并通过肾动态显像观察双侧肾脏大小和GFR的变化,得出梗阻肾脏体积增大,且随着时间延长患侧肾的GFR逐渐下降的结论。肾积水对肾功能有不同程度的影响,若不能及时解除梗阻,纠正肾积水,会导致肾功能严重受损,诱发感染,甚至会危及生命[10-11]
林小敏等[12]认为,术前检查时健侧肾的GFR及总的GFR的降低是术后肾功能不全的独立危险因素,术前行肾动态显像检查尤为重要。其实,当一侧肾脏受到损伤时,对侧肾功能会代偿性增高[13]。这可能是因为对侧肾的肾小管和肾小球代偿性肥大,并通过代偿性肾小球超滤来维持肾功能,但从长远看,这些补偿性适应机制可能会导致高血压和肾脏损伤[14]。及时了解健侧肾代偿能力的影响因素,对于选择手术方式及预防术后肾功能损伤具有重要意义。
本研究通过核素肾动态显像对影响健侧肾代偿能力的因素进行分析,结果发现大多数患者健侧肾的GFR存在不同程度的代偿性增高,且健侧肾代偿能力受患者年龄及患侧肾的积水程度的影响。孝晨等[15]认为,非老年人群残余肾的GFR会出现30%~40%的代偿性增高。崔静等[16]的研究结果显示,肾脏的代偿能力与年龄有关,与性别、不同病因及患侧肾是否经手术切除无关。尤超等[17]则认为,随着年龄的增长,GFR代偿性增高程度会逐渐降低,具体的代偿能力还应该结合年龄进行综合分析。本研究结果与上述研究结论基本一致,在治疗复杂单侧肾积水时,如需切除患侧肾,可根据以上因素对患者残留肾的预后进行评估,减少术后肾功能不全的发生。
Eskild-Jensen等[18]建立猪的单侧肾积水模型以观察其对侧肾的代偿功能,在最初的4周即使患侧肾的GFR明显降低,但对侧肾的GFR与对照组无差异。在第12周时,对侧肾的GFR较对照组明显增高,然而第24周时,对侧肾的GFR再次与对照组无显著差异。单侧肾积水患者健侧肾的代偿情况可能与肾积水的持续时间有关,然而本研究为回顾性分析,对患者患病时间不能准确了解,这可能对最终结果造成影响。设计前瞻性研究,细化健侧肾的GFR代偿功能的影响因素,对治疗后的患者进行随访是下一步的研究方向。
综上,放射性核素肾动态显像能够评价分肾的GFR,还能获得分肾的血流灌注及排泄等情况,在肾脏疾病的诊疗过程中,相比血清肾功能检查能够更早地发现肾功能的异常[11]。通过放射性核素肾动态显像研究单侧肾积水患者健侧肾代偿能力的影响因素,能够更好地为单侧肾积水患者的诊治及预后评估提供依据。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 李亚男负责资料的收集、相关文献的查阅、论文的撰写;张遵城负责论文思路的设计、修改意见的提出;董华负责论文的修订。
99Tcm-DTPA肾动态显像对单侧肾积水患者健侧肾代偿功能的研究
Study of 99Tcm-DTPA renal dynamic imaging on the compensatory capacity of contralateral kidney in patients with unilateral hydronephrosis
-
摘要:
目的 探讨99Tcm-二亚乙基三胺五乙酸(99Tcm-DTPA)肾动态显像在评价单侧肾积水患者健侧肾代偿功能中的应用。 方法 回顾性分析2016年1月至2019年7月天津医科大学第二医院收治的257例单侧肾积水患者的临床资料,其中男性149例、女性108例,年龄12~87(52.84±14.23)岁。所有患者均行99Tcm-DTPA肾动态显像,并通过Gates法计算患者分肾及总的肾小球滤过率(GFR)。按照患者的肾积水程度、患肾受损程度、肾结石位置、患肾位置、性别和年龄进行分组。将各组的健侧肾与单侧肾的GFR正常值上限作比较,计算患者健侧肾的GFR的代偿率(%)。健侧肾与患侧肾的GFR的比较采用两独立样本t检验。患者健侧肾代偿能力的影响因素分析采用Mann-Whitney U 检验及Kruskal-Wallis检验。 结果 所有患者的患侧肾的GFR为(28.60±15.13) mL/min,健侧肾的GFR为(63.17±15.74) mL/min,总的GFR为(92.94±24.46) mL/min。患侧肾的GFR明显低于健侧肾的GFR,且差异有统计学意义(t=25.39,P<0.001)。患者健侧肾的GFR存在不同程度的代偿性增高,其代偿率为9.54%(−5.94%,26.45%)。患者不同年龄和患侧肾积水程度对健侧肾的GFR的代偿率有影响,且差异均有统计学意义(χ2=47.32、12.71,均P<0.01);患侧肾受损程度、肾脏积水位置、肾结石位置和性别对健侧肾的GFR代偿率无影响,且差异均无统计学意义(χ2=4.34,Z=−0.51、−1.62、−1.41,均P>0.05)。 结论 99Tcm-DTPA肾动态显像可以更好地评估单侧肾积水患者健侧肾代偿能力,能够为单侧肾积水患者的诊治及预后评估提供依据。 -
关键词:
- 肾小球滤过率 /
- 肾盂积水;放射性核素显像 /
- 代偿功能 /
- 二亚乙基三胺五乙酸
Abstract:Objective To investigate the application of 99Tcm-diethylene-triaminepentaaccetic acid (99Tcm-DTPA) dynamic renal imaging in evaluating the compensatory function of healthy kidneys in patients with unilateral hydronephrosis. Methods A total of 257 cases of unilateral hydronephrosis admitted to the Second Hospital of Tianjin Medical University from January 2016 to July 2019 were retrospectively analyzed. They included 149 males and 108 females, aged 12~87 (52.84±14.23) years. All patients underwent 99Tcm-DTPA renal dynamic imaging, and their glomerular filtration rate (GFR) was counted using the Gates method. They were also grouped in accordance with the degree of hydronephrosis, the degree of renal impairment, gender, age, and etiology. The GFR compensation rate (%) of the uninfected kidney in different groups was calculated. The GFR of both kidneys was compared using independent sample t-test. The influencing factors of the compensatory ability were analyzed using the Mann-Whitney U and Kruskal-Wallis tests. Results The GFR of the affected kidney was (28.60±15.13) mL/min, while that of the contralateral kidney was (63.17±15.74) mL/min, and the total GFR was (92.94±24.46) mL/min. The GFR of the affected kidney was significantly lower than that of the contralateral kidney (t=25.39, P<0.001). Varying degrees of compensatory increase were observed in the GFR of the uninfected kidney, the GFR compensation rate was 9.54% (−5.94%, 26.45%). Statistically significant differences were also found in the GFR compensation rate of the contralateral kidney among patients of different ages and degrees of hydronephrosis (χ2=47.32, 12.71, both P<0.01). No statistically significant difference was found in the GFR compensation rate of the contralateral kidney among patients with different degrees of renal damage on the affected side, the location of hydronephrosis, the location of the stones, and gender (χ2=4.34, Z=−0.51, −1.62, −1.41, all P>0.05). Conclusion Using renal dynamic imaging to study the factors affecting the compensatory ability of the contralateral kidney in patients with unilateral hydronephrosis could further provide a basis for the diagnosis, treatment, and prognostic evaluation of these patients. -
图 1 左侧输尿管结石伴肾积水患者(女性,61岁)的99Tcm-DTPA肾动态显像图
Figure 1. 99Tcm-DTPA renal dynamic imaging of left ureteral stones with hydronephrosis patient (female, 61 years old)
表 1 不同因素分组的257例单侧肾积水患者健侧肾GFR的代偿率
Table 1. GFR compensation rate in healthy kidney of different factor groups of 257 case of unilateral hydronephrosis
影响因素 例数 健侧肾的GFR代偿率[%,M(P25,P75)] 检验值 P值 年龄 ≤30岁 21 19.62( 8.89,30.38) χ2=47.32 <0.01 30岁<年龄≤40岁 26 16.07(− 7.59,36.53) 40岁<年龄≤50岁 51 6.36(−15.24,24.85) >50岁 159 −9.92(−21.26, 4.69) 肾积水程度 轻度肾积水 55 −8.80(−19.97,6.43) χ2=12.71 <0.01 中度肾积水 79 −3.51(−17.45,7.09) 重度肾积水 123 5.53(−7.21,24.85) 肾受损程度 近无功能 25 1.37(−16.64,35.37) χ2=4.34 0.36 重度损伤 63 −1.92(−19.70,12.54) 中度受损 54 −1.36(−14.57,12.46) 轻度受损 53 −2.91(−17.01,11.72) 正常 62 5.81(−10.85,13.68) 肾积水位置 左肾 123 −0.27(−14.60,14.79) Z=−0.51 0.68 右肾 134 −0.88(−15.79,12.77) 肾结石位置 肾盂 101 −3.87(−20.37, 9.21) Z=−1.62 0.10 输尿管 156 −1.55(−16.50,16.96) 性别 男 149 1.45(−14.68,16.07) Z=−1.41 0.16 女 108 −1.36(−16.20, 9.31) 注:表中,GFR:肾小球滤过率  下载: 导出CSV
下载: 导出CSV
-
[1] 叶章群, 刘浩然. 泌尿系结石的诊断治疗进展[J]. 临床外科杂志, 2017, 25(2): 85−88. DOI: 10.3969/j.issn.1005-6483.2017.02.001.
Ye ZQ, Liu HR. Progress in diagnosis and treatment of urinary calculi[J]. J Clin Suerg, 2017, 25(2): 85−88. DOI: 10.3969/j.issn.1005-6483.2017.02.001.[2] Shoag J, Halpern J, Goldfarb DS, et al. Risk of chronic and end stage kidney disease in patients with nephrolithiasis[J]. J Urol, 2014, 192(5): 1440−1445. DOI: 10.1016/j.juro.2014.05.117. [3] 董华, 张遵城, 董萍, 等. 重度肾积水手术前后 99mTc-DTPA肾动态显像的临床价值[J]. 山东医药, 2011, 51(20): 77−78. DOI: 10.3969/j.issn.1002-266X.2011.20.039.
Dong H, Zhang ZC, Dong P, et al. The clinical value of 99mTc-DTPA renal dynamic imaging before and after the operation of severe hydronephrosis[J]. Shandong Med J, 2011, 51(20): 77−78. DOI: 10.3969/j.issn.1002-266X.2011.20.039.[4] 张遵城, 郑妙瑢, 董萍. 核素肾动态显像对2型糖尿病患者肾功能的研究[J]. 中华内分泌代谢杂志, 2000, 16(6): 363. DOI: 10.3760/j.issn:1000-6699.2000.06.007.
Zhang ZC, Zheng MR, Dong P. Radionuclide renal dynamic for renal function study in patients with type 2 diabetes mellitus[J]. China J Endocrinol Metab, 2000, 16(6): 363. DOI: 10.3760/j.issn:1000-6699.2000.06.007.[5] Wang C, Gao C, Maimaiti W, et al. The features of technetium-99m-DTPA renal dynamic imaging after severe unilateral ureteral obstruction in adult rabbits[J/OL]. PLoS One, 2020, 15(8): e237443[2019-09-09]. https://www.researchgate.net/publication/343754626_The_features_of_technetium-99m-DTPA_renal_dynamic_imaging_after_severe_unilateral_ureteral_obstruction_in_adult_rabbits. DOI:10.1371/journal.pone.0237443. [6] 中华人民共和国卫生部医政司. 核医学诊断与治疗规范[M]. 北京: 科学出版社, 1997: 186.
Department of Medical Administration, Ministry of Health of the People's Republic of China. Nuclear medicine diagnosis and treatment norms[M]. Beijing: Science Press, 1997: 186.[7] 黄晓红, 蒋宁一, 卢献平, 等. 99mTc-DTPA 肾动态显像对泌尿系结石合并肾积水患者肾功能的评价[J]. 实用医学杂志, 2006, 22(13): 1519−1520. DOI: 10.3969/j.issn.1006-5725.2006.13.020.
Huang XH, Jiang NY, Lu XP, et al. Evaluation of renal function with 99mTc-DTPA renal dynamic imaging in patients with urinary calculi and hydronephrosis[J]. J Pract Med, 2006, 22(13): 1519−1520. DOI: 10.3969/j.issn.1006-5725.2006.13.020.[8] 蒋宁一, 刘雄英, 胡莹莹, 等. 99mTc-DTPA肾动态显像对IVP不显影患肾功能的评价[J]. 中国临床医学影像杂志, 2007, 18(7): 479−481. DOI: 10.3969/j.issn.1008-1062.2007.07.008.
Jiang NY, Liu XY, Hu YY, et al. Evaluation of 99mTc-DTPA renal dynamic imaging on renal function of patients without IVP[J]. J China Clin Med Imaging, 2007, 18(7): 479−481. DOI: 10.3969/j.issn.1008-1062.2007.07.008.[9] Yang Q, Wang C, Gao C, et al. Does baseline renal function always decrease after unilateral ureteral severe obstruction? -experimental validation and novel findings by Tc-99m diethylene triamine pentaacetate acid (DTPA) dynamic renal scintigraphy[J]. Quant Imaging Med Surg, 2019, 9(8): 1451−1465. DOI: 10.21037/qims.2019.07.09. [10] Sternberg KM, Pais VM, Larson T, et al. Is hydronephrosis on ultrasound predictive of ureterolithiasis in patients with renal colic?[J]. J Urol, 2016, 196(4): 1149−1152. DOI: 10.1016/j.juro.2016.04.076. [11] Nuraj P, Hyseni N. The diagnosis of obstructive hydronephrosis with color doppler ultrasound[J]. Acta infor Med, 2017, 25(3): 178−181. DOI: 10.5455/aim.2017.25.178-181. [12] 林小敏, 唐明灯, 倪雷春. 99Tcm-DTPA肾动态显像在根治性肾切除术中的应用价值[J]. 国际放射医学核医学杂志, 2017, 41(5): 331−334. DOI: 10.3760/cma.j.issn.1673-4114.2017.05.005.
Lin XM, Tang MD, Ni LC. Application value of 99Tcm-DTPA renal dynamic imaging in radical nephrectomy[J]. Int J Radiat Med Nucl Med, 2017, 41(5): 331−334. DOI: 10.3760/cma.j.issn.1673-4114.2017.05.005.[13] Fong D, Denton KM, Moritz KM, et al. Compensatory responses to nephron deficiency: adaptive or maladaptive?[J]. Nephrology (Carlton), 2014, 19(3): 119−128. DOI: 10.1111/nep.12198. [14] McArdle Z, Schreuder MF, Moritz KM, et al. Physiology and pathophysiology of compensatory adaptations of a solitary functioning kidney[J]. Front Physiol, 2020, 11: 725. DOI: 10.3389/fphys.2020.00725. [15] 孝晨, 傅茜, 刘龙山, 等. 不同性别、年龄活体供肾代偿能力的比较[J]. 肾脏病与透析肾移植杂志, 2012, 21(1): 14−56. DOI: 10.3969/j.issn.1006-298X.2012.01.003.
Xiao C, Fu X, Liu LS, et al. Compensation of graft kidney function from living related donors in different age and gender[J]. Chin J Nephrol Dialysis Transplant, 2012, 21(1): 14−56. DOI: 10.3969/j.issn.1006-298X.2012.01.003.[16] 崔静, 任振泰, 武新宇, 等. 留存肾肾小球滤过率代偿情况及影响因素分析[J]. 中华核医学与分子影像杂志, 2016, 36(1): 59−62. DOI: 10.3760/cma.j.issn.2095-2848.2016.01.014.
Cui J, Ren ZT, Wu XY, et al. Reference values for glomerular filtration rate in patients with solitary kidney and multifactor analy-sis[J]. Chin J Nucl Med Mol Imaging, 2016, 36(1): 59−62. DOI: 10.3760/cma.j.issn.2095-2848.2016.01.014.[17] 尤超, 高永举, 崔静. 留存肾功能正常者99mTc-DTPA显像参数正常值的建立[J]. 郑州大学学报: 医学版, 2018, 53(1): 68−71. DOI: 10.13705/j.issn.1671-6825.2017.04.121.
You C, Gao YJ, Cui J. Normal reference of 99mTc-DTPA renal dynamic imaging parameters of compensatory residual kidney[J]. J Zhengzhou Univ (Med Sci), 2018, 53(1): 68−71. DOI: 10.13705/j.issn.1671-6825.2017.04.121.[18] Eskild-Jensen A, Jacobsen L, Christensen H, et al. Renal function outcome in unilateral hydronephrosis in newborn pigs. II. Function and volume of contralateral kidneys[J]. J Urol, 2001, 165(1): 205−209. DOI: 10.1097/00005392-200101000-00059. -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 2810
- HTML全文浏览量: 1828
- PDF下载量: 18
