



-
近年来脑卒中的发病率逐年升高,因其可导致患者瘫痪、失能甚至死亡等严重后果,已成为威胁人们健康的重大疾病。脑动脉粥样硬化是引起脑卒中的主要和直接原因。已有研究结果证明,吸烟是导致动脉粥样硬化的独立危险因素[1]。因烟雾中含有的有害化学成分尼古丁、焦油、碳氧化物等可刺激血管收缩、损伤血管内皮细胞、暴露内皮下胶原组织、激活血小板,导致血栓形成;同时可以导致脂质代谢紊乱,促进内皮下脂质沉积,从而促进动脉粥样硬化斑块形成。除主动吸烟外,尚有部分人群长期暴露于烟雾场合,成为被动吸烟者,此类人群的颈部动脉粥样硬化情况有待研究。多层螺旋CT的发展使得颈部动脉CT血管成像(CT angiography,CTA)成为可能,且随着成像技术的不断提高,其对于斑块的显示及血管狭窄程度的测量相较于数字减影血管造影(DSA)、超声具有独特的优势[2-3]。本研究旨在通过对比吸烟、被动吸烟、非吸烟者的多层螺旋颈部CTA图像上颈部动脉粥样硬化斑块的特征,无创性评价吸烟和被动吸烟对颈部动脉粥样硬化斑块的影响。
-
回顾性分析2017年1月至2019年7月于山东省聊城市茌平区人民医院行颈部CTA的拟诊为脑血管病的受检者284名,其中,男性133名、女性151名,年龄42~79(60.3±12.5)岁。根据是否吸烟或被动吸烟将受检者分为吸烟组(95名)、被动吸烟组(87名)、非吸烟组(102名)。纳入标准:CTA图像质量清晰、一般资料完整者。排除标准:吸烟史不明确者、脑动脉支架术后者、严重心肾功能不全者、碘过敏者。吸烟诊断标准:每天吸烟支数≥1支,并持续1年以上。被动吸烟诊断标准:自身不吸烟,但平均每天暴露于吸烟环境1 h以上,并持续1年以上。非吸烟诊断标准:自身不吸烟,且无持续暴露于吸烟环境者。所有受检者均于检查前签署了知情同意书。本研究符合《赫尔辛基宣言》的原则。
-
设计调查问卷,每名受检者检查前进行认真记录,内容包括受检者的主动吸烟或被动吸烟情况(吸烟者平均每天吸烟量及吸烟年限、被动吸烟者每天暴露于吸烟环境中的平均时长及年限)、身高、体重、血压、是否患有糖尿病和(或)高血脂。吸烟者的吸烟指数=平均每天吸烟支数×吸烟年数;被动吸烟者的吸烟指数=平均每天暴露于吸烟环境中的小时数×被动吸烟年数。
-
使用荷兰Philips公司Brilliance 64排螺旋CT进行扫描。受检者仰卧位,肩部尽量下垂。采用双筒高压注射器将显像剂碘帕醇75~80 mL(上海博莱科信谊药业有限责任公司,370 mgI /mL)以4.0~5.0 mL/s的流速经肘静脉注入,随后以同一流速注入30 mL生理盐水。扫描条件:管电压120 kV、管电流360 mA、机架旋转时间400 ms、螺距0.2、探测器准直64×0.8 mm、扫描时间8~10 s。扫描时嘱受检者勿做吞咽动作,ROI置于主动脉弓处,触发阈值150 HU。扫描范围自主动脉弓水平至颅底动脉环水平。采用最大密度投影(MIP)、曲面重建(CPR)、容积重建(VR)、多平面重组(MPR)进行图像后处理。使用荷兰Philips公司Extended BrillianceTM Workspace(版本4.5.3.40140)工作站测量斑块。
-
(1)颈部动脉分段。依据北美症状性颈部动脉内膜切除试验(NASCET)指南[4]将颈部动脉分为10段:左右颈总动脉、左右颈总动脉分叉处、左右颈内动脉颅外段、左右颈外动脉、左右椎动脉颅外段。其中,左右颈总动脉分叉处定义为自分叉“V”型隆嵴处沿血管长轴向近侧和远侧各延伸3 cm的范围,包括颈总动脉末端及颈内动脉起始段、颈外动脉起始段。
(2)斑块分型。将所有斑块分为非钙化斑块、钙化斑块、混合型斑块3种类型。其中,非钙化斑块为斑块无钙化,其密度低于增强的血管腔密度;钙化斑块为钙化区域(CT值>130 HU)大于斑块面积的50%;混合型斑块为钙化区域小于斑块面积的50%。对所有斑块的以下几项指标进行测量:①最大横截面积;②重构指数,即管腔最窄处血管面积与血管平均面积(斑块近侧和远侧血管横截面积的平均值)的比值;③斑块负荷,即选取斑块面积最大的血管横截面,测量斑块面积与同层面血管总面积的比值。
由2名有5年以上工作经验的主治医师或以上职称的放射科医师在不了解受检者吸烟情况及所有临床资料的情况下,独立评估颈部动脉斑块累及节段数、斑块类型及累及节段,并进行定量指标的测量,结果不一致时协商达成一致,所有定量指标取平均值。
-
采用SPSS17.0软件进行统计学分析。定性资料采用率表示,组间比较采用χ2检验;定量资料符合正态分布,以
$\bar x $ ±s表示,多组间比较采用单因素方差分析,两组间比较采用独立样本t检验(方差齐)。吸烟指数与斑块累及节段数的相关性分析采用Spearman秩相关检验。P<0.05为差异有统计学意义。 -
由表1可知,吸烟组男性比例(83.2%,79/95)高于被动吸烟组(31.0%,27/87)和非吸烟组(26.5%,27/102),差异均有统计学意义(χ2= 10.03、9.77,均P<0.05)。被动吸烟组和非吸烟组的性别组成差异无统计学意义。3组受检者的年龄,体重指数,高血压、糖尿病及高血脂的发病率的差异均无统计学意义(F=0.30、0.43;χ2=1.58、0.19、0.56,均P>0.05)。
组别 年龄(岁) 性别[例(%)] 体重指数(kg/m2) 疾病发生率[例(%)] 女 男 糖尿病 高血压 高血脂 吸烟组(n=95) 59.3±10.1 16(16.8) 79(83.2) 22.3±9.2 20(21.1) 40(42.1) 35(36.8) 被动吸烟组(n=87) 60.2±12.0 60(69.0) 27(31.0)a 22.5±8.9 19(21.8) 38(43.7) 33(37.9) 非吸烟组(n=102) 61.5±9.5 75(73.5) 27(26.5)a 21.5±9.5 22(21.6) 45(44.1) 37(36.3) 检验值 F=0.30 χ2=10.65 F=0.43 χ2=0.19 χ2=1.58 χ2=0.56 P值 0.82 0.01 0.74 0.66 0.80 0.43 注:表中,a:与吸烟组比较,差异均有统计学意义(χ2=10.03、9.77,均P<0.05) 表 1 3组受检者临床资料的比较
Table 1. General conditions of the smoking, passive smoking and nonsmoking groups
-
3组受检者共检测2840个动脉节段,其中2058(72.5%)个节段存在斑块。钙化斑块、混合型斑块、非钙化斑块的典型CTA图像分别见图1~3。由表2可知,吸烟组和被动吸烟组的总斑块、非钙化斑块、混合型斑块累及节段比例均高于非吸烟组,差异均有统计学意义(χ2=7.43~21.33,均P<0.05)。吸烟组总斑块、非钙化斑块累及节段比例高于被动吸烟组,差异均有统计学意义(χ2=7.40、9.77,均P<0.05)。3组受检者钙化斑块累及节段比例的差异无统计学意义(χ2=0.82,P>0.05)。
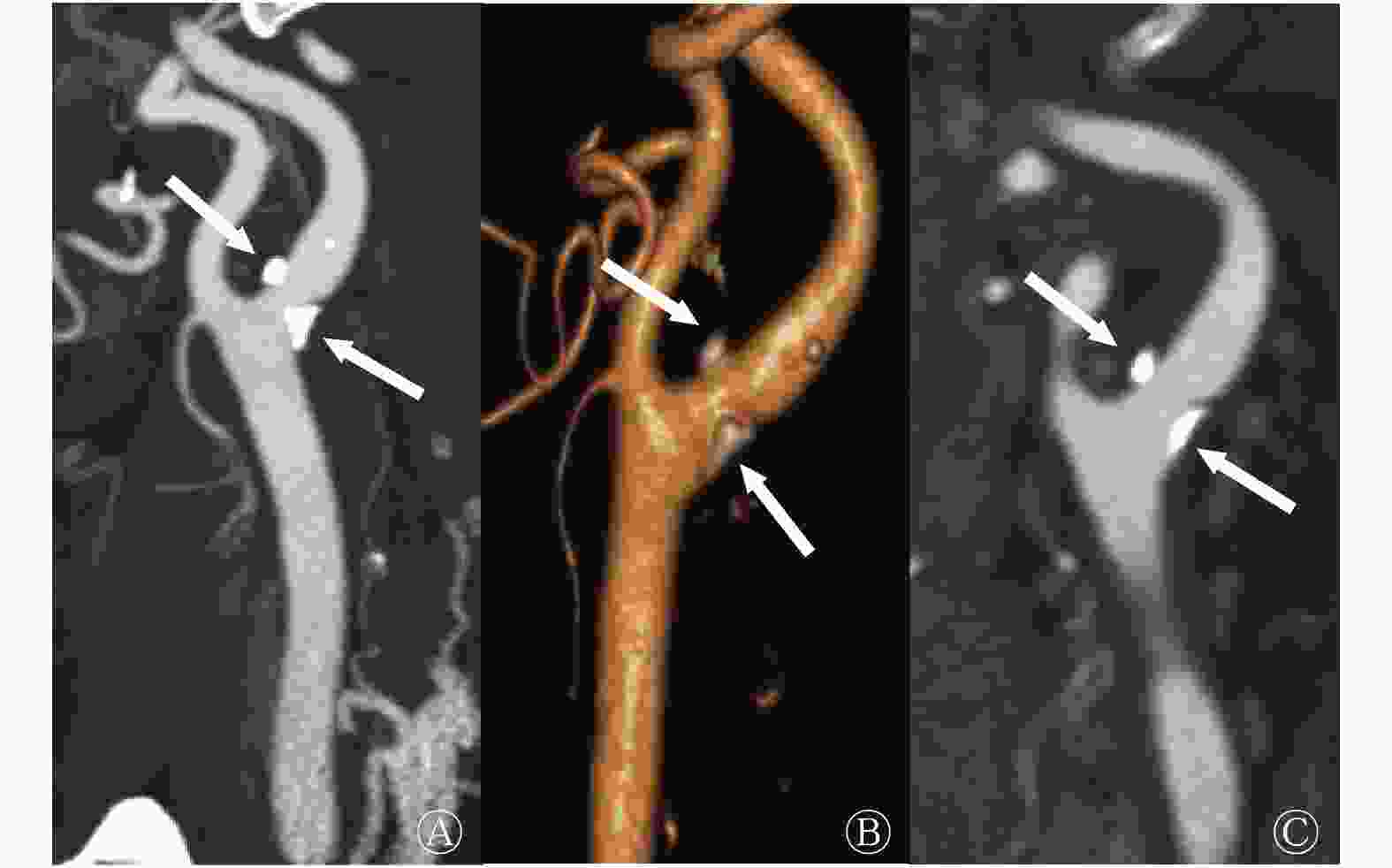
图 1 吸烟者(男性,65岁)左侧颈总动脉分叉处钙化斑块CT血管成像图 图中,最大密度投影(A)、容积重建(B)、多平面重组(C)图像均显示左侧颈总动脉分叉处多发钙化斑块(箭头所示)。CT:计算机体层摄影术
Figure 1. CT angiography images showing calcified plaques at the left common carotid bifurcation of a 65-year-old male smoker
组别 动脉节段数 累及节段数 总斑块 钙化斑块 非钙化斑块 混合型斑块 吸烟组(n=95) 950 765(80.5)a,b 534(56.2) 445(46.8)a,b 433(45.6)b 被动吸烟组(n=87) 870 650(74.7)b 480(55.2) 348(40.0)b 360(41.4)b 非吸烟组(n=102) 1020 643(63.0) 568(55.7) 213(20.9) 314(30.8) χ2值 8.56 0.82 9.40 10.61 P值 0.04 0.78 0.03 0.02 注:表中,a:与被动吸烟组比较,差异均有统计学意义(χ2=7.40、9.77,均P<0.05);b:与非吸烟组比较,差异均有统计学意义(χ2=7.43~21.33,均P<0.05) 表 2 3组受检者斑块分型和累及节段数的比较[个(%)]
Table 2. Plaque types and numbers of involved segments in the smoking, passive smoking and nonsmoking groups (%)
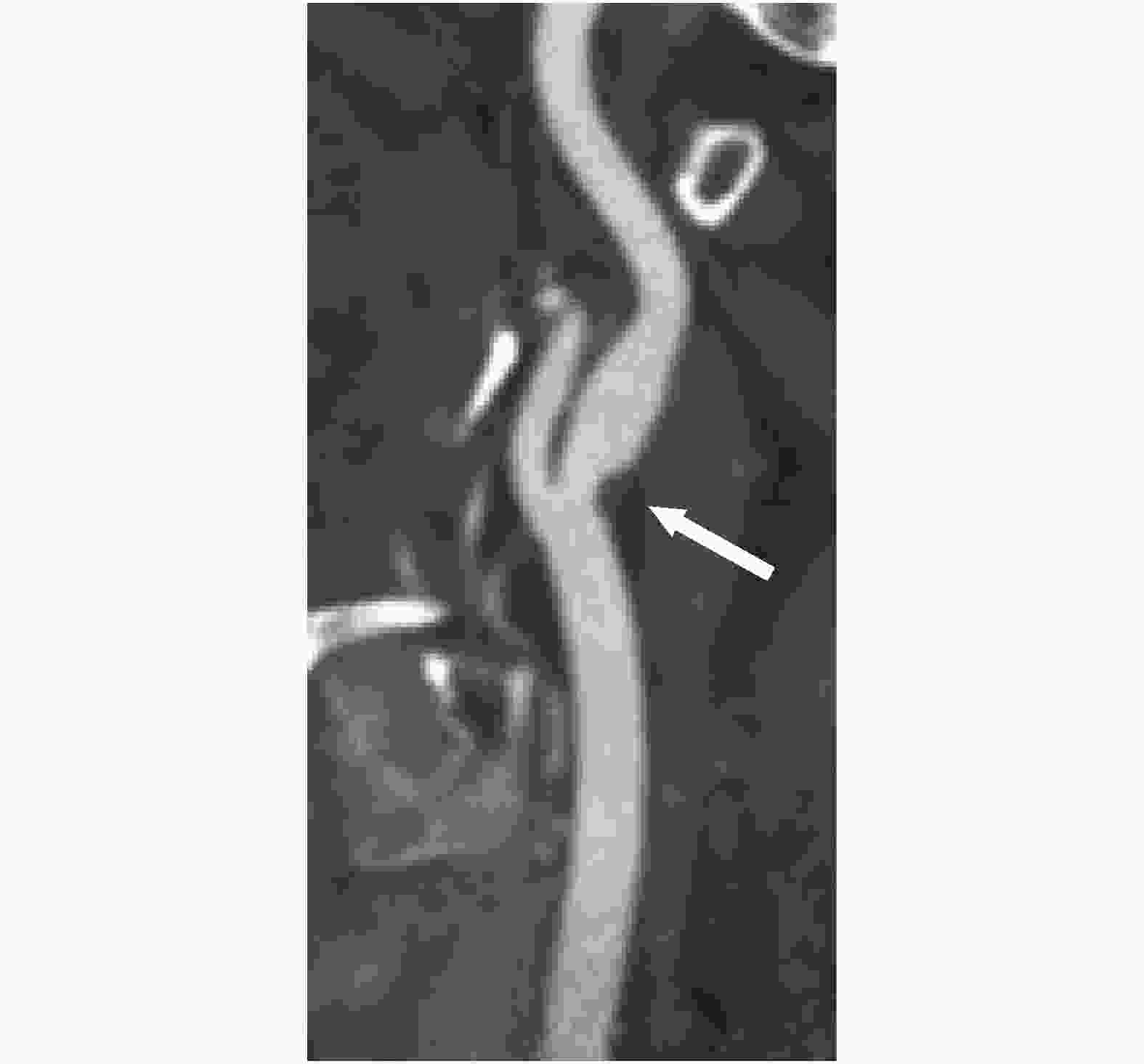
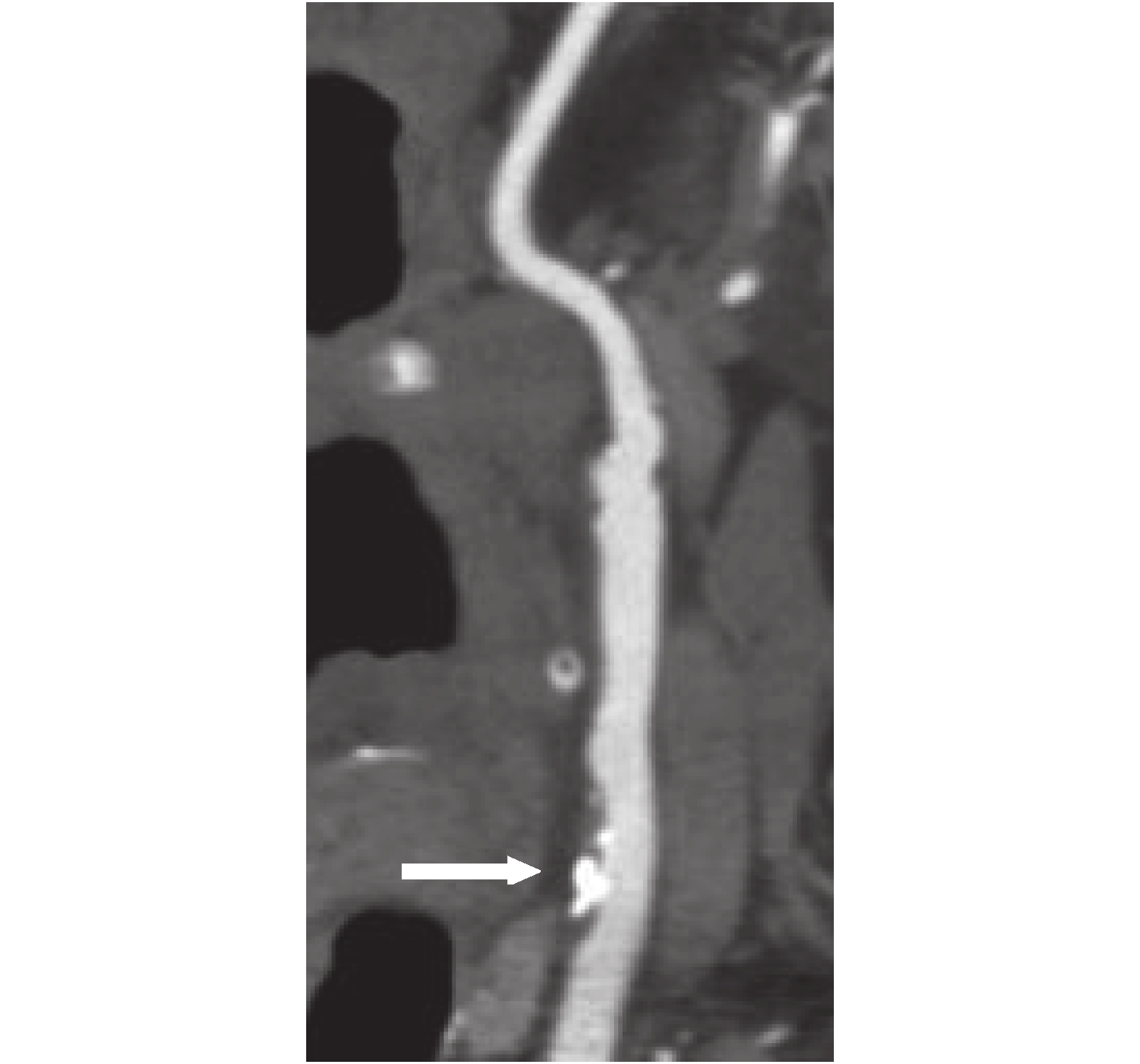
图 3 吸烟者(男性,59岁)颈总动脉分叉处非钙化斑块CT血管成像图 图中,曲面重建图像显示颈总动脉分叉处非钙化斑块(箭头所示)。CT:计算机体层摄影术
Figure 3. CT angiography image showing noncalcified plaque at the common carotid bifurcation of a 59-year-old male smoker
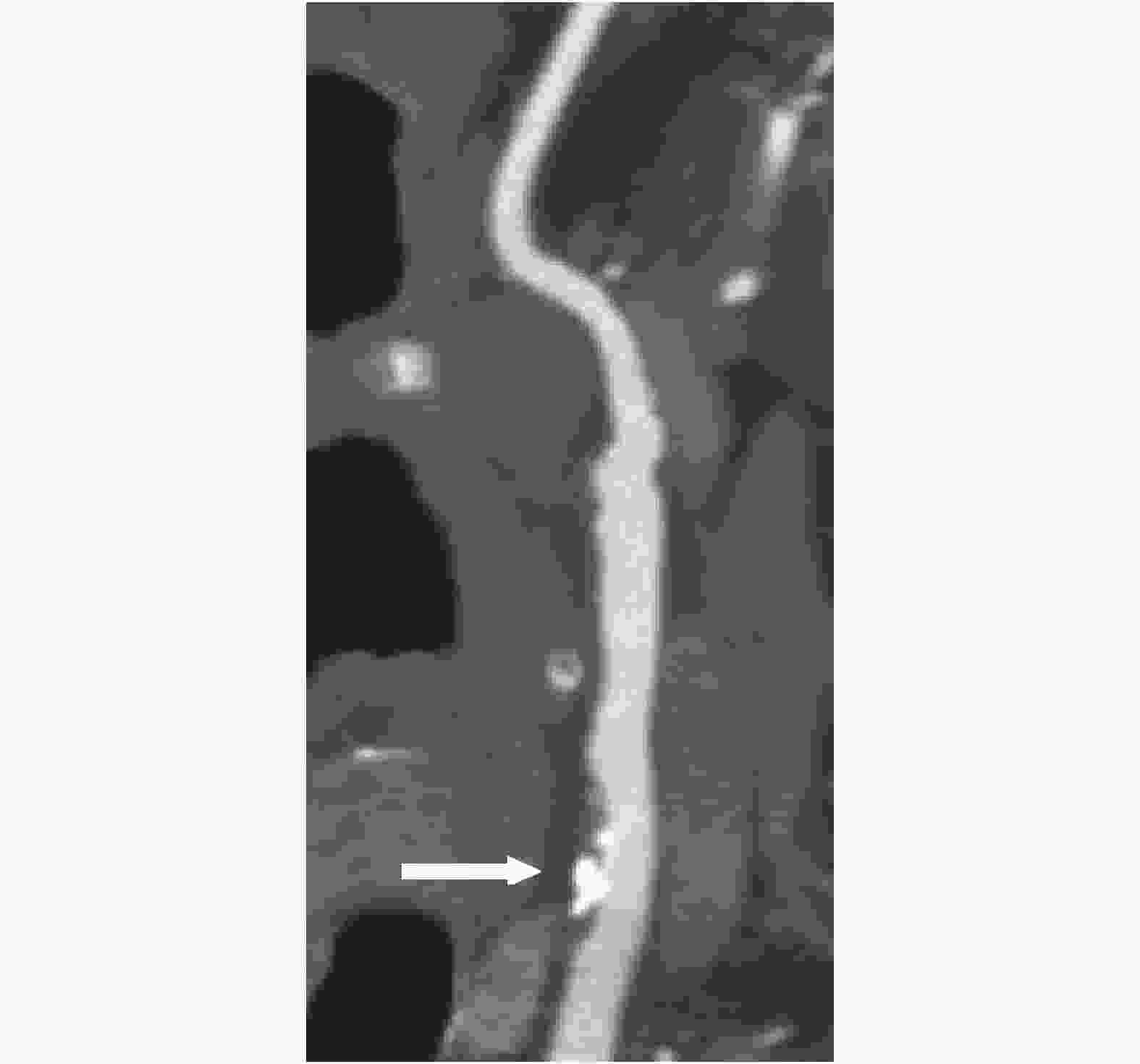
图 2 被动吸烟者(女性,68岁)颈总动脉混合型斑块CT血管成像图 图中,曲面重建图像显示颈总动脉混合型斑块(箭头所示)。CT:计算机体层摄影术
Figure 2. CT angiography image showing mixed plaque at the common carotid artery of a 68-year-old female passive smoker
-
3组受检者斑块测量指标的比较结果见表3。吸烟组和被动吸烟组所有类型斑块的最大横截面积、斑块负荷、重构指数均明显高于非吸烟组,差异均有统计学意义(t=6.54~20.11,均P<0.05)。吸烟组混合型斑块和非钙化斑块的最大横截面积、斑块负荷、重构指数均明显高于被动吸烟组,差异均有统计学意义(t=9.05~15.64,均P<0.05)。
组别 动脉
节段数斑块最大横截面积(mm2) 斑块负荷(%) 重构指数 钙化斑块 混合型斑块 非钙化斑块 钙化斑块 混合型斑块 非钙化斑块 钙化斑块 混合型斑块 非钙化斑块 吸烟组(n=95) 950 12.45±4.22a 12.30±4.34a,b 12.25±4.34a,b 40.34±12.02a 42.56±12.02a,b 41.22±12.02a,b 1.09±0.17a 1.12±0.02a,b 1.11±0.06a,b 被动吸烟组(n=87) 870 11.82±2.35a 10.00±2.55a 9.34±2.55a 40.87±9.88a 36.33±9.43a 37.65±8.20a 1.08±0.11a 1.09±0.10a 1.07±0.05a 非吸烟组(n=102) 1020 8.23±2.20 8.32±2.13 8.50±2.55 32.78±7.69 29.67±7.65 30.05±6.67 0.94±0.02 0.88±0.01 0.90±0.01 F值 10.73 9.54 11.00 12.80 8.59 9.03 13.50 18.99 14.55 P值 0.05 0.05 0.04 0.04 0.05 0.04 0.03 0.01 0.02 注:表中,a:与非吸烟组比较,差异均有统计学意义(t=6.54~20.11,均P<0.05);b:与被动吸烟组比较,差异均有统计学意义(t=9.05~15.64,均P<0.05) 表 3 3组受检者斑块测量指标的比较(
$\bar x $ Table 3. Quantitative measurements of plaques in the smoking, passive smoking and nonsmoking groups (
$\bar x $ -
吸烟组和被动吸烟组的吸烟指数与总斑块、非钙化斑块、混合型斑块的累及节段数均呈正相关(吸烟组:r=0.52、0.57、0.48,均P<0.05;被动吸烟组:r=0.40、0.42、0.43,均P<0.05),2组吸烟指数与钙化斑块的累及节段数无相关性(r=0.03~0.08,均P>0.05)。
-
吸烟与颈部动脉粥样硬化的关系已被多项研究结果证实[5]。郑越昌等[6]研究发现,吸烟是佳木斯地区脑卒中高危人群颈部动脉斑块形成的重要危险因素;洪玉娥等[7]认为颈部动脉斑块的形成与吸烟等因素有关;李涛等[1]认为,在脑卒中高危人群中,吸烟是颈部动脉硬化及斑块形成的独立危险因素,吸烟时间、吸烟量等与颈部动脉粥样硬化的发生呈正相关。但既往的研究多采用超声作为颈部动脉斑块的测量方法,超声检查简便易行,且对于颈部动脉斑块检测的灵敏度高,可检出直径为1 mm以内的斑块[8],对于浅表的颈总动脉显示清楚,但对于颈内动脉远端的显示欠佳,且受操作者水平影响较大。近年来CTA技术发展迅速,因其具有无创、分辨率高、扫描范围大、可多角度多平面观察等独特的优势,已逐渐成为颈部动脉成像的主要方法。本研究采用CTA作为评估方法,探讨吸烟对颈部动脉斑块发生率、类型、分布及量化指标的影响。另外,除主动吸烟外,被动吸烟也成为危害健康的不可忽视的因素,近年来受到越来越多地关注,多项结果研究表明,被动吸烟能导致颈部动脉内中膜厚度增加,血管弹性下降[9-10],但关于被动吸烟与颈部动脉斑块形态及分布的关系的CTA研究未见报道。本研究将吸烟和被动吸烟者同时纳入研究组,以探讨吸烟和被动吸烟对颈部动脉斑块的影响。
有研究结果表明,非钙化斑块、混合型斑块更倾向于不稳定性斑块(易损斑块),而钙化斑块相对稳定,可能与非钙化斑块、混合型斑块含有较大的脂质核心有关[11]。本研究结果显示,吸烟组、被动吸烟组患者总斑块、非钙化斑块、混合型斑块累及节段比例均高于非吸烟组,而3组的钙化斑块累及节段比例差异无统计学意义;吸烟组总斑块、非钙化斑块累及节段比例高于被动吸烟组。提示吸烟和被动吸烟均易导致易损斑块的形成,增加脑卒中风险。这与陈蓓蕾等[12]通过高分辨率MRI研究的结果一致,其研究结果同样显示吸烟是颈部动脉不稳定斑块的独立危险因素。另外,本研究结果显示,吸烟组、被动吸烟组所有斑块的最大横截面积、斑块负荷均明显大于非吸烟组,而吸烟组非钙化斑块、混合型斑块的最大横截面积、斑块负荷均大于被动吸烟组,提示斑块负荷更大,管腔狭窄更明显,更易导致脑供血不足。这与既往研究结果一致:Herder等[13]通过超声研究发现,吸烟是导致颈部动脉内中膜增厚和总斑块面积增加的独立危险因素;Vukadinovic等[14]发现,吸烟导致颈部动脉总斑块体积增加。另外,重构指数也是斑块易损性的重要指标,重构指数越大提示斑块越不稳定。本研究结果显示吸烟组、被动吸烟组斑块的重构指数均大于非吸烟组,吸烟组混合型斑块、非钙化斑块的重构指数均大于被动吸烟组。本研究结果还显示,吸烟组、被动吸烟组的吸烟指数与总斑块、混合型斑块、非钙化斑块累及节段数均呈正相关,提示吸烟量越大,颈部动脉粥样硬化越严重;李亚玉等[15]同样发现,吸烟指数与颈部动脉斑块分级、颈部动脉狭窄程度呈正相关。
本研究尚有以下不足之处:①受检者人数较少;②高血压、糖尿病和高血脂等因素可能对颈部动脉斑块有一定的影响,本研究未进行细化分析;③吸烟组、被动吸烟组未按照吸烟量进行细化分组,可能存在组内差异;④只分析了吸烟量、吸烟年限与斑块累及节段数的相关性,而吸烟量、吸烟年限与颈部动脉斑块的量化指标是否存在相关性,以及戒烟对于颈部动脉斑块有何影响等尚有待进一步地研究。
综上所述,吸烟、被动吸烟均可以导致颈部动脉斑块累及节段数增多,混合型斑块和非钙化斑块累及节段比例增加,斑块量化指标(斑块最大横截面积、斑块负荷、重构指数)增大,从而加重脑血管病的发生风险,且吸烟和被动吸烟量越大、年限越长颈部动脉斑块累及节段数越多。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 王飞飞负责试验的设计、论文的撰写;迟华群负责临床资料的记录及分析;刘月平、路彬负责数据的测量与分析、统计学的分析;郝大鹏负责论文的审阅及校对。
CTA评估吸烟和被动吸烟对颈部动脉粥样硬化斑块的影响
Effects of smoking and passive exposure to cigarette smoke on atherosclerotic plaques in extracranial arteries assessed by computed tomography angiography
-
摘要:
目的 通过CT血管成像(CTA)评估吸烟和被动吸烟对颈部动脉粥样硬化斑块的影响。 方法 回顾性分析2017年1月至2019年7月于山东省聊城市茌平区人民医院行颈部CTA的拟诊为脑血管病的受检者284名,其中男性133名、女性151名,年龄42~79(60.3±12.5)岁。根据是否吸烟或被动吸烟将受检者分为吸烟组(95名)、被动吸烟组(87名)、非吸烟组(102名)。比较3组受检者的颈部动脉粥样硬化斑块的累及节段数、类型、最大横截面积、斑块负荷、重构指数,并分析吸烟指数与斑块累及节段数之间的相关性。定性资料的组间比较采用χ2检验;定量资料的多组间比较采用单因素方差分析,2组间比较采用独立样本t检验;吸烟指数与斑块累及节段数的相关性分析采用Spearman秩相关检验。 结果 3组受检者的年龄,体重指数,高血压、糖尿病及高血脂的发病率的差异均无统计学意义(F=0.30、0.43;χ2=1.58、0.19、0.56,均P>0.05)。吸烟组男性比例(83.2%,79/95)高于被动吸烟组(31.0%,27/87)和非吸烟组(26.5%,27/102),差异均有统计学意义(χ2=10.03、9.77,均P<0.05)。284名受检者共检测2840个动脉节段,其中2058个(72.5%)节段存在斑块。吸烟组和被动吸烟组的总斑块[80.5%(765/950)、74.7%(650/870)]、非钙化斑块[46.8%(445/950)、40.0%(348/870)]、混合型斑块[45.6%(433/950)、41.4%(360/870)]累及节段比例均高于非吸烟组[63.0%(643/1020)、20.9%(213/1020)、30.8%(314/1020)],且差异均有统计学意义(χ2=7.43~21.33,均P<0.05);吸烟组总斑块、非钙化斑块累及节段比例高于被动吸烟组,且差异均有统计学意义(χ2=7.40、9.77,均P<0.05)。吸烟组、被动吸烟组所有类型斑块的最大横截面积、斑块负荷、重构指数均明显高于非吸烟组,且差异均有统计学意义(t=6.54~20.11,均P<0.05)。吸烟组混合型斑块及非钙化斑块的最大横截面积、斑块负荷、重构指数均明显高于被动吸烟组,且差异均有统计学意义(t=9.05~15.64,均P<0.05)。吸烟组和被动吸烟组的吸烟指数与总斑块、非钙化斑块、混合型斑块的累及节段数均呈正相关(吸烟组:r=0.52、0.57、0.48,均P<0.05;被动吸烟组:r=0.40、0.42、0.43,均P<0.05)。 结论 吸烟、被动吸烟均可导致颈部动脉粥样硬化斑块数量增多、斑块量化指标增大;且吸烟量越大、年限越长颈部动脉斑块的累及节段数越多。 -
关键词:
- 颈动脉疾病 /
- 计算机体层摄影血管造影术 /
- 吸烟 /
- 斑块,动脉粥样硬化
Abstract:Objective To explore differences in the morphology of atherosclerotic plaques among active smokers, passive smokers, and nonsmokers using CT angiography (CTA). Methods A retrospective analysis was performed on 284 patients (133 males and 151 females aged 42−79 (60.3±12.5) years old) with suspected cerebrovascular disease, including 95 active smokers and 87 passive smokers, and 102 nonsmokers who underwent 64-slice extracranial CTA in Chiping People's Hospital in Liaocheng City of Shandong Province from January 2017 to July 2019. Numbers of plaque involved segments, plaque type, area, burden, and remodeling index were compared among the three groups. Correlations between smoking index and numbers of plaque involved segments in the smoking and passive smoking groups were also calculated. Rates and the χ2 test were used to analyze qualitative data, while t test and one-way ANOVA were used to assess quantitative data. Spearman’s rank correlation test was used to analyze the relationship between smoking index and numbers of plaque involved segments. Results No difference in age, body mass index, incidence rates of diabetes, hypertension, hyperlipidemia was observed between groups (F=0.30, 0.43; χ2=1.58, 0.19, 0.56, all P>0.05). More males belonged to the active smoking group (83.2%, 79/95) than to the passive smoking (31.0%, 27/87) and nonsmoking (26.5%, 27/102) groups (χ2=10.03, 9.77, both P<0.05). A total of 2840 segments from 284 patients were studied, and 2058 (72.5%) segments revealed plaques. Total plaques (80.5% (765/950), 74.7% (650/870)), noncalcified plaques (46.8% (445/950), 40.0% (348/870)), and mixed plaques (45.6% (433/950), 41.4% (360/870)) involved segments percentages were more higher in the smoking and passive smoking groups than in the nonsmoking group (total plaques, 63.0% (643/1020); noncalcified plaques, 20.9% (213/1020); mixed plaques, 30.8% (314/1020)) (χ2=7.43−21.33, all P<0.05). Total plaques, noncalcified plaques involved segments percentages in the smoking group were more higher than in the passive smoking groups(χ2=7.40, 9.77, both P<0.05). Smokers and passive smokers had a higher plaque area, plaque burden, and remodeling index than nonsmokers in three types of plaques(t=6.54−20.11, all P<0.05), while smokers had a higher plaque area, plaque burden, and remodeling index than passive smokers in noncalcified and mixed plaques (t=9.05−15.64, all P<0.05). A positive correlation between smoking index and total plaques, noncalcified plaques, mixed plaques involved segments numbers in the smoking and passive smoking groups (smoking: r=0.52, 0.57, 0.48, all P<0.05; passive smoking: r=0.40, 0.42, 0.43, all P<0.05) were observed. Conclusions Active and passive exposure to smoke can lead to more atherosclerotic plaques and higher quantitative index. The greater the amount of smoking and the longer the age, the more segments involved in carotid artery plaque will be found. -
图 1 吸烟者(男性,65岁)左侧颈总动脉分叉处钙化斑块CT血管成像图 图中,最大密度投影(A)、容积重建(B)、多平面重组(C)图像均显示左侧颈总动脉分叉处多发钙化斑块(箭头所示)。CT:计算机体层摄影术
Figure 1. CT angiography images showing calcified plaques at the left common carotid bifurcation of a 65-year-old male smoker
图 3 吸烟者(男性,59岁)颈总动脉分叉处非钙化斑块CT血管成像图 图中,曲面重建图像显示颈总动脉分叉处非钙化斑块(箭头所示)。CT:计算机体层摄影术
Figure 3. CT angiography image showing noncalcified plaque at the common carotid bifurcation of a 59-year-old male smoker
图 2 被动吸烟者(女性,68岁)颈总动脉混合型斑块CT血管成像图 图中,曲面重建图像显示颈总动脉混合型斑块(箭头所示)。CT:计算机体层摄影术
Figure 2. CT angiography image showing mixed plaque at the common carotid artery of a 68-year-old female passive smoker
表 1 3组受检者临床资料的比较
Table 1. General conditions of the smoking, passive smoking and nonsmoking groups
组别 年龄(岁) 性别[例(%)] 体重指数(kg/m2) 疾病发生率[例(%)] 女 男 糖尿病 高血压 高血脂 吸烟组(n=95) 59.3±10.1 16(16.8) 79(83.2) 22.3±9.2 20(21.1) 40(42.1) 35(36.8) 被动吸烟组(n=87) 60.2±12.0 60(69.0) 27(31.0)a 22.5±8.9 19(21.8) 38(43.7) 33(37.9) 非吸烟组(n=102) 61.5±9.5 75(73.5) 27(26.5)a 21.5±9.5 22(21.6) 45(44.1) 37(36.3) 检验值 F=0.30 χ2=10.65 F=0.43 χ2=0.19 χ2=1.58 χ2=0.56 P值 0.82 0.01 0.74 0.66 0.80 0.43 注:表中,a:与吸烟组比较,差异均有统计学意义(χ2=10.03、9.77,均P<0.05)  下载: 导出CSV
下载: 导出CSV
表 2 3组受检者斑块分型和累及节段数的比较[个(%)]
Table 2. Plaque types and numbers of involved segments in the smoking, passive smoking and nonsmoking groups (%)
组别 动脉节段数 累及节段数 总斑块 钙化斑块 非钙化斑块 混合型斑块 吸烟组(n=95) 950 765(80.5)a,b 534(56.2) 445(46.8)a,b 433(45.6)b 被动吸烟组(n=87) 870 650(74.7)b 480(55.2) 348(40.0)b 360(41.4)b 非吸烟组(n=102) 1020 643(63.0) 568(55.7) 213(20.9) 314(30.8) χ2值 8.56 0.82 9.40 10.61 P值 0.04 0.78 0.03 0.02 注:表中,a:与被动吸烟组比较,差异均有统计学意义(χ2=7.40、9.77,均P<0.05);b:与非吸烟组比较,差异均有统计学意义(χ2=7.43~21.33,均P<0.05)
下载: 导出CSV
表 3 3组受检者斑块测量指标的比较(
$\bar x $ Table 3. Quantitative measurements of plaques in the smoking, passive smoking and nonsmoking groups (
$\bar x $ 组别 动脉
节段数斑块最大横截面积(mm2) 斑块负荷(%) 重构指数 钙化斑块 混合型斑块 非钙化斑块 钙化斑块 混合型斑块 非钙化斑块 钙化斑块 混合型斑块 非钙化斑块 吸烟组(n=95) 950 12.45±4.22a 12.30±4.34a,b 12.25±4.34a,b 40.34±12.02a 42.56±12.02a,b 41.22±12.02a,b 1.09±0.17a 1.12±0.02a,b 1.11±0.06a,b 被动吸烟组(n=87) 870 11.82±2.35a 10.00±2.55a 9.34±2.55a 40.87±9.88a 36.33±9.43a 37.65±8.20a 1.08±0.11a 1.09±0.10a 1.07±0.05a 非吸烟组(n=102) 1020 8.23±2.20 8.32±2.13 8.50±2.55 32.78±7.69 29.67±7.65 30.05±6.67 0.94±0.02 0.88±0.01 0.90±0.01 F值 10.73 9.54 11.00 12.80 8.59 9.03 13.50 18.99 14.55 P值 0.05 0.05 0.04 0.04 0.05 0.04 0.03 0.01 0.02 注:表中,a:与非吸烟组比较,差异均有统计学意义(t=6.54~20.11,均P<0.05);b:与被动吸烟组比较,差异均有统计学意义(t=9.05~15.64,均P<0.05)
下载: 导出CSV
-
[1] 李涛, 张允岭, 赵晖, 等. 吸烟与脑卒中高危人群颈动脉粥样硬化发生的相关性分析[J]. 中西医结合心脑血管病杂志, 2015, 13(2): 175−178. DOI: 10.3969/j.issn.16721349.2015.02.015.
Li T, Zhang YL, Zhao H, et al. Study on the correlativity between smoking and carotid atherosclerosis for high risk group of stroke[J]. Chin J Integr Med Cardio/Cerebrovascular Dis, 2015, 13(2): 175−178. DOI: 10.3969/j.issn.16721349.2015.02.015.[2] Ramanathan R, Dey D, Nørgaard BL, et al. Carotid plaque composition by CT angiography in asymptomatic subjects: a head-to-head comparison to ultrasound[J]. Eur Radiol, 2019, 29(11): 5920−5931. DOI: 10.1007/s00330-019-06086-y. [3] Song S, Heo R, Lee SE, et al. Comparing the feasibility and accuracy of three-dimensional ultrasound to two-dimensional ultrasound and computed tomography angiography in the assessment of carotid atherosclerosis[J]. Echocardiography, 2019, 36(12): 2241−2250. DOI: 10.1111/echo.14543. [4] North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis[J]. N Engl J Med, 1991, 325(7): 445−453. DOI: 10.1056/NEJM199108153250701. [5] 杨华, 胡斌, 刘月琴, 等. 社区脑卒中高危人群颈动脉粥样硬化危险因素分析[J]. 中国现代医生, 2020, 58(16): 158−161.
Yang H, Hu B, Liu YQ, et al. Analysis on the risk factors of carotid atherosclerosis in high-risk population of stroke in community[J]. China Modern Doctor, 2020, 58(16): 158−161.[6] 郑越昌, 王昆祥, 伊婷婷, 等. 佳木斯地区脑卒中高危人群颈动脉斑块与卒中危险因素的相关性研究[J]. 湖北民族学院学报: 医学版, 2018, 35(1): 18−20. DOI: 10.13501/j.cnki.42-1590/r.2018.01.006.
Zheng YC, Wang KX, Yi TT, et al. Investigation correlation between risk factors and carotid plaques in high risk groups of stroke in Jiamusi Area[J]. J Hubei Univ National: Med Ed, 2018, 35(1): 18−20. DOI: 10.13501/j.cnki.42-1590/r.2018.01.006.[7] 洪玉娥, 吴倩, 贺军. 颈动脉粥样硬化斑块及其危险因素与脑梗死的关系[J]. 临床神经病学杂志, 2009, 22(3): 212−214. DOI: 10.3969/j.issn.1000-7377.2008.12.023.
Hong YE, Wu Q, He J. Relationship between the carotid artery atherosclerotic plaque and its risk factors and cerebral infarction[J]. J Clin Neuro, 2009, 22(3): 212−214. DOI: 10.3969/j.issn.1000-7377.2008.12.023.[8] 李媛媛, 姚晓松, 陈菲, 等. 超声与CTA在评估缺血性脑血管病患者颈动脉粥样斑块性质中的应用[J]. 中国CT和MRI杂志, 2018, 16(4): 47−50. DOI: 10.3969/j.issn.1672-5131.2018.04.015.
Li YY, Yao XS, Chen F, et al. The application of ultrasound and CTA in evaluating carotid atherosclerotic plaques in patients with ischemic cerebrovascular disease[J]. Chin J CT MRI, 2018, 16(4): 47−50. DOI: 10.3969/j.issn.1672-5131.2018.04.015.[9] 赵玉海, 曲胜明, 高燕燕, 等. 被动吸烟对女性颈动脉内中膜厚度影响的对比研究[J]. 中国自然医学杂志, 2009, 11(4): 292−293.
Zhao YH, Qu SM, Gao YY, et al. Comparison study of passive smoking on women's carotid intima-media thickness[J]. Chin J Nat Med, 2009, 11(4): 292−293.[10] 乞艳华, 郑转梅, 周琦, 等. 血管回声跟踪技术评价主动与被动吸烟者动脉弹性功能[J]. 中国医学影像学杂志, 2012, 20(2): 130−133. DOI: 10.3969/j.issn.1005-5185.2012.02.017.
Qi YH, Zheng ZM, Zhou Q, et al. Echo-tracking technology in evaluating carotid artery elasticity function of passive smokers and active smokers[J]. Chin J Med imaging, 2012, 20(2): 130−133. DOI: 10.3969/j.issn.1005-5185.2012.02.017.[11] 王超, 王启荣, 王明涛, 等. 多层螺旋CTA与超声造影联合在颈动脉斑块稳定性评估中的临床应用[J]. 中国CT和MRI杂志, 2018, 16(12): 30−32, 40. DOI: 10.3969/j.issn.1672-5131.2018.12.010.
Wang C, Wang QR, Wang MT, et al. Clinical application of multi-slice spiral CTA combined with contrast-enhanced ultrasound in the stability evaluation of carotid plaque[J]. Chin J CT MRI, 2018, 16(12): 30−32, 40. DOI: 10.3969/j.issn.1672-5131.2018.12.010.[12] 陈蓓蕾, 徐俊, 叶靖, 等. 有症状颈动脉狭窄患者颈动脉斑块的稳定性: 高分辨率磁共振成像研究[J]. 国际脑血管病杂志, 2017, 25(2): 127−133. DOI: 10.3760/cma.j.issn.1673-4165.2017.02.005.
Chen BL, Xu J, Ye J, et al. Carotid plaque stability in patients with symptomatic carotid stenosis: a study of high-resolution magnetic resonance imaging[J]. Int J Cerebrovasc Dis, 2017, 25(2): 127−133. DOI: 10.3760/cma.j.issn.1673-4165.2017.02.005.[13] Herder M, Johnsen SH, Arntzen KA, et al. Risk factors for progression of carotid intima-media thickness and total plaque area: a 13-year follow-up study: the Tromsø Study[J]. Stroke, 2012, 43(7): 1818−1823. DOI: 10.1161/STROKEAHA.111.646596. [14] Vukadinovic D, Rozie S, van Gils M, et al. Automated versus manual segmentation of atherosclerotic carotid plaque volume and components in CTA: associations with cardiovascular risk factors[J]. Int J Cardiovasc Imaging, 2012, 28(4): 877−887. DOI: 10.1007/s10554-011-9890-6. [15] 李亚玉, 王曈, 曲青霞, 等. 吸烟指数与全身动脉粥样硬化的关系研究[J]. 实用心脑肺血管病杂志, 2020, 28(9): 61−66. DOI: 10.3969/j.issn.1008-5971.2020.09.013.
Li YY, Wang T, Qu QX, et al. Relationship between smoking index and systemic atherosclerosis[J]. Pract J Cardiac Cereb Pneum Vasc Dis, 2020, 28(9): 61−66. DOI: 10.3969/j.issn.1008-5971.2020.09.013. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3024
- HTML全文浏览量: 2124
- PDF下载量: 11
