


 下载:
下载:

-
甲状旁腺癌(parathyroid carcinoma,PTC)是一类以甲状旁腺功能亢进为主要临床表现的十分罕见的恶性肿瘤。基于PTC肿瘤细胞的特点,大多数99Tcm-MIBI显像都会表现为阳性。但在某些特殊情况下,有极少部分PTC 99Tcm-MIBI显像表现为阴性,现报道如下。
-
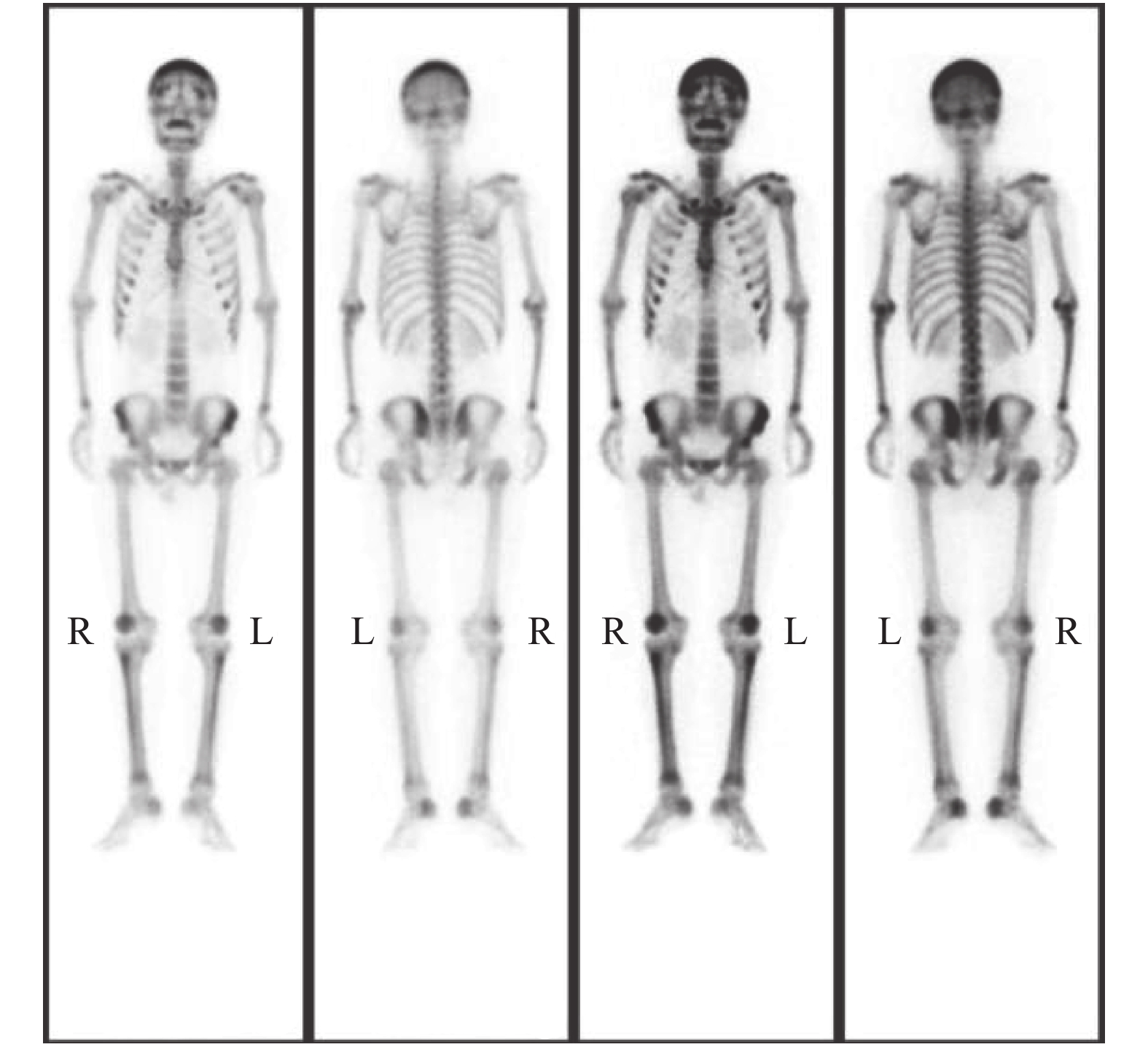
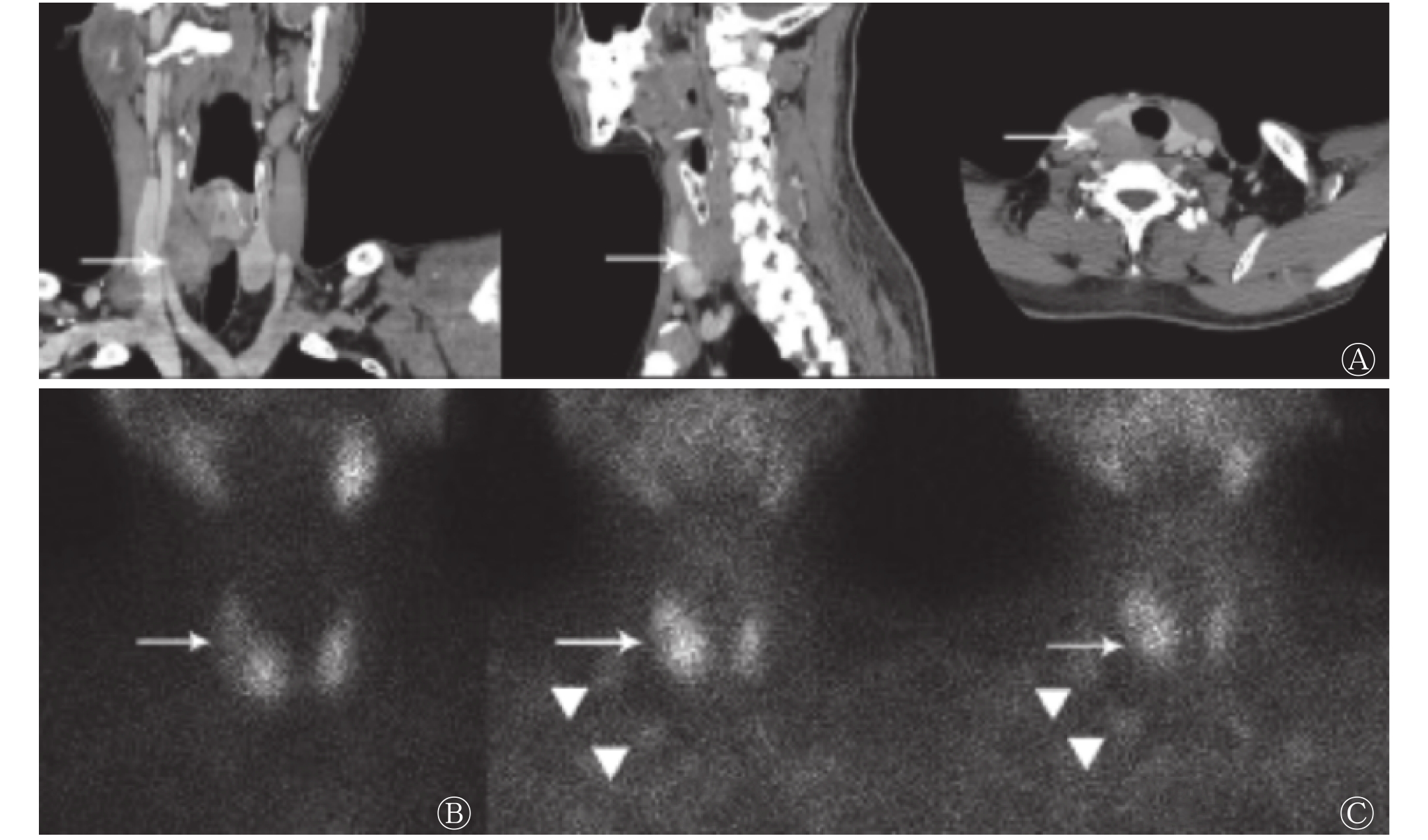
患者男性,41岁,乏力伴多关节疼痛1年。2018年2月于当地医院就诊,血尿酸升高,考虑为“痛风性关节炎”,给予非布司他治疗,上述症状未见明显改善,遂于我院就诊。体格检查结果:双侧甲状腺Ⅱ度肿大,质软,甲状腺右侧叶触及一2.0 cm×2.0 cm的质韧肿物,随吞咽上下活动,无压痛和血管杂音,侧颈部淋巴结触诊不清。辅助检查:心电图示窦性心动过缓(心率55次/min)。甲状旁腺激素(parathyroid hormone,PTH)为1553~1601 pg/mL(正常参考值12~65 pg/mL)、碱性磷酸酶为1392 U/L(正常参考值40~129 U/L)、游离甲状腺激素为7.43 pmol/L(正常参考值11.5~22.7 pmol/L)、总钙为3.49~3.50 mmol/L(正常参考值2.10~2.55 mmol/L)、磷为0.74 mmol/L(正常参考值0.81~1.45 mmol/L)。超声检查结果:甲状腺右侧叶中下部背侧探及大小约3.5 cm×2.4 cm×2.1 cm的低回声肿块;右侧颈部Ⅳ区可见多个淋巴结,较大的2个分别为2.2 cm×1.0 cm和1.8 cm×0.9 cm。增强CT检查结果:甲状腺右叶偏后方可见不规则团块状低强化区(图1中A),右侧颈部Ⅴ区可见增大淋巴结,短径约1.4 cm。X射线检查结果:符合代谢病骨关节的特征。高锝酸盐(99TcmO4−)甲状腺显像结果:甲状腺右叶中部“冷”结节(图1中B)。99Tcm-MIBI双时相平面显像结果:早期相(注射后15 min)见甲状腺右叶中部边界欠清的放射性分布减低区,延迟显像(注射后2 h)未见明显填充;右侧颈部可见2个团状放射性摄取影,延迟显像未见明显降低(图1中C)。全身骨显像结果:超级骨显像,符合甲状旁腺功能亢进引起的代谢性骨病的特征(图2)。
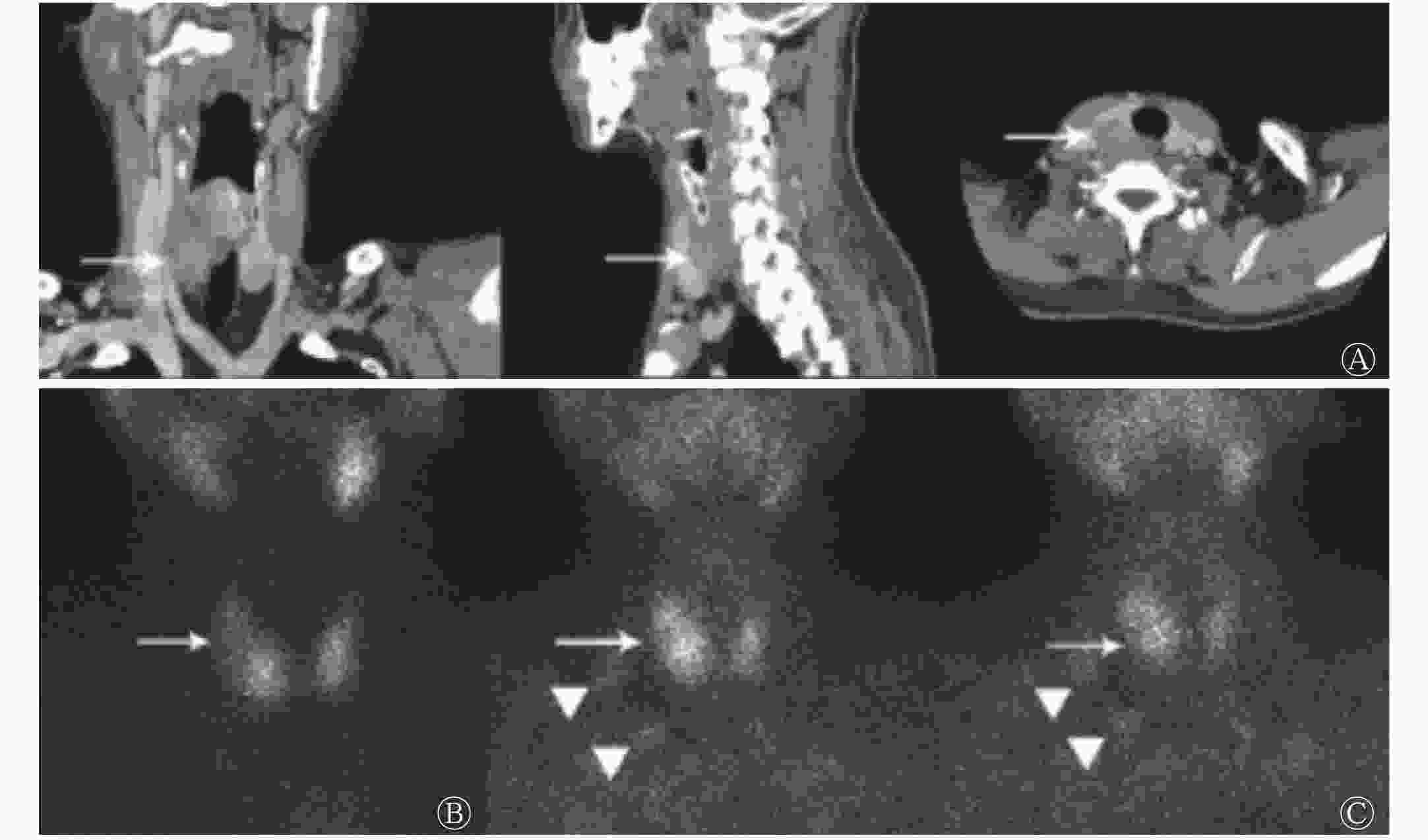
图 1 甲状旁腺癌患者(男性,41岁)影像学检查结果
Figure 1. Imaging findings of a 41 years old man with parathyroid carcinoma

图 2 甲状旁腺癌患者(男性,41岁)全身骨显像图
Figure 2. Whole body bone imaging in a 41 years old man with parathyroid carcinoma
术中所见:甲状腺右叶背侧肿物大小约3.5 cm×2.0 cm×2.0 cm,质硬,边界不清,无明显包膜,与周围组织紧密相连,背侧包绕喉返神经并侵入食道肌层,右侧颈部多发肿大淋巴结,质硬,边界不清,大者短径约为3.0 cm。行(右)甲状腺、PTC切除+喉返神经探查+侧颈部淋巴结清扫术。术中PTC组织离体30 min后复查PTH,为624.1 pg/mL。术后病理结果:甲状腺右叶及右甲状旁腺符合PTC(图3),肿瘤大小为3.2 cm×2.5 cm×2.3 cm,侵及甲状腺,甲状腺右侧颈部Ⅱ、Ⅲ、Ⅳ、Ⅴ区可见转移(5/8),右侧颈部Ⅵ区淋巴结未见转移(0/1)。免疫组化结果:甲状腺转录因子1(−),甲状腺球蛋白(−),嗜铬素A(部分+),CD56(+),Syn(−),Galectin-3(+),Calcitonin(−),细胞角蛋白8/18(+),细胞角蛋白19(+),细胞增殖相关核抗原Ki-67(+,10%)。术后6 d PTH为67.2 pg/mL。
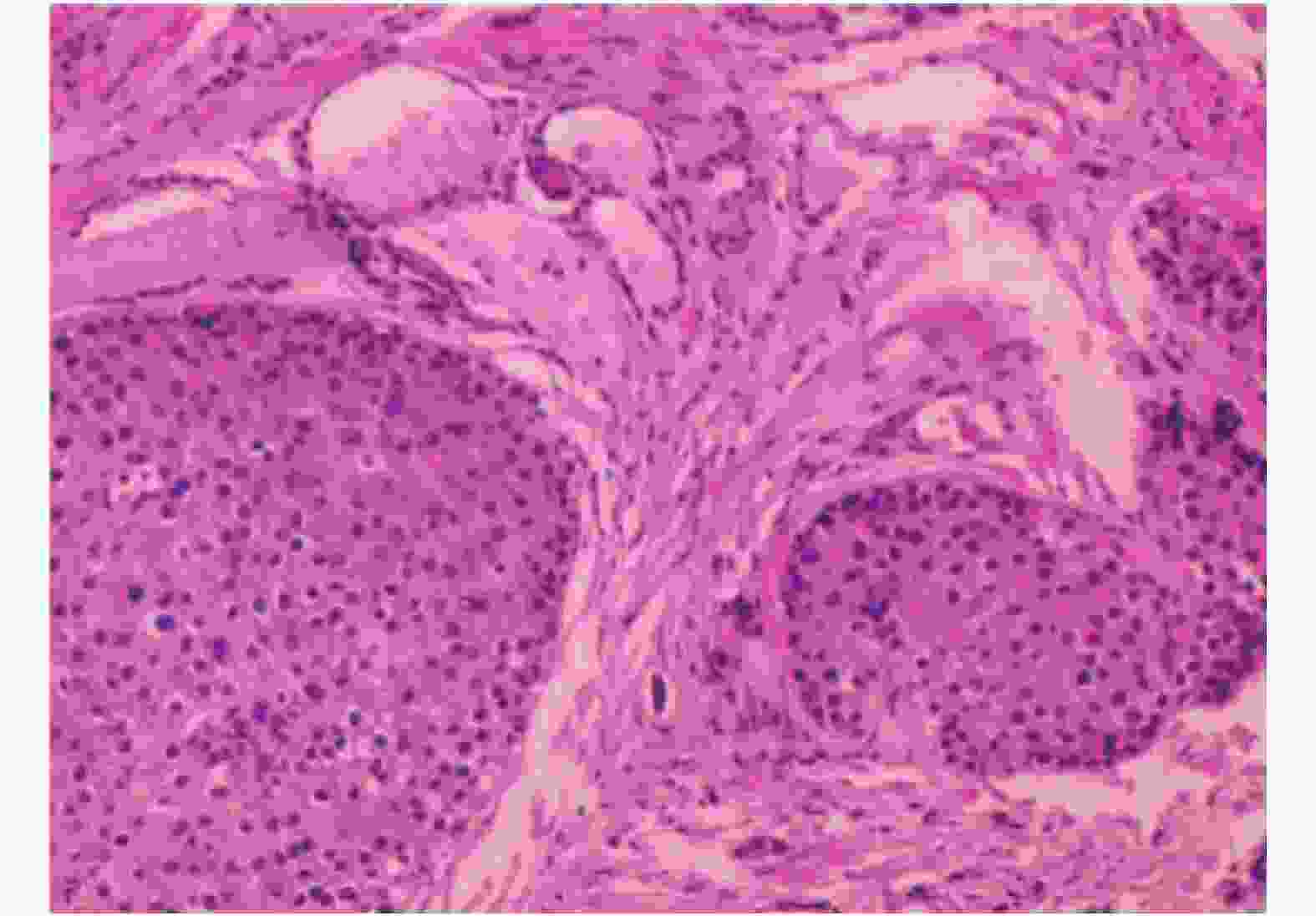
图 3 甲状旁腺癌患者(男性,41岁)病理图
Figure 3. Pathology of a 41 years old man with parathyroid carcinoma
-
PTC发病率占所有恶性肿瘤的 0.005%[1]。自1904年首次报道了1例无功能性PTC以来,英文文献共报道PTC 1000余例[2],国内共报道200余例,大多为个案报道和文献复习。在大多数研究中,PTC只占原发性甲状旁腺功能亢进症的不足1%[3],在日本这一百分比为5.0%[4],在我国该百分比为3.5%[5]。PTC缺乏特异性特征,因此常常造成漏诊、误诊,以致延误治疗。
临床表现:PTC通常散在发生,也可以呈家族聚集性发生。已报道的与PTC有关的遗传综合征包括甲状旁腺功能亢进症-下颌肿瘤综合征(HPT-JT)、多发内分泌腺瘤综合症1型(MEN1)、多发内分泌腺瘤综合症2A型(MEN2A)和家族孤立性原发性甲状旁腺功能亢进症(FIPHPT)[6-7]。PTC的发病年龄在45~60岁之间,比甲状旁腺腺瘤(parathyroid adenoma,PTA)的发病年龄小10岁。PTC男女发病率无明显差别,而PTA更多见于女性(3∶1~4∶1)[7]。我国相关研究结果显示,PTC发病年龄平均为34.8岁,女性多于男性[5]。30%~76%的PTC患者可触及颈前肿物,但仅有不足5%的良性病变患者可触及肿物[8]。
实验室检查:约90%的PTC患者的甲状腺有激素分泌功能,主要表现为PTH水平明显升高(通常是正常值的40倍),血清钙水平通常超过14 mg/dL。而PTA患者的PTH一般不超过正常值上限的3倍[8]。PTC导致的高血钙症状通常比良性甲状旁腺肿瘤导致的高血钙症状更为严重,临床上主要表现为肾脏和骨骼受累,包括乏力、头痛、头晕、呕吐、消化不良、体重减轻、食欲减退、烦渴、多尿、肾绞痛、肾钙化、肾结石、骨痛、骨质疏松和病理性骨折。高血钙还可以导致腹泻、腹痛、消化性溃疡和胰腺炎、心律失常、精神异常如倦怠和抑郁症,甚至发生高钙危象[9-11]。有研究者认为,当血钙超过正常值上限1.15倍以上或血PTH超过正常值上限3倍以上,需高度怀疑PTC,若伴有肾脏病变,则更倾向于恶性诊断[12]。
本研究中该例患者为中青年男性,临床症状典型,主要表现为乏力、多关节疼痛、食欲减退、体重减轻、颈部肿块、窦性心动过缓、高钙低磷血症、高尿磷、PTH及碱性磷酸酶升高,均符合上述研究报道。患者既往体健,无放射线接触史,无明显家族史,属于散发功能型PTC。
病理学分析:PTC肿瘤大小(>3 cm)大于PTA(<3 cm),前者呈分叶状、灰白色、重约2~10 g,质硬,通常粘附于或侵袭周围邻近组织,后者呈椭圆形,红棕色,质软[9]。PTC显微镜下见细胞核异型性,散在分布的滋养核细胞以及增厚的瘤内纤维分割通常提示恶性病变,但PTA中也可见核异型性。PTC镜下亦可见钙化、囊变、凝固性坏死和核分裂像,发现血管或被膜侵犯即可确诊为PTC[10]。本研究中该例患者甲状腺右叶背侧肿物大小约为3.5 cm×2.0 cm×2.0 cm,质硬,边界不清,无明显包膜,与周围组织紧密相连,背侧包绕喉返神经并侵入食道肌层,镜下可见核异型性明显,并且证实存在颈部淋巴结转移,免疫组化结果显示其来源于甲状旁腺组织,故确诊为PTC。
影像学表现:超声、CT和99Tcm-MIBI显像常用于定位甲状旁腺病变,99Tcm-MIBI双时相平面显像诊断PTC的灵敏度为91%[7],因此是较理想的PTC术前定位方法。本研究中该例患者颈部超声及CT均发现甲状腺右叶中下部背侧病变,但99Tcm-MIBI甲状旁腺平面显像阴性。假阴性MIBI显像结果见于5.7%~14%的原发性甲状旁腺功能亢进症患者[13-14],可能与显像分辨率低,病变较小,多发腺体疾病,异位病灶,合并甲状腺疾病,病灶功能差,继发囊变、出血、坏死,注射药物剂量过多,延迟时间过短,组织类型功能较差,以及P-糖蛋白(P-glycoprotein, P-gP)或多药耐药相关蛋白表达有关[15]。MIBI具有P-gP和(或)多药耐药相关蛋白转运底物的特征,可被P-gP识别,并被泵出细胞外,使MIBI无法滞留在细胞内或在细胞内的滞留时间缩短。本研究中该例患者病变占位较大,且CT扫描、术中探查及术后病理均未证实肿瘤存在囊性变或坏死、合并多发腺体疾病、异位病灶及甲状腺疾病,同时排除技术及病灶功能差等因素,推测该患者MIBI双时相显像假阴性可能与癌细胞P-gP和(或)多药耐药相关蛋白表达阳性有关。
治疗与预后:由于PTC发病率低,目前还没有研究能够证实放化疗对PTC有确切的治疗效果[10],因此其主要治疗方式为手术切除。初次手术时最佳切除范围是肿瘤以及同侧甲状腺的整体切除,以防病灶被膜破损,减少术后复发[7]。PTC病灶切除10 min后,PTH与术前最高值相比下降50%以上提示功能亢进的甲状旁腺组织已被切除[7]。本研究中该例患者术中冰冻病理结果(右甲状旁腺)提示PTC倾向,行右侧甲状腺和右甲状旁腺切除,喉返神经探查,侧颈部淋巴结清扫术。PTC病灶切除30 min后复查PTH,为 624.1 pg/mL,与术前最高值相比下降>50%,说明病变组织已被切除。术后第6天复查PTH,为67.2 pg/mL,患者术后恢复良好,未见明显并发症。15%~30%的PTH患者在就诊时已经出现淋巴结转移,其中1/3的患者发生远处转移,通常转移至肺(40%)和肝(10%),少数情况下可转移至骨骼、胸膜、心包和胰腺[16]。本研究中该例患者被证实存在颈部淋巴结转移,未发现远处转移。有淋巴结和(或)远处转移的患者,术后复发率升高,主要表现为PTH和血钙的升高,因此要密切追踪患者术后PTH和血钙变化。由于PTC为惰性肿瘤,因此预后相对较好,PTC的5年生存率为78.3%,10年生存率为49.0%[3]。
本文探讨了一例99Tcm-MIBI显像阴性的PTC患者,并进行了较全面的文献复习。该类患者在临床工作中较为罕见,并且难以与甲状腺疾病及甲状旁腺良性病变进行鉴别,因此应该引起临床医师的高度重视。遇到此类患者时,需全面分析患者的临床特点及其实验室、影像学检查结果,在MIBI显像阴性时也不能完全排除PTC可能。一旦高度怀疑PTC,应积极采取手术等方法进行治疗。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 杨冬竹负责研究命题的提出、方法的建立、数据的分析、论文的撰写;龙再颖负责论文的修订、审核;单英丽、李燕萍负责数据的采集、现场工作的实施。
99Tcm-MIBI双时相平面显像阴性的散发性甲状旁腺癌一例及文献复习
99Tcm-MIBI dual phase planar imaging negative in patient with sporadic parathyroid carcinoma: a case report and literature review
-
摘要: 笔者报道了一例散发性甲状旁腺癌(PTC)99Tcm-甲氧基异丁基异腈(MIBI)显像阴性病例。PTC患者临床上表现为严重高钙血症引起的多个系统及器官的改变,需依赖于超声、甲状旁腺核素扫描(99Tcm-MIBI)、CT等检查明确定位后予以手术治疗,其中99Tcm-MIBI显像具有方法简便、灵敏度高的优势,被广泛应用于临床,但仍有少数病例存在检查结果阴性的可能,易造成患者误诊、漏诊。笔者通过文献复习加深了对99Tcm-MIBI显像阴性的PTC患者的认识:对于怀疑PTC,但99Tcm-MIBI显像阴性的患者,需考虑到可能存在假阴性,并应分析讨论导致假阴性可能的原因,进而结合其他临床特征进行综合判断,尽可能地减少患者的误诊及漏诊。Abstract: This paper reported a case of sporadic parathyroid carcinoma with negative 99Tcm-methoxyisobutylisonitrile (MIBI) imaging. The patient with parathyroid carcinoma is characterized by severe hypercalcemia which could cause pathological changes in multiple systems and different organs. It depends on ultrasound, parathyroid nuclide scan (99Tcm-MIBI) and CT examination to localize the position of lesions for further operation treatment. Among these examinations, parathyroid 99Tcm-MIBI imaging is widely used in clinical for its easy accessibility and high sensitivity. However, there are some cases presented with negative 99Tcm-MIBI imaging and is easy to be misdiagnosed. Through the literature review, the author deeply understood the negative 99Tcm-MIBI imaging of parathyroid carcinoma. For patients suspected of parathyroid carcinoma but with negative 99Tcm-MIBI imaging, the possibility of false negative need to be considered. In this specific clinical scenario, doctors should analyze its potential causes and make a comprehensive judgment through combining with other clinical characteristics, which could reduce the rate of misdiagnosis as much as possible.
-
Key words:
-
图 1 甲状旁腺癌患者(男性,41岁)影像学检查结果
Figure 1. Imaging findings of a 41 years old man with parathyroid carcinoma
图 2 甲状旁腺癌患者(男性,41岁)全身骨显像图
Figure 2. Whole body bone imaging in a 41 years old man with parathyroid carcinoma
-
[1] Obara T, Fujimoto Y. Diagnosis and treatment of patients with parathyroid carcinoma: an update and review[J]. World J Surg, 1991, 15(6): 738−744. DOI: 10.1007/BF01665308. [2] Sadler C, Gow KW, Beierle EA, et al. Parathyroid carcinoma in more than 1, 000 patients : a population-level analysis[J]. Surgery, 2014, 156(6): 1622−1630. DOI: 10.1016/j.surg.2014.08.069. [3] Cetani F, Pardi E, Marcocci C, et al. Parathyroid Carcinoma[J]. Front Horm Res, 2019, 51(3): 63−76. DOI: 10.1159/000491039. [4] Obara T, Okamoto T, Kanbe M, et al. Functioning parathyroid carcinoma: clinicopathologic features and rational treatment[J]. Semin Surg Oncol, 1997, 13(2): 134−141. DOI: 10.1002/(sici)1098-2388(199703/04)13:2<134::aid-ssu9>3.0.co;2-a. [5] 周建平, 田雨霖. 中国人原发性甲状旁腺功能亢进10年文献回顾(1995~2004年)[J]. 中国普通外科杂志, 2007, 16(1): 78−80. DOI: 10.3969/j.issn.1005-6947.2007.01.024.
Zhou JP, Tian YL. A 10-year literature review of Chinese primary hyperparathyroidism (1995~2004)[J]. Chin J Gen Surg, 2007, 16(1): 78−80. DOI: 10.3969/j.issn.1005-6947.2007.01.024.[6] Di Meo G, Sgaramella LI, Ferraro V, et al. Parathyroid carcinoma in multiple endocrine neoplasm type 1 syndrome: case report and systematic literature review[J]. Clin Exp Med, 2018, 18(4): 585−593. DOI: 10.1007/s10238-018-0512-7. [7] Rodrigo JP, Hernandez-Prera JC, Randolph GW, et al. Parathyroid cancer: an update[J]. Cancer Treat Rev, 2020, 86: 102012. DOI: 10.1016/j.ctrv.2020.102012. [8] Insogna KL. Primary hyperparathyroidism[J]. N Engl J Med, 2018, 379(11): 1050−1059. DOI: 10.1056/NEJMcp1714213. [9] Duan K, Mete Ö. Parathyroid carcinoma: diagnosis and clinical implication[J]. Turk Patoloji Derg, 2015, 31(Suppl 1): S80−97. DOI: 10.5146/tipath.2015.01316. [10] Christakis I, Bussaidy N, Clarke C, et al. Differrentiating atypical parathyroid neoplasm from prathyroid cancer[J]. Ann Surg Oncol, 2016, 23(9): 2889−2897. DOI: 10.1245/s10434-016-5248-6. [11] Cetani F, Frustaci G, Torregrossa L, et al. A nonfunctioning parathyroid carcinoma misdiagnosed as a follicular thyroid nodule[J/OL]. World J Surg Oncol, 2015, 13: 270[2019-06-10]. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4563849/pdf/12957_2015_Article_672.pdf. DOI: 10.1186/s12957-015-0672-9. [12] Schaapveld M, Jorna FH, Aben KK, et al. Incidence and prognosis of parathyroid gland carcinoma: a population-based study in The Netherlands estimating the preoperative diagnosis[J]. Am J Surg, 2011, 202(5): 590−597. DOI: 10.1016/j.amjsurg.2010.09.025. [13] Dy BM, Richards ML, Vazquez BJ, et al. Primary hyperparathyroidism and negative Tc99 sestamibi imaging: to operate or not?[J]. Ann Surg Oncol, 2012, 19(7): 2272−2278. DOI: 10.1245/s10434-012-2325-3. [14] Wu S, Hwang SS, Haigh PI. Influence of a negative sestamibi scan on the decision for parathyroid operation by the endocrinologist and surgeon[J]. Surgery, 2017, 161(1): 35−43. DOI: 10.1016/j.surg.2016.05.048. [15] Kao A, Shiau YC, Tsai SC, et al. Technetium-99m methoxyisobutylisonitrile imaging for parathyroid adenoma: relationship to P-glycoprotein or multidrug resistance-related protein expression[J]. Eur J Nucl Med Mol Imaging, 2002, 29(8): 1012−1015. DOI: 10.1007/s00259-002-0817-2. [16] Allen ME, Semrad A, Yang AD, et al. Parathyroid carcinoma survival: improvements in the era of intact parathyroid hormone monitoring?[J]. Rare Tumors, 2013, 5(1): e12. DOI: 10.4081/rt.2013.e12. -

 点击查看大图
点击查看大图
图(3)
计量
- 文章访问数: 3234
- HTML全文浏览量: 2269
- PDF下载量: 14