


-
乳腺癌是具有高度异质性的恶性肿瘤,其发病率和病死率均逐年递增,严重威胁女性的生命健康。磁共振弥散加权成像(diffusion weighted imaging,DWI)对乳腺癌的诊断及鉴别诊断具有较高的灵敏度及特异度。DWI是检测活体组织内水分子微观扩散运动的常用方法,可获取定量参数表观扩散系数(apparent diffusion coefficient,ADC)。研究表明,依据增强MRI的不同形态特征,乳腺癌又分为肿块型和非肿块型[1]。基础和临床研究结果表明,二者存在不同的病理生理学基础,在涉及肿瘤类型、级别和预后等方面均有差异,分类探讨很有意义[2]。目前有关DWI的ADC与雌激素受体(estrogen receptor,ER)、孕激素受体(progesterone receptor, PR) 、 人表皮生长因子受体2(human epidermal growth factor receptor 2,HER-2)和细胞增殖核抗原 Ki-67(简称 Ki-67)等乳腺癌分子生物学标志物的相关性研究仍较少,且多数未将肿瘤按强化类型进行分类,导致相关性存在一定争议[3]。本研究探讨不同强化类型乳腺癌的ADC与肿瘤生物学表征间的相关性,为术前预判肿瘤生物学特征提供依据。
-
选择2015年1月至2019年1月珠海市中西医结合医院收治的68例非特殊类型乳腺癌女性患者,年龄34~72(48.5±4.7)岁;其中肿块型49例、非肿块型19例。病理组织分级:Ⅰ级13例、Ⅱ级28例、Ⅲ级27例,病灶最大直径为0.9~10.4(4.4±1.2) cm。纳入标准:①行乳腺MRI检查前未进行任何治疗;②经手术或穿刺活检病理结果证实为乳腺癌;③病灶最大直径线可满足ADC的稳定测量,多数病灶≥1 cm;④ MRI图像清晰,可供分析。排除标准:① MRI图像不清晰;②不愿意配合研究者;③严重心、肝、肾功能障碍者。所有患者检查前均签署了知情同意书。
-
使用美国GE公司1.5 T Sigma HDx MRI检查仪,乳腺8通道相控阵表面线圈。患者取俯卧位,双乳自然悬垂于线圈,行动态增强MRI扫描。采用容积内插体部检查序列(VIBE)轴面扫描,参数:重复时间6.53 ms、回波时间3.2 ms、层厚2 mm、翻转角15°、视野320 mm×320 mm、矩阵410×320。对比剂采用Gd-DTPA(北京北陆药业股份有限公司,批准文号:国药准字H20013088),注射剂量为0.1 mmoL/kg,流率为2 mL/s,团注结束后以相同速率注入20 mL生理盐水冲管。注入对比剂后行横轴位DWI,采用单次激发平面回波成像(SS-EPI)采集技术:弥散加权因子b值取0 s/mm2和1000 s/mm2,重复时间5700 ms、回波时间78 ms、视野 33 cm、激励次数(NEX)6、层厚 4 mm、间隔1、矩阵130×128。
-
采用美国GE 公司ADW 4.4自带软件对DWI图像进行后处理,软件自动生成ADC图,在ADC图上肿瘤实性部分选取ROI直接测量ADC,至少测量3个ADC,取平均值作为病灶的ADC。ROI的选取尽可能避开囊变、出血、坏死及乳腺X射线摄影提示钙化的区域。多发病灶选取最大病灶进行测量。
图像分析均由放射科两位具有10年及以上工作经验的医师共同完成。意见不一致时,由二者讨论决定,必要时与另一位高年资医师协商解决。
-
术后肿瘤组织经4%中性缓冲甲醛溶液固定,组织脱水、二甲苯透明、石蜡包埋后,4 μm连续切片,按常规免疫组化SP法进行ER、PR、HER-2和Ki-67检测。采用许良中和杨文涛[4]的半定量计分方法将染色强度分为4个等级,由浅到深依次记为0~3分。同时在高倍光学显微镜下根据着色的阳性细胞百分比计分:≤5%为0分、5%~25%为1分、25%~50%为2分、≥50%为3分。阳性强度总评分=染色强度×阳性细胞百分比,其中0~1分(−)、2~3分(+)均记为阴性;4~6分(++)、>6分(+++)均记为阳性。
-
依据免疫组化检测结果,将乳腺癌分为以下4种分子亚型。① Luminal A型:ER(+)、PR(+)、HER-2(−)、Ki-67低表达(≤14%)。② Luminal B型:ER(+)、PR(+)、HER-2(−)、Ki-67高表达(>14%);ER、PR、HER-2均为(+),Ki-67任意表达。③ HER-2过表达型:ER(−)、PR(−)、HER-2(+)、Ki-67任意表达。④三阴性乳腺癌(triple negative breast cancer,TNBC) :ER、PR和HER-2均为(−)、Ki-67任意表达。
-
采用SPSS 17.0软件对数据进行统计学分析。对符合正态分布且方差齐的数据用均数±标准差(
${\bar x} $ ± s)表示,不同强化类型乳腺癌、不同生物学标志物及不同分子亚型乳腺癌的ADC比较采用t检验,采用Spearman等级相关性分析ADC与生物学标志物和分子亚型的相关性。P<0.05为差异有统计学意义。 -
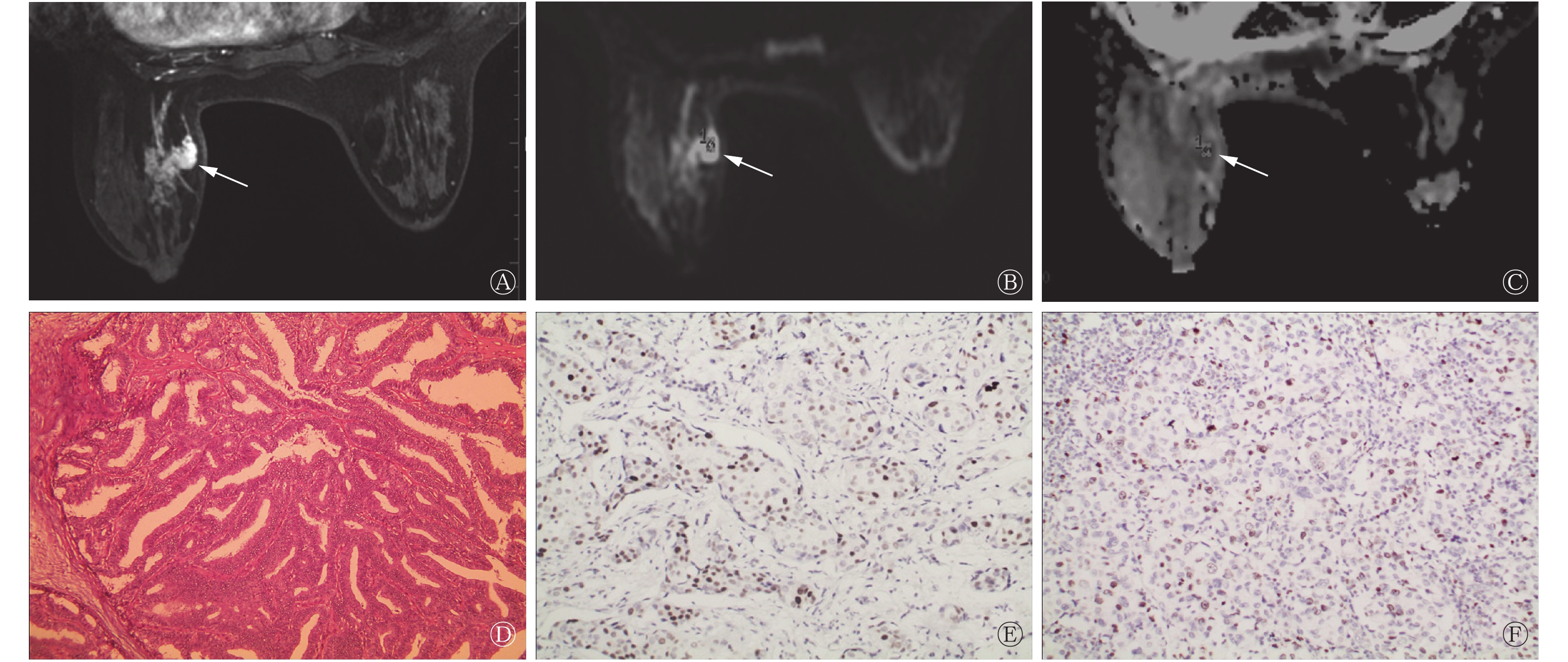
肿块型乳腺癌患者的ADC为(0.95±0.13)×103 mm2/s,显著低于非肿块型的(1.03±0.12)×103 mm2/s,且差异有统计学意义(t=2.193,P=0.023)。典型病例的MRI图像见图1和图2。
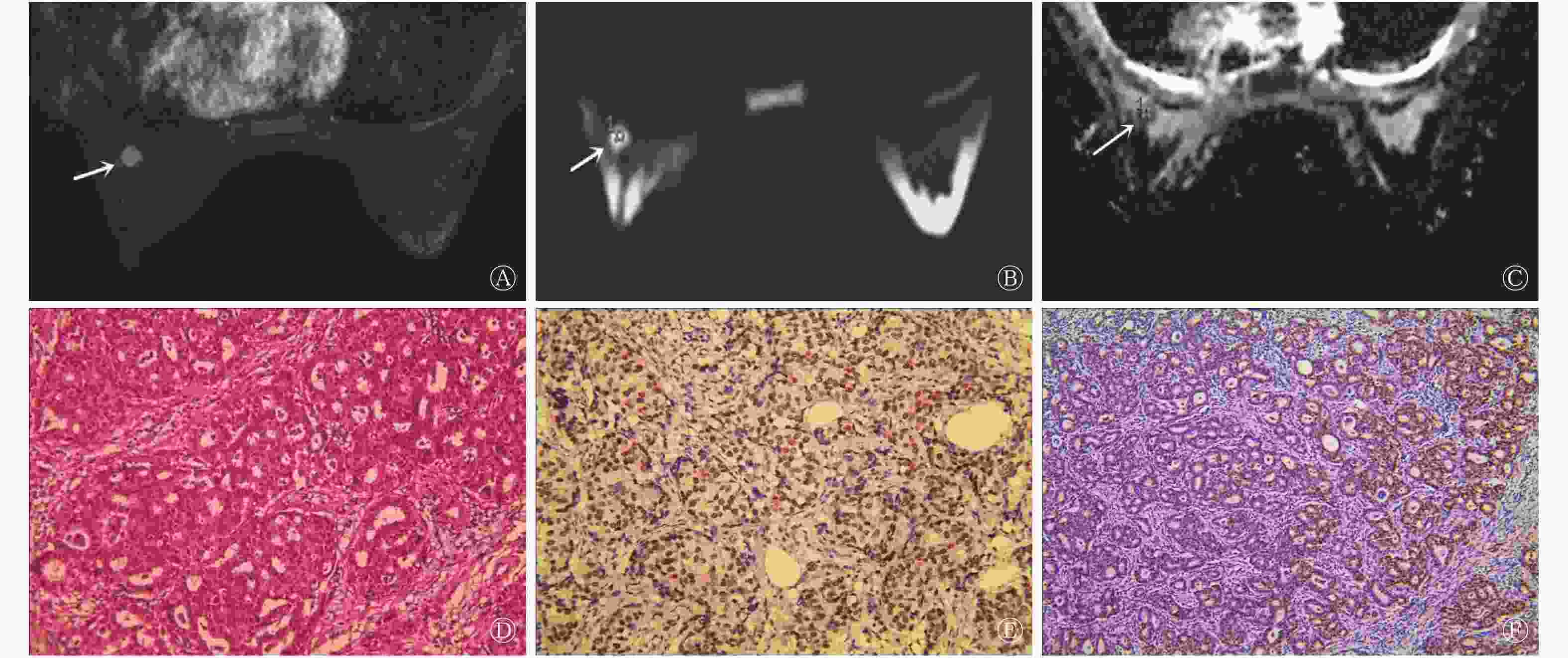
图 1 肿块型乳腺癌患者(女性,40岁)的MRI、病理及免疫组化图
Figure 1. MRI,pathology and immunohistochemical images of breast cancer patient(female,40 years old)
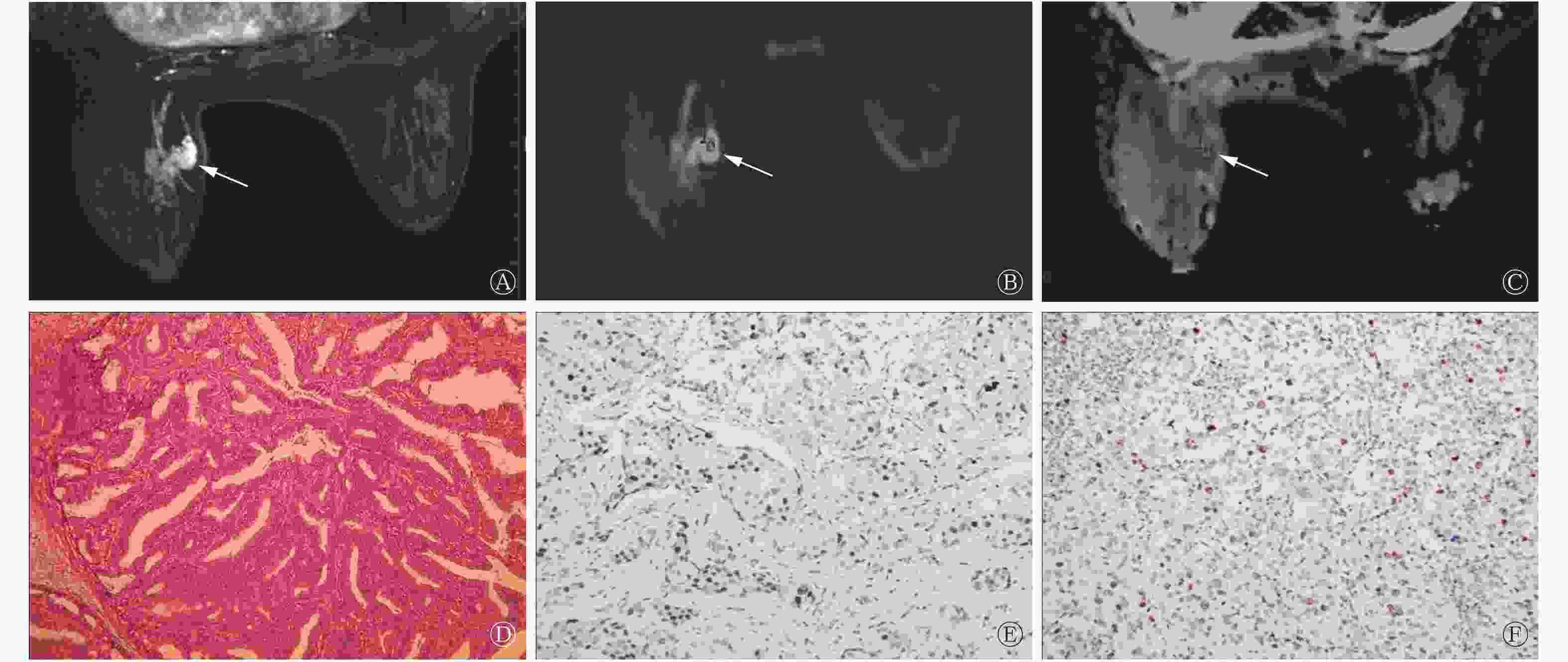
图 2 非肿块型乳腺癌患者(女性,51岁)的MRI、病理及免疫组化图
Figure 2. MRI,pathology and immunohistochemical images of breast cancer(female,51 years old)
-
在19例非肿块型乳腺癌患者中,ER(−)、PR(−)、Ki-67>14%者的ADC显著低于ER(+)、PR(+)、Ki-67≤14%者 (t =2.742、2.054、2.323,均 P<0.05);HER-2过表达型患者的ADC高于Luminal A 型、Luminal B 型和TNBC患者,且差异均有统计学意义(t=2.515、2.336、2.721,均P<0.05)。在49例肿块型乳腺癌患者中,ER(−)、Ki-67>14%者的ADC显著低于ER(+)、Ki-67≤14%者(t=3.291、2.183,均P<0.05),HER-2过表达型患者的ADC高于Luminal A 型、Luminal B 型和TNBC患者,且差异均有统计学意义(t =2.493、2.453、2.512,均P <0.05)。其他具体数据见表1。
生物学标志物及
分子亚型分类 病灶数 ADC t 值 P 值 肿块型 非肿块型 ER − 27 0.93±0.12 0.99±0.14 2.038 0.048 + 41 1.02±0.14a 1.09±0.11a 2.517 0.014 PR − 24 0.95±0.12 1.00±0.11 1.505 0.139 + 44 0.98±0.16a 1.03±0.13 2.045 0.042 HER-2 − 39 0.95±0.13 0.98±0.12 1.061 0.293 + 29 0.97±0.15 1.02±0.14 1.306 0.195 Ki-67 ≤14% 35 0.98±0.16 1.03±0.16 1.392 0.169 >14% 33 0.90±0.12b 0.97±0.13b 2.272 0.026 分子亚型 Luminal A型 15 0.92±0.09c 0.95±0.13c 0.678 0.500 Luminal B型 33 0.95±0.11c 0.99±0.12c 1.103 0.279 HER-2过表达型 9 1.05±0.13 1.09±0.15 0.993 0.329 TNBC 11 0.94±0.10c 0.97±0.12c 0.639 0.531 注:表中,−:阴性;+:阳性。a:与ER、PR(−)比较,差异均有统计学意义(t=2.054~3.291,均P<0.05);b: 与≤14%比较,差异均有统计学意义(t=2.183、2.232,均P<0.05);c : 与HER-2过表达型比较,差异均有统计学意义(t =2.336~2.515,均 P<0.05)。ADC:表观扩散系数;ER:雌激素受体;PR:孕激素受体:HER-2:人表皮生长因子受体2;Ki-67:细胞增殖核抗原Ki-67;TNBC:三阴性乳腺癌 表 1 68例乳腺癌患者不同强化类型、不同生物学标记物及分子亚型的ADC比较(
$ \scriptstyle \bar x \pm s$ Table 1. Comparison of ADC of 68 patients with different types of enhancement, different biomarkers and molecular subtypes (
$\scriptstyle \bar x \pm s$ -
由表2可知,肿块型乳腺癌的ADC与ER(+)、PR(+)表达呈正相关,与Ki-67表达水平呈负相关;非肿块型乳腺癌的ADC与ER(+)表达呈正相关,与Ki-67表达水平呈负相关。
不同类型的检验值 ER(+) PR(+) HER-2 Ki-67 肿块型乳腺癌的ADC r值 0.394 0.360 −0.232 −0.407 P值 0.024 0.044 0.178 0.016 非肿块型乳腺癌的ADC r值 0.371 0.303 −0.214 −0.397 P值 0.036 0.061 0.126 0.027 注:表中,ADC:表观扩散系数;ER:雌激素受体;PR:孕激素受体:HER-2:人表皮生长因子受体2;Ki-67:细胞增殖核抗原Ki-67 表 2 不同强化类型乳腺癌的ADC与生物学标志物的相关性
Table 2. Correlation between apparent diffusion coefficient and biomarkers in different enhancement types of breast cancer
-
ER和PR为存在于正常腺体内的激素依赖型受体,其高表达表明对内分泌治疗敏感,预后更好。ER与PR间有一定的相关性,但也各自独立起作用,研究表明,ER、PR均为阳性患者内分泌治疗的反应率比ER(+)、PR(−)的患者高30%[5]。HER-2是一种原癌基因,在正常乳腺组织中低表达或不表达,HER-2蛋白过表达参与维持肿瘤恶化发展的多条通路,包括生长的自主性、持续的血管形成、细胞分裂能力增加和浸润能力增强,HER-2过表达的肿瘤预后差,可作为评估乳腺癌患者预后的独立指标[6]。Ki-67是与细胞增殖相关的核蛋白,是检测肿瘤增殖活性的可靠指标[7],其能够发现病理分级较低却具有高度增殖能力的恶性肿瘤,从而更准确地反映肿瘤性质[8],并可作为肿瘤分级的独立指标。Ki-67高表达患者行蒽环类联合紫杉类新辅助化疗的效果更好。Juanjuan等[9]研究结果表明,不同分子亚型的乳腺癌临床特征各异,治疗的反应性、肿瘤复发模式及生存情况不相同。Luminal A型是最常见的分子亚型,通常见于早期乳腺癌,对内分泌治疗敏感,预后较好;Luminal B型也对内分泌治疗敏感,但其化疗敏感性易变,且无明显集中的临床分期;HER-2过表达型乳腺癌多为晚期,恶性程度高;TNBC常见于晚期、年轻和绝经前女性患者,易复发转移。
-
本研究结果显示,肿块型乳腺癌的ADC低于非肿块型乳腺癌,与文献报道一致[10]。分析原因可能在于非肿块型乳腺癌中部分为导管原位癌,病变导管基底膜完整,水分子受限不明显;此外肿块型乳腺癌病灶细胞致密、纤维间质成分减少、细胞外间隙缩小,而非肿块型乳腺癌肿瘤细胞密度相对低、纤维间质多、水分子受限不明显,且肿瘤细胞内可能夹杂正常腺体、脂肪组织、纤维组织等,故ADC相对偏高。
-
本研究结果显示,肿块型乳腺癌ER(−)、PR(−)和Ki-67>14%者的ADC均低于非肿块型,差异有统计学意义,与Aydin等[11]研究结果相似。在肿块型乳腺癌中,ADC与ER(+)、PR(+)表达呈正相关;在非肿块型乳腺癌中,ADC与ER(+)表达呈正相关,与PR(+)表达不相关。Kamitani等[12]认为,ER、PR受体表达对血管通路造成抑制,导致灌注减低,且与阳性肿瘤细胞密度较高相一致。有研究发现,HER-2与ADC未表现出明显相关性(P>0.05)[13],本研究也得出类似结果。理论上讲,HER-2表达率越高,细胞密度越大,ADC越低。Jeh等[14]研究发现,ADC与HER-2具有相关性。以上研究结果的差异可能是因为ADC受多种因素的影响,除了细胞密度,还有其他方面与之相对的因素,如肿瘤血管的高灌注、新生血管通透性的增加及血管源性水肿等都可以导致细胞外间隙的增大,使ADC增高。Choi等[15]对乳腺癌的ADC与Ki-67的高低表达进行研究,结果表明,ADC与Ki-67呈负相关。本研究结果亦显示不论哪种强化类型,肿瘤ADC均与Ki-67表达水平呈负相关。这与Ki-67高表达提示肿瘤细胞增殖旺盛和ADC降低相吻合。
Youk等[16]比较各亚型乳腺癌的平均ADC,发现ER(+)和HER-2过表达型的平均ADC比TNBC的平均ADC低。本研究得出,肿块型和非肿块型乳腺癌中,与HER-2过表达型比较,Luminal A型、Luminal B型及TNBC患者的ADC均显著降低(P<0.05),考虑可能与测量时ROI放置位置及包括范围有关,本研究ROI放置于肿瘤实性部分,避开了中心坏死区。Uematsu等[17]认为,肿瘤中心在T2加权成像的高信号与TNBC有显著相关性,病理结果证实该表现与肿瘤内部坏死有关,坏死区域细胞密度减低,水分子更易扩散,ADC相应增高。郜莹莹等[18]研究结果也得出了TNBC组病灶的ADC较HER-2过表达组偏高,这提示TNBC较HER-2过表达型肿瘤内部更易坏死。
综上所述,本研究将乳腺癌按照不同强化方式进行分类,得出肿块型乳腺癌的ADC较非肿块型低,肿瘤ADC与分子生物学表征具有一定的相关性,且因强化类型不同相关性亦略有差异,据此可初步预判肿瘤分子生物学特征,为临床个体化治疗提供依据。
利益冲突 本研究由署名作者按以下贡献声明独立开展,不涉及任何利益冲突。
作者贡献声明 石琴负责命题的提出与设计、数据的获取与分析、论文的撰写与最终版本的修订;张文负责命题的设计、数据的获取与分析;付志明、卢晓娟、贝金玲负责试验的实施、数据的获取。
肿块型与非肿块型乳腺癌MRI弥散加权成像表观扩散系数与分子生物学指标的相关性研究
Study on the correlation between MRI diffusion-weighted imaging apparent diffusion coefficient and molecular biological indexes of mass-like and non-mass-like breast cancer
-
摘要:
目的 探讨肿块型与非肿块型乳腺癌磁共振弥散加权成像(DWI)表观扩散系数(ADC)与肿瘤分子生物学特征之间的相关性。 方法 回顾性分析2015年1月至2019年1月珠海市中西医结合医院收治的68例经病理学确诊的乳腺癌患者术前磁共振的DWI资料,患者均为女性,年龄34~72(48.5±4.7)岁;其中肿块型49例,非肿块型19例。采用免疫组化法测定雌激素受体(ER)、孕激素受体(PR)、人表皮生长因子受体2(HER-2)和细胞增殖核抗原Ki-67(简称Ki-67)的表达,肿块型与非肿块型乳腺癌、不同生物学标记物及不同分子亚型乳腺癌的ADC比较采用t检验。采用Spearman等级相关性分析ADC与生物学标志物和分子亚型的相关性。 结果 肿块型乳腺癌的ADC低于非肿块型[(0.95±0.13)×103 mm2/s vs.(1.03±0.12)×103 mm2/s],差异有统计学意义(t=2.193,P=0.023)。19例非肿块型乳腺癌中ER(−)、PR(−)、Ki-67>14%者的ADC低于ER(+)、PR(+)、Ki-67≤14%者(t =2.742、2.054、2.323,均 P<0.05),HER-2过表达型的ADC高于其他分子亚型,且差异均有统计学意义(t=2.515、2.336、2.721,均P<0.05)。49例肿块型乳腺癌中ER(−)、Ki-67>14%者的ADC低于ER(+)、Ki-67≤14%者(t=3.291、2.183,均 P<0.05),HER-2过表达型的ADC高于其他分子亚型,且差异均有统计学意义(t=2.493、2.453、2.512,均P<0.05)。肿块型乳腺癌患者的ADC与ER(+)、PR(+)表达呈正相关,与Ki-67表达水平呈负相关,且差异均有统计学意义(r=0.394、0.360、−0.407,均P<0.05);非肿块型乳腺癌患者的ADC与ER(+)表达呈正相关,与Ki-67表达水平呈负相关,且差异均有统计学意义(r=0.371、−0.397,均P<0.05)。 结论 非肿块型乳腺癌的ADC高于肿块型乳腺癌,肿瘤ADC与分子生物学表征具有一定的相关性。 Abstract:Objective To investigate the correlation of apparent diffusion coefficient (ADC) value of MRI diffusion-weighted imaging (DWI) in breast cancer of mass-like and non-mass-like breast cancer with tumor molecular biomarkers. Methods DWI of 68 breast cancer patients admitted to Zhuhai Integrative Medicine Hospital from January 2015 to January 2019 before operation was retrospectively analyzed, all patients were female, aged 34−72 (48.5±4.7) years, 49 case mass-like and 19 case non-mass-like breast cancer patients . Estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER-2) and cancer antigen were expressed by immunohistochemical assay, and the molecular subtypes were evaluated. T-test was used to compared the ADC of tumor type and non-tumor type breast cancer, different biological markers and different molecular subtypes of breast cancer. The correlation between ADC values and molecular markers and subtypes was analyzed by Spearman level correlation. Results The ADC value of mass-like breast cancer was significantly lower than that of non-mass-like breast cancer ((0.95±0.13)×103 mm2/s vs. (1.03±0.12)×103 mm2/s, t=2.193, P=0.023). The ADC values of 19 non-mass-like breast cancer patients with ER(−), PR(−) and Ki-67>14% were significantly lower than those of ER(+), PR(+) and Ki-67≤14% (t=2.742, 2.054, 2.323; all P<0.05), and patients with the HER-2 overexpression type was higher than other molecular subtypes (t=2.515, 2.336, 2.721; all P<0.05). The ADC values of 49 mass-like breast cancer patients with ER(−) and Ki-67>14% were significantly lower than those of ER(+) and Ki-67≤14% (t=3.291, 2.183; both P<0.05) and patients with the HER-2 overexpression type was higher than other molecular subtypes(t=2.493, 2.453, 2.512; all P<0.05). The ADC value of mass-like breast cancer was positively correlated with the negative expression of ER (+) and PR (+), and the expression level of Ki-67 (r=0.394, 0.360, −0.407; all P<0.05). The ADC value of mass-like breast cancer was positively correlated with ER (+) negative expression and Ki-67 expression (r=0.371, −0.397; both P<0.05). Conclusion The ADC value of non-mass-like breast cancer is higher than that of mass-like, and the ADC value has a good correlation with the expression of molecular biological characterization. -
图 1 肿块型乳腺癌患者(女性,40岁)的MRI、病理及免疫组化图
Figure 1. MRI,pathology and immunohistochemical images of breast cancer patient(female,40 years old)
图 2 非肿块型乳腺癌患者(女性,51岁)的MRI、病理及免疫组化图
Figure 2. MRI,pathology and immunohistochemical images of breast cancer(female,51 years old)
表 1 68例乳腺癌患者不同强化类型、不同生物学标记物及分子亚型的ADC比较(
$ \scriptstyle \bar x \pm s$ Table 1. Comparison of ADC of 68 patients with different types of enhancement, different biomarkers and molecular subtypes (
$\scriptstyle \bar x \pm s$ 生物学标志物及
分子亚型分类 病灶数 ADC t 值 P 值 肿块型 非肿块型 ER − 27 0.93±0.12 0.99±0.14 2.038 0.048 + 41 1.02±0.14a 1.09±0.11a 2.517 0.014 PR − 24 0.95±0.12 1.00±0.11 1.505 0.139 + 44 0.98±0.16a 1.03±0.13 2.045 0.042 HER-2 − 39 0.95±0.13 0.98±0.12 1.061 0.293 + 29 0.97±0.15 1.02±0.14 1.306 0.195 Ki-67 ≤14% 35 0.98±0.16 1.03±0.16 1.392 0.169 >14% 33 0.90±0.12b 0.97±0.13b 2.272 0.026 分子亚型 Luminal A型 15 0.92±0.09c 0.95±0.13c 0.678 0.500 Luminal B型 33 0.95±0.11c 0.99±0.12c 1.103 0.279 HER-2过表达型 9 1.05±0.13 1.09±0.15 0.993 0.329 TNBC 11 0.94±0.10c 0.97±0.12c 0.639 0.531 注:表中,−:阴性;+:阳性。a:与ER、PR(−)比较,差异均有统计学意义(t=2.054~3.291,均P<0.05);b: 与≤14%比较,差异均有统计学意义(t=2.183、2.232,均P<0.05);c : 与HER-2过表达型比较,差异均有统计学意义(t =2.336~2.515,均 P<0.05)。ADC:表观扩散系数;ER:雌激素受体;PR:孕激素受体:HER-2:人表皮生长因子受体2;Ki-67:细胞增殖核抗原Ki-67;TNBC:三阴性乳腺癌  下载: 导出CSV
下载: 导出CSV
表 2 不同强化类型乳腺癌的ADC与生物学标志物的相关性
Table 2. Correlation between apparent diffusion coefficient and biomarkers in different enhancement types of breast cancer
不同类型的检验值 ER(+) PR(+) HER-2 Ki-67 肿块型乳腺癌的ADC r值 0.394 0.360 −0.232 −0.407 P值 0.024 0.044 0.178 0.016 非肿块型乳腺癌的ADC r值 0.371 0.303 −0.214 −0.397 P值 0.036 0.061 0.126 0.027 注:表中,ADC:表观扩散系数;ER:雌激素受体;PR:孕激素受体:HER-2:人表皮生长因子受体2;Ki-67:细胞增殖核抗原Ki-67
下载: 导出CSV
-
[1] Park EK, Cho KR, Bo Seo K, et al. Additional Value of Diffusion-Weighted Imaging to Evaluate Prognostic Factors of Breast Cancer: Correlation with the Apparent Diffusion Coefficient[J/OL]. Iran J Radiol, 2016, 13(1): e33133[2019-03-07]. https://www.ncbi.nlm.nih.gov/pubmed/27127582. DOI: 10.5812/iranjradiol.33133. [2] 杨义文, 胡春洪, 朱默, 等. MRI表观扩散系数联合动态增强TIC类型对肿块型浆细胞性乳腺炎及乳腺癌的鉴别诊断价值[J]. 磁共振成像, 2019, 10(7): 530−534. DOI: 10.12015/issn.1674−8034.2019.07.010.
Yang YW, Hu CH, Zhu M, et al. The differential diagnosis value of MRI apparent diffusion coefficient value combined with dynamic contrast enhanced MRI time-intensity curve type for mass plasma cell mastitis and breast cancer[J]. Chin J Magn Reson Imaging, 2019, 10(7): 530−534. DOI: 10.12015/issn.1674−8034.2019.07.010.[3] Belli P, Costantini M, Bufi E, et al. Diffusion magnetic resonance imaging in breast cancer characterisation: correlations between the apparent diffusion coefficient and major prognostic factors[J]. Radiol Med, 2015, 120(3): 268−276. DOI: 10.1007/s11547−014−0442−8. [4] 许良中, 杨文涛. 免疫组织化学反应结果的判断标准[J]. 中国癌症杂志, 1996, 6(4): 229−231. DOI: 10.19401/j.cnki.1007−3639.1996.04.001.
Xu LZ, Yang WT. Criteria for the outcome of immunohistochemical reactions[J]. China Oncol, 1996, 6(4): 229−231. DOI: 10.19401/j.cnki.1007−3639.1996.04.001.[5] 刘静, 钟玲, 陈庆秋, 等. 乳腺癌发生过程中ER、PR、HER-2及WT1蛋白表达变化的研究[J]. 临床肿瘤学杂志, 2019, 24(8): 722−726. DOI: 10.3969/j.issn.1009−0460.2019.08.010.
Liu J, Zhong L, Chen QQ, et al. Changes of ER, PR, HER-2 and WT1 protein expression during the development of breast cancer[J]. Chin Clin Oncol, 2019, 24(8): 722−726. DOI: 10.3969/j.issn.1009−0460.2019.08.010.[6] Bae MS, Seo M, Kim KG, et al. Quantitative MRI morphology of invasive breast cancer: correlation with immunohistochemical biomarkers and subtypes[J]. Acta Radiol, 2015, 56(3): 269−275. DOI: 10.1177/0284185114524197. [7] María del RTS, Teresa SM, Petit A, et al. Digital quantification of KI-67 in breast cancer[J]. Virchows Archiv, 2019, 474(2): 169−176. DOI: 10.1007/s00428−018−2481−3. [8] Alexey S, Paola C, Yun-Woo C, et al. Can diffusion-weighted imaging predict tumor grade and expression of Ki-67 in breast cancer? A multicenter analysis[J]. Breast Cancer Res, 2018, 20(1): 58−62. DOI: 10.1186/s13058−018−0991−1. [9] Juanjuan L, Yue X, Qi W, et al. Outcomes of patients with inflammatory breast cancer by hormone receptor- and HER2-defined molecular subtypes: A population-based study from the SEER program[J]. Oncotarget, 2017, 8(30): 49370−49379. DOI: 10.18632/oncotarget.17217. [10] 李芹, 牛庆亮, 杜汉旺, 等. 肿块型与非肿块型乳腺癌ADC值、Ki67指数的对比分析[J]. 中国临床医学影像杂志, 2018, 29(1): 11−13, 27. DOI: 10.3969/j.issn.1008−1062.2018.01.004.
Li Q, Niu QL, Du HW, et al. Comparative analysis of ADC value and Ki67 index in mass-like and non-mass-like breast cancer[J]. J China Clin Med Imaging, 2018, 29(1): 11−13, 27. DOI: 10.3969/j.issn.1008−1062.2018.01.004.[11] Aydin H, Guner B, Esen Bostanci I, et al. Is there any relationship between adc values of diffusion-weighted imaging and the histopathological prognostic factors of invasive ductal carcinoma?[J]. Br J Radiol, 2018, 91(1084): 20170705. DOI: 10.1259/bjr.20170705. [12] Kamitani T, Matsuo Y, Yabuuchi H, et al. Correlations between apparent diffusion coefficient values and prognostic factors of breast cancer[J]. Magn Reson Med Sci, 2013, 12(3): 193−199. DOI: 10.2463/mrms.2012−0095. [13] Trihia H, Murray S, Price K, et al. Ki-67 expression in breast carcinoma: Its association with grading systems, clinical parameters, and other prognostic factors-A surrogate marker?[J]. Cancer, 2003, 97(5): 1321−1331. DOI: 10.1002/cncr.11188. [14] Jeh SK, Kim SH, Kim HS, et al. Correlation of the apparent diffusion coefficient value and dynamic magnetic resonance imaging findings with prognostic factors in invasive ductal carcinoma[J]. J Magn Reson Imaging, 2011, 33(1): 102−109. DOI: 10.1002/jmri.22400. [15] Choi SY, Chang YW, Park HJ, et al. Correlation of the apparent diffusion coefficiency values on diffusion-weighted imaging with prognostic factors for breast cancer[J/OL]. Br J Radiol, 2012, 85(1016): e474-479[2019-03-07]. https://www.ncbi.nlm.nih.gov/pubmed/22128125. DOI: 10.1259/bjr/79381464. [16] Youk JH, Son EJ, Chung J, et al. Triple-negative invasive breast cancer on dynamic contrast-enhanced and diffusion-weighted MR imaging: comparison with other breast cancer subtypes[J]. Eur Radiol, 2012, 22(8): 1724−1734. DOI: 10.1007/s00330−012−2425−2. [17] Uematsu T, Kasami M, Yuen S. Triple-Negative Breast Cancer: Correlation Between MR Imaging and Pathologic Findings[J]. Radiology, 2009, 250(3): 638−647. DOI: 10.1148/radiol.2503081054. [18] 郜莹莹, 刘艳, 杨爱梅. 三阴性乳腺癌与HER-2过表达型乳腺癌MRI动态增强特征及ADC值分析[J]. 实用放射学杂志, 2014, 30(4): 606-609. DOI: 10.3969/j.issn.1002-1671.2014.04.016.
Gao YY, Liu Y, Yang AM. DCE-MRI features and ADC value analysis in triple-negative breast cancer and HER-2 overexpression subtype of breast cancer[J]. J Pract Radiol, 2014, 30(4): 606-609. DOI: 10.3969/j.issn.1002-1671.2014.04.016. -

 点击查看大图
点击查看大图

计量
- 文章访问数: 3599
- HTML全文浏览量: 2133
- PDF下载量: 7
